Follicle vs papillae vs concretions in ophthalmology and it’s treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
follicle vs papillae vs concretions conjunctiva ophthalmology differences treatment
Reading File
Reading Web Page
https://entokey.com/follicular-conjunctivitis
Finding Sources
Reading File
Searching the Web
conjunctival concretions ophthalmology causes treatment removal calcified deposits eyelid
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Follicles vs Papillae vs Concretions in Ophthalmology
These are three distinct conjunctival findings that differ fundamentally in their structure, pathological basis, clinical location, associated diseases, and treatment. Correctly identifying them at the slit lamp is one of the most important skills in diagnosing conjunctival disease.
1. FOLLICLES
Structure & Pathology
Follicles are aggregations of lymphoid tissue (lymphocytes, lymphoblasts, and macrophages) within the conjunctival stroma. They are a non-vascular reaction - blood vessels run around the periphery, leaving the center avascular and pale/whitish. This is the key differentiating feature from papillae.
- They do NOT appear in neonates (lymphoid system is immature) and are less prominent under age 2
- Size: generally 0.5 mm to several mm; large ones are called "giant follicles"
- They are dome-shaped, smooth elevations
Clinical Appearance
- Grey-white or pale yellowish, dome-shaped elevations
- Blanched/pale apex with vessels at the base only
- Blood vessels course around the follicle, not through it
- Found most commonly in the inferior fornix and inferior palpebral conjunctiva
- In trachoma: superior tarsal plate (pathognomonic location)
Here is the classic appearance of trachomatous follicles on the superior tarsal conjunctiva (from Kanski's Clinical Ophthalmology):
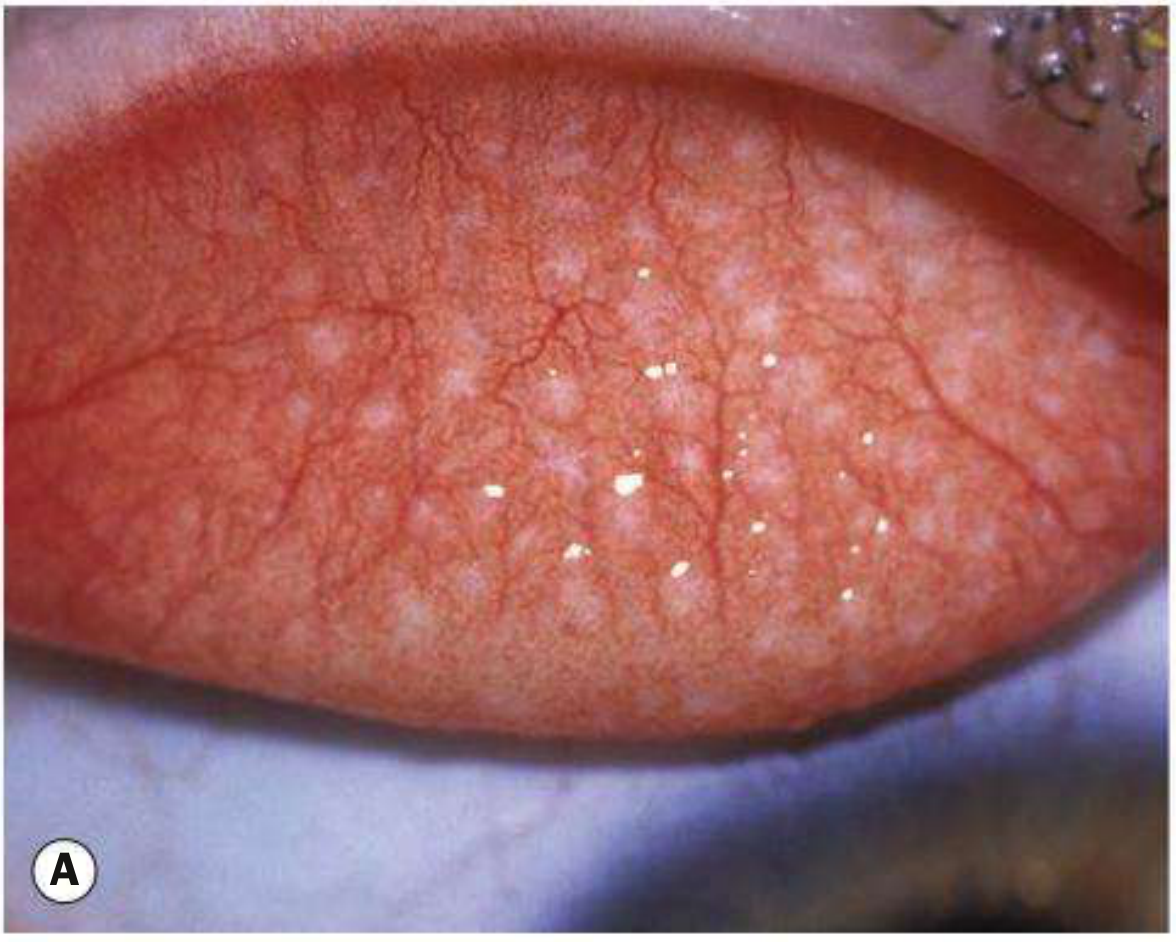
Fig. 6.7A - Typical white subtarsal follicles in trachoma. (Kanski's Clinical Ophthalmology, 10th ed.)
Associated Conditions
| Condition | Notes |
|---|---|
| Viral conjunctivitis (adenovirus, EKC) | Most common cause; inferior fornix follicles + watery discharge |
| Chlamydial conjunctivitis (adult inclusion) | Large forniceal + superior tarsal follicles; may persist months |
| Trachoma (C. trachomatis serovars A-C) | Superior tarsal follicles ≥5 in number, ≥0.5 mm (WHO grade TF) |
| Herpes simplex conjunctivitis | Unilateral follicles + vesicular lid lesions |
| Molluscum contagiosum | Chronic follicular reaction from shed viral antigen |
| Parinaud's oculoglandular syndrome | Unilateral follicles + preauricular lymphadenopathy |
| Topical drug-induced (miotics, antivirals, neomycin) | Inferior fornix follicles; resolves on drug withdrawal |
| Toxic/chemical conjunctivitis | |
| Physiologic (children 2-10 years) | Normal finding; asymptomatic, no treatment needed |
Treatment
Treatment targets the underlying cause, not the follicles themselves:
- Viral conjunctivitis: supportive (cold compresses, lubricants, antihistamine drops); topical steroids for subepithelial infiltrates
- Chlamydial (adult inclusion): Azithromycin 1g single oral dose OR doxycycline 100 mg BD x 7 days; test/treat sexual partners
- Trachoma (SAFE strategy):
- S - Surgery (trichiasis correction - lid rotation procedures)
- A - Antibiotics (azithromycin 1g single dose OR tetracycline eye ointment BD x 6 weeks)
- F - Face washing / cleanliness
- E - Environmental hygiene
- Topical drug toxicity: withdraw offending agent
- HSV: topical acyclovir ointment 5x/day OR oral acyclovir 400 mg 5x/day
2. PAPILLAE
Structure & Pathology
Papillae are fundamentally vascular reactions. They form because fibrous septa from the tarsus anchor the conjunctiva, dividing the epithelium into compartments. Within each compartment, a central blood vessel proliferates and becomes the core of the papilla, surrounded by oedema, neutrophils, eosinophils, mast cells, and other inflammatory cells.
- The fibrous septa limit their growth - except on the upper tarsus where septa are less dense, allowing giant papillae to form (GPC)
- They are smaller and flatter than follicles
Clinical Appearance
- Red or pink, flat-topped nodules with a central blood vessel (red core on slit lamp)
- Vessels radiate outward from center ("spoke-wheel" pattern)
- Pale/white at the base, red on the surface (opposite of follicles)
- Located primarily on superior palpebral (tarsal) conjunctiva
- Large papillae coalesce into a cobblestone appearance (GPC, VKC)
Key Memory Trick
| Feature | Follicle | Papilla |
|---|---|---|
| Center color | Pale/white (avascular) | Red (vascular core) |
| Shape | Dome-shaped, rounded | Flat-topped, polygonal |
| Location | Inferior fornix primarily | Superior tarsus primarily |
| Vessel pattern | Around the periphery | Central core with branches |
| Cause | Lymphoid (immune) reaction | Vascular/epithelial reaction |
| Lymphadenopathy | May be present | Absent |
Associated Conditions
| Condition | Papilla Features |
|---|---|
| Allergic conjunctivitis (SAC/PAC) | Small papillae, upper tarsus, itching, watery ropey discharge |
| Vernal keratoconjunctivitis (VKC) | Giant cobblestone papillae (upper tarsus) + limbal follicles (Trantas' dots) |
| Atopic keratoconjunctivitis (AKC) | Upper and lower lid papillae + eczematoid lid skin |
| Giant papillary conjunctivitis (GPC) | Large papillae on upper tarsus from contact lens, ocular prosthesis, exposed suture |
| Bacterial conjunctivitis | Small papillae + mucopurulent discharge |
| Floppy eyelid syndrome | Upper lid papillae from mechanical irritation |
| Chronic blepharitis | Fine papillae |
Treatment
Again, directed at the underlying cause:
- Allergic (SAC/PAC): antihistamine drops (olopatadine, azelastine), mast cell stabilisers (nedocromil, lodoxamide), cold compresses; avoid allergen
- VKC: mast cell stabilisers (sodium cromoglicate); topical steroids for acute exacerbations; cyclosporin 0.05-2% drops for steroid-sparing; supratarsal steroid injection for severe cases; giant papillae can be mechanically debrided
- AKC: as for VKC + treat eyelid eczema; tacrolimus 0.03-0.1% ointment to lids
- GPC: discontinue/change contact lens type/regime; switch to daily disposables; topical mast cell stabilisers/antihistamines; treat underlying foreign body or suture
- Bacterial: topical antibiotics (chloramphenicol, fusidic acid, fluoroquinolones)
- Floppy eyelid: lubricants; lid taping at night; surgical lid tightening if severe
3. CONCRETIONS (Conjunctival Lithiasis)
Structure & Pathology
Conjunctival concretions (also called lithiasis or calcareous deposits) are entirely different from follicles and papillae - they are not an active inflammatory response but rather a degenerative deposit.
They form from:
- Degenerated epithelial cells
- Compacted secretions from conjunctival glands (particularly Henle's glands in the fornix)
- Calcium salts, protein, mucin, and debris that become trapped in sub-epithelial depressions and calcify over time
They are avascular, non-inflammatory structures and represent epithelial degeneration, not an immune response.
Clinical Appearance
- Small (usually <1mm), yellow-white or chalky white deposits
- Hard consistency (calcified)
- Located in inferior palpebral conjunctiva and fornices (most common), occasionally superior
- May be single or multiple
- Usually subepithelial and asymptomatic
- When they erode through the epithelium, they cause a foreign body sensation and can abrade the cornea
- Usually discovered incidentally on routine slit lamp examination with eyelid eversion
Associated Conditions / Risk Factors
- Age (most common in elderly) - degenerative
- Chronic conjunctival inflammation (trachoma, follicular conjunctivitis)
- Dry eye disease
- Previous ocular surgery
- May be idiopathic
Comparison Table: Concretions vs Follicles vs Papillae
| Feature | Follicle | Papilla | Concretion |
|---|---|---|---|
| Nature | Lymphoid aggregate | Vascular-epithelial reaction | Calcified deposit |
| Vascularity | Avascular centre | Central blood vessel | Avascular (no vessels) |
| Color | Grey-white, translucent | Red/pink | Chalky yellow-white |
| Consistency | Soft | Soft | Hard/gritty |
| Location | Inferior fornix, superior tarsus (trachoma) | Superior tarsus | Inferior palpebral + fornix |
| Cause | Immune/infective | Allergic/mechanical/bacterial | Degenerative/age |
| Symptoms | Usually mild | Itching, mucous discharge | Usually asymptomatic until erosion |
| Resolves spontaneously | Yes (with treatment of cause) | Yes (with treatment) | No |
| Treatment | Treat underlying infection | Treat underlying allergy/cause | Observe if asymptomatic; remove if symptomatic |
Treatment of Concretions
- Asymptomatic concretions: observation only - no intervention required; most remain stable
- Symptomatic (foreign body sensation, corneal abrasion risk):
- Instil topical anaesthetic (proparacaine hydrochloride 0.5%) eyedrops
- Evert the eyelid
- Apply additional anaesthetic on a cotton-tipped swab directly over the concretion
- Use a 26G or 30G needle (bevel away from the eyelid) to lift and extract the deposit - or fine-tipped forceps
- Apply antibiotic drop/ointment post-procedure
- If the corneal epithelium was abraded, continue antibiotic drops for several days
- There is no medical therapy to dissolve or prevent concretions
- Recurrence is possible since the underlying degenerative process persists
Quick Clinical Summary
Red eye with follicles + watery discharge + preauricular node → VIRAL (treat supportively)
Red eye with follicles + mucopurulent discharge (weeks) + STI risk → CHLAMYDIAL (systemic antibiotics)
Superior tarsal follicles ≥ 5, size ≥ 0.5mm, endemic area → TRACHOMA (SAFE)
Itching + ropey discharge + cobblestone papillae → VKC/AKC (antihistamine, mast cell stabiliser)
Large upper tarsal papillae + contact lens use → GPC (stop lenses, stabilisers)
Hard yellow-white spots inferior palpebral, incidental, elderly → CONCRETIONS (observe or needle removal)
Sources: Kanski's Clinical Ophthalmology 10th Ed., Entokey - Follicular Conjunctivitis, StatPearls - Conjunctival Concretions, Eyes on Eyecare - Conjunctivitis Differential, Review of Optometry - Calcifications
This is a shared conversation. Sign in to Orris to start your own chat.