After splenectomy How is the blood picture changes in hyperslenism
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the complete answer:
Blood Picture Changes After Splenectomy in Hypersplenism
What is Hypersplenism? (Before Splenectomy)
Hypersplenism is defined by the triad of:
- Splenomegaly
- Cytopenia(s) - reduction in one or more blood cell lines (anemia, leukopenia, thrombocytopenia, or all three = pancytopenia)
- Normal or hyperplastic bone marrow (reactive compensation)
The spleen causes cytopenias through two main mechanisms: (a) sequestration and destruction of blood cells (especially in congestive splenomegaly), and (b) immune-mediated destruction. Up to 80% of the platelet pool can be sequestered in a massively enlarged spleen. Red cells may appear spherocytic on smear due to membrane loss during prolonged transit through congested splenic cords. Reticulocyte production is increased but may be blunted by splenic sequestration of reticulocytes.
Blood Picture Changes After Splenectomy
Splenectomy removes the organ responsible for both filtration and destruction, producing predictable and characteristic changes in the peripheral blood smear and counts:
1. Red Blood Cell Changes
| Finding | Mechanism |
|---|---|
| Howell-Jolly bodies | Nuclear chromatin remnants (DNA fragments) no longer removed by the absent spleen. Single Howell-Jolly bodies per cell are the hallmark of post-splenectomy. |
| Siderocytes (Pappenheimer bodies) | Iron-containing granules in RBCs that the spleen would normally pit out |
| Target cells (codocytes) | Increased membrane-to-hemoglobin ratio, accumulate without splenic remodeling |
| Acanthocytes / burr cells | Abnormal membrane projections, minor finding |
| Nucleated RBCs (normoblasts) | Spleen normally removes these; escape into circulation post-splenectomy |
| Rise in hemoglobin / resolution of anemia | The pre-op hemolytic/sequestration anemia corrects as red cell survival increases |
| Increased reticulocyte count (initially) | Reflects the previously stimulated marrow; normalizes over time |
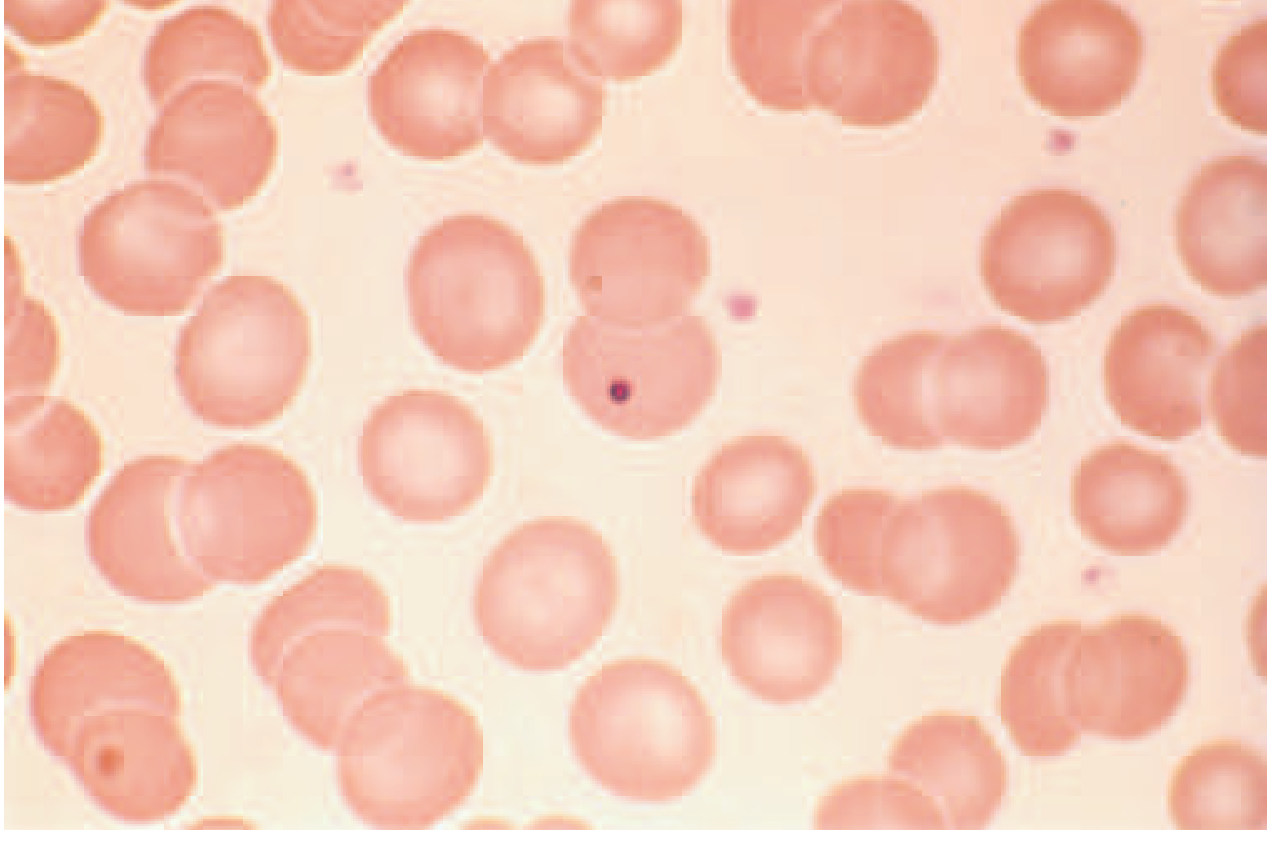
Howell-Jolly bodies: tiny nuclear remnants that the spleen normally removes via "pitting." Their appearance on smear is the classic marker of asplenia/post-splenectomy state. - Harrison's Principles of Internal Medicine 22E, Figure 65-17
2. Platelet Changes
- Thrombocytosis - the most dramatic early change. Platelet count rises within 2 days of surgery. In patients who had severe pre-op thrombocytopenia, the peak may not occur for several weeks.
- Counts can transiently rise to >1,000 x 10⁹/L (reactive thrombocytosis), raising concern for thromboembolism.
- This is especially relevant in myeloproliferative disorders and splenomegaly patients - risk of portal vein thrombosis post-splenectomy may reach 50%.
3. White Blood Cell Changes
- Leukocytosis develops within 1 day post-splenectomy and may persist for several months.
- The WBC rise reflects both the release of sequestered leukocytes and removal of the spleen's role in WBC clearance.
- Predominantly a neutrophilia in the early post-op period.
Summary Table
| Parameter | In Hypersplenism (Pre-op) | After Splenectomy |
|---|---|---|
| Hemoglobin | Low (anemia) | Rises toward normal |
| Platelets | Low (thrombocytopenia) | Rises - thrombocytosis |
| WBC | Low (leukopenia) | Rises - leukocytosis |
| Reticulocytes | Increased (suppressed by sequestration) | Initially high, then normalizes |
| Peripheral smear | Spherocytes possible | Howell-Jolly bodies, siderocytes, target cells, nucleated RBCs |
| Bone marrow | Hyperplastic (compensatory) | Returns toward normal |
Important Clinical Notes
- Granulocytopenia reversal is not always sustained after splenectomy - Harrison's notes this is less reliable than platelet or hemoglobin responses.
- For ITP, long-term platelet response is seen in ~80% of patients after splenectomy.
- For chronic hemolytic anemia (e.g., hereditary spherocytosis), success rates for hemoglobin normalization are 90-100%.
- The key marker of functional asplenia at any time is the presence of Howell-Jolly bodies on peripheral smear.
- Lifelong susceptibility to encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae type B, Neisseria meningitidis) follows splenectomy - vaccination and prophylactic antibiotics are required.
Sources: Harrison's Principles of Internal Medicine 22E; Schwartz's Principles of Surgery 11E; Bailey & Love's Short Practice of Surgery 28E; Henry's Clinical Diagnosis and Management by Laboratory Methods
Trend of platelet and wbc
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I have everything needed. Here is the focused answer on the post-splenectomy trend of platelets and WBC:
Post-Splenectomy Trend of Platelets and WBC
Platelets
| Time Point | What Happens |
|---|---|
| Day 1-2 | Platelet count begins to rise - this is the earliest and most reliable sign |
| Days 2-7 | Rapid rise; initial response (defined as a rise within several days) is seen in most patients |
| Weeks 1-4 | Counts continue to climb; may not peak for several weeks if the patient had severe pre-op thrombocytopenia |
| Peak | Can reach >1,000 x 10⁹/L (reactive thrombocytosis) - clinically important as it raises thromboembolism risk |
| Long-term | Normalizes in most patients; long-term platelet response sustained in ~80% of ITP patients; ~60% achieve long-term remission |
Key point: The more severe the pre-operative thrombocytopenia, the more delayed the peak platelet response. This is because the bone marrow needs time to ramp up megakaryocyte production after the chronic sequestration load is removed.
Watch for portal vein thrombosis in patients with splenomegaly + myeloproliferative disorders - risk can be as high as 50% post-splenectomy due to the thrombocytotic surge.
White Blood Cells (WBC)
| Time Point | What Happens |
|---|---|
| Within 1 day | WBC rises - this is one of the earliest post-op changes |
| Days 1-7 | Leukocytosis (predominantly neutrophilia) is well established |
| Weeks to months | Elevation may persist for several months |
| Long-term | Eventually returns toward normal baseline |
Key point: WBC normalizes more gradually than platelets. The rise reflects:
- Release of previously sequestered leukocytes (immediate effect)
- Loss of the spleen's neutrophil clearance function (sustained effect)
- Reactive bone marrow response
Visual Trend Summary
PLATELETS WBC
↑ ↑
│ Peak (weeks) │ Rise within 1 day
│ /‾‾‾‾‾‾\ │ _______________
│ / \___ normalize │/ \__ normalize (months)
│ / rises Day 2 │
────┼──────────────────────► ───┼───────────────────────►
Pre-op Days Weeks Months Pre-op Days Weeks Months
(low in hypersplenism) (low in hypersplenism)
Why Both Rise - Mechanism
- Before splenectomy: The enlarged spleen sequesters up to 80% of the platelet pool and traps WBCs in congested sinusoids, causing both thrombocytopenia and leukopenia.
- After splenectomy: Both sequestration and immune-mediated destruction are abolished. The hyperplastic bone marrow (which was already working overtime) now has an unobstructed output - hence the overshoot into thrombocytosis and leukocytosis before normalizing.
Sources: Schwartz's Principles of Surgery 11E; Fischer's Mastery of Surgery 8E; Harrison's Principles of Internal Medicine 22E
Why does WBC not normalize faster like platelets?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
The key textbook passage (Schwartz's) confirms the critical facts. Here is the full mechanistic explanation:
Why WBC Stays Elevated Longer Than Platelets After Splenectomy
The answer is rooted in three fundamental differences between neutrophils and platelets.
1. The Spleen's Role is Different for Each Cell Type
This is the most important reason, directly from Schwartz's Surgery:
"The spleen's role in the normal clearance of neutrophils is not well established. Platelets...a third of the total platelet pool is sequestered in the spleen under normal circumstances."
- Schwartz's Principles of Surgery 11E
For platelets, the spleen is the dominant controller of circulating levels - it physically holds up to 80% of the pool in splenomegaly. Remove the spleen → that reservoir is immediately released → platelet count spikes fast and predictably.
For neutrophils, the spleen is NOT the primary clearance organ. The neutrophil leukocytosis after splenectomy is therefore not simply the reversal of sequestration - it reflects a broader, less tightly regulated phenomenon.
2. Neutrophil Half-Life is Extremely Short (~6 Hours)
| Cell | Normal lifespan in circulation |
|---|---|
| Neutrophil | ~6 hours |
| Platelet | ~10 days |
| RBC | ~120 days |
Because neutrophils turn over every few hours, the WBC count is continuously being reset by bone marrow output. After splenectomy:
- The hyperplastic bone marrow (which was overproducing WBCs to compensate for pre-op leukopenia) does not get an instant feedback signal to "stop overproducing."
- Regulation of granulopoiesis depends on cytokine signals (G-CSF, IL-17, etc.) that take days to weeks to re-equilibrate after the inflammatory/surgical stress and the change in demand.
- Because the neutrophil pool turns over multiple times per day, even a small excess in production maintains leukocytosis for a prolonged time.
Platelets, by contrast, survive 10 days - so as soon as the spleen is gone and marrow production re-regulates, the excess platelet production winds down within 1-2 weeks.
3. Surgical Stress Response Drives Prolonged Neutrophilia
Splenectomy itself is a surgical trauma. The acute phase response causes:
- Cortisol surge → demargination of neutrophils from vessel walls into circulating pool
- Epinephrine → further demargination
- IL-6, G-CSF → stimulate ongoing marrow neutrophil production
This stress-driven leukocytosis can persist for weeks to months independently of the splenectomy effect, and it is layered on top of the post-splenectomy change. Platelets are far less affected by the acute stress response.
4. The Marginating Pool Problem
In normal physiology, ~50% of circulating neutrophils are in the marginating pool (adherent to vessel walls, not counted in a standard WBC). The spleen acts as one margination site among many (liver sinusoids, lung capillaries, etc.).
After splenectomy, neutrophil margination redistributes across remaining sites. The recalibration of this marginating pool takes time, contributing to prolonged leukocytosis.
Summary: The Core Contrast
| Feature | Platelets | WBC (Neutrophils) |
|---|---|---|
| Spleen's role in clearance | Major - stores 1/3 to 80% of pool | Uncertain - not the primary organ |
| Mechanism of normalization | Release of sequestration reversed → fast | Cytokine re-regulation + stress resolution → slow |
| Cell lifespan | 10 days | 6 hours (needs constant marrow replenishment) |
| Effect of surgical stress | Minimal | Significant (demargination + G-CSF drive) |
| Timeline to normalize | Days to weeks | Weeks to months |
Bottom line: Platelets normalize relatively fast because the spleen was their main reservoir - remove the reservoir, count spikes, marrow adjusts within days-weeks. WBC stays elevated longer because neutrophil production is driven by bone marrow cytokine signals that take longer to reset, the spleen was never the primary WBC regulator, and surgical stress independently fuels granulopoiesis for months.
Sources: Schwartz's Principles of Surgery 11E; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.