
430152f9-3e64-453f-a67e-a7c94ef73ff0.jpg
Hypotension and AF Patient on norad and amiadarone both infusion urine 100 ml overnight
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Critical ECG Analysis - Mrs. Manorama, 76F
This ECG requires immediate, urgent attention. The clinical picture and tracing strongly point to severe hyperkalemia as the unifying diagnosis, not primary AF or VT.
ECG Findings
| Parameter | Value | Significance |
|---|---|---|
| HR | 145 bpm | Tachycardia |
| QRS duration | 142 ms | Markedly wide |
| P axis | -150° | P waves abnormal / absent |
| QT/QTc | 320/468 ms | Prolonged |
| Morphology | Near-sine-wave pattern in precordial leads | Severe hyperkalemia pattern |
What is Actually Happening Here
This is NOT atrial fibrillation with a rapid ventricular response. The ECG shows a sine-wave / wide-complex tachycardia pattern - the most dangerous stage of hyperkalemia progression. The "AF" interpretation on the machine is almost certainly incorrect given the clinical context.
The triad screams hyperkalemia:
- Patient is on noradrenaline (vasopressor) = severely ill, likely in cardiogenic or distributive shock
- Urine output only 100 mL overnight = oliguric acute kidney injury / renal failure - potassium is not being excreted
- ECG shows massively wide QRS with near-sine-wave morphology in precordial leads
The progression of hyperkalemic ECG changes is:
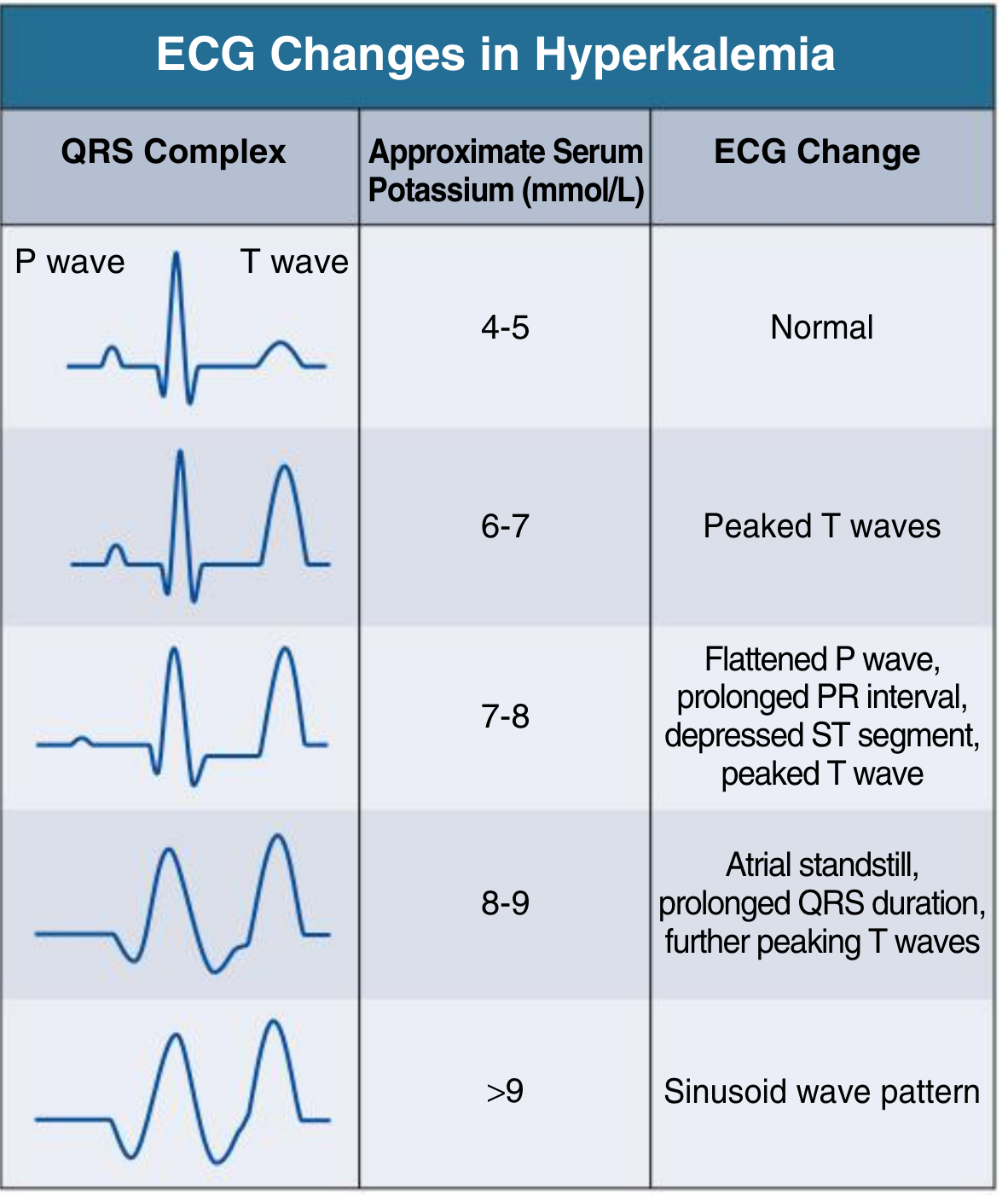
Potassium >9 mmol/L produces the sinusoidal pattern seen here. This patient is at immediate risk of ventricular fibrillation or asystole.
Emergency Management - Right Now
Step 1: Cardiac Membrane Stabilization (IMMEDIATE - within minutes)
Calcium gluconate 10% - 30 mL (3 g) IV slowly over 2-3 minutes (can repeat in 5 min if no ECG improvement)
- OR Calcium chloride 10%: 10 mL (1 g) via central line only
- This does NOT lower potassium - it buys time by stabilizing the myocardium
- Effect onset: 1-3 minutes; duration: 30-60 minutes
Step 2: Shift Potassium Intracellularly (Onset 15-30 min)
- Insulin + Dextrose: Actrapid 10 units IV + 25g dextrose (50 mL 50% dextrose) IV - lowers K by ~1 mEq/L
- Sodium bicarbonate: 50-100 mEq IV if acidotic (pH <7.3) - redistributes K intracellularly
- Salbutamol (nebulized): 10-20 mg via nebulizer - additional intracellular shift
Step 3: Remove Potassium from Body
- Furosemide: Patient is oliguric - use cautiously; may try 40-80 mg IV to encourage diuresis, but likely will not work with severe AKI
- Sodium polystyrene sulfonate (Kayexalate): 15-30 g orally or rectally - onset 1-2 hours
- Dialysis/CRRT - this patient almost certainly needs emergent hemodialysis or CRRT given oliguria + severe hemodynamic compromise. This is the definitive treatment.
What NOT to Do
- Do NOT attempt DC cardioversion for this rhythm - you are not treating AF
- Do NOT give more amiodarone - it will not help and prolongs QT further in an already compromised conduction system
- Do NOT stop noradrenaline abruptly - maintain hemodynamic support
Immediate Investigations Needed
| Test | Why |
|---|---|
| Serum potassium STAT | Confirm hyperkalemia - expect >7-9 mEq/L |
| ABG with electrolytes | Assess pH, ionized Ca2+, K+, lactate |
| Serum creatinine/urea | Confirm AKI severity |
| Serum calcium, magnesium | Electrolyte profile |
| Repeat ECG after calcium | To document response |
Summary
This 76-year-old woman on vasopressors with overnight oliguria (100 mL) has a life-threatening hyperkalemia producing a sine-wave/wide-complex tachycardia on ECG. The automated diagnosis of "AF" is misleading.
Immediate priority: Calcium gluconate IV now, followed by insulin-dextrose, then arrange urgent nephrology review and CRRT/dialysis. Get a STAT potassium level but do not wait for the result before giving calcium.
- Comprehensive Clinical Nephrology 7th Ed - ECG changes table: sine wave pattern correlates with K+ >9 mmol/L
- Tintinalli's Emergency Medicine - hyperkalemia treatment protocol with calcium, insulin, bicarbonate
- Goldman-Cecil Medicine - hyperkalemia causing sinoventricular rhythm preceding VF
Potassium is 3.89
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Revised Assessment - K+ is 3.89 mEq/L (Normal)
Hyperkalemia is off the table. This significantly changes the differential. Let me reassess the ECG and clinical picture systematically.
Re-reading the ECG
The machine called the rhythm "AF" but the automated measurements also show:
- HR 145 bpm
- QRS 142 ms (markedly wide)
- P axis -150° (abnormal)
- QTc 468 ms (prolonged)
- The precordial leads show a near-sinusoidal wide-complex pattern
The automated label of "AF" in the context of a wide QRS at 145 bpm should be treated as AF with a wide QRS - meaning one of the following:
Differential Diagnosis - Wide Complex Tachycardia at 145 bpm
| Diagnosis | Likelihood | Key Clue |
|---|---|---|
| Ventricular Tachycardia (VT) | HIGHEST | Hemodynamically unstable, on vasopressor, QRS 142 ms |
| AF with pre-existing bundle branch block | Moderate | Machine called "AF"; irregular rhythm possible |
| AF with aberrant conduction (rate-related BBB) | Moderate | Rate 145 could cause functional BBB |
| AF via accessory pathway (pre-excited AF) | Lower | Would expect even wider, bizarre QRS, irregular |
| Amiodarone-induced QRS widening | Consider | IV amiodarone blocks Na+ channels, widens QRS |
Clinical rule: In any hemodynamically unstable patient on vasopressors with a wide-complex tachycardia - treat as VT until proven otherwise. - Tintinalli's Emergency Medicine
The Amiodarone Factor - Important
IV amiodarone is a class I + III antiarrhythmic - it blocks sodium channels (widens QRS) AND potassium channels (prolongs QT). In a patient already on an amiodarone infusion:
- The wide QRS (142 ms) may be partly or wholly drug-induced conduction slowing
- The QTc of 468 ms is concerning - amiodarone + hypotension + electrolyte shifts create a risk of Torsades de Pointes
- If this IS VT and the patient is already on amiodarone, adding more amiodarone is unlikely to help and may worsen conduction
Critical Questions to Answer NOW
1. Is this rhythm regular or irregular?
- Regular = favour VT or SVT with BBB
- Irregular = favour AF with aberrancy
- The machine said "AF" but the tracing appears fairly regular in the limb leads - please look at the rhythm strip carefully
2. Are there any visible P waves?
- Dissociated P waves = VT (AV dissociation)
- No P waves + irregular = AF with aberrancy
3. What was the baseline ECG before the tachycardia?
- A pre-existing BBB on a prior ECG would support AF with aberrancy rather than VT
Immediate Management Plan
If hemodynamically unstable (which she is - on noradrenaline):
Step 1 - Do NOT wait for diagnosis certainty:
Treat as VT - perform synchronised DC cardioversion immediately
- Start at 200J biphasic (or 150J if that is the device setting)
- Sedate if conscious (midazolam 1-2 mg IV + fentanyl 25-50 mcg IV titrated)
- Keep crash trolley at bedside
If a brief pause before cardioversion is acceptable:
Step 2 - Check if rhythm is truly irregular (looks at V1 for fibrillatory baseline)
- If truly irregular wide-complex tachycardia: AF with aberrancy - amiodarone may help, but she is already on it
- If regular: monomorphic VT - cardiovert
Step 3 - After cardioversion / rhythm control:
- Check 12-lead in sinus rhythm - look for baseline BBB, delta waves (WPW), or ischemic changes
- Troponin - tachycardia at 145 in a sick elderly woman - rule out ACS driving the rhythm
- Echo - LV function? The tachycardia + hypotension may be from underlying structural heart disease
- Electrolytes panel: Mg2+ (hypomagnesaemia worsens AF and predisposes to TdP), Ca2+, Na+
Step 4 - Review the amiodarone:
- If QTc remains >500 ms after rhythm control, consider reducing or stopping the amiodarone infusion
- Switch to digoxin for AF rate control in haemodynamically compromised patients - it has less negative inotropy and does not widen QRS
- Or beta-blocker at ultra-low dose if EF is preserved
Summary of the Situation
This 76F is in haemodynamic shock (on noradrenaline) with a wide-complex tachycardia at 145 bpm and oliguria (100 mL overnight = AKI likely from poor perfusion). The tachycardia is either driving the shock (tachycardia-mediated cardiomyopathy / reduced diastolic filling) or is a consequence of it. Either way, restoring a controlled rhythm is the priority. Potassium being normal is reassuring - but check magnesium urgently, as hypomagnesaemia is an independent cause of refractory AF and predisposes to TdP with amiodarone.
Immediate action: Synchronised cardioversion if unstable. Get Mg2+ level. Reassess rhythm for regularity. - Tintinalli's Emergency Medicine; Braunwald's Heart Disease
Patient has CAD and ischemic stroke too Had hyponatremia now corrected
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Updated Clinical Picture - Full Problem List
Mrs. Manorama, 76F:
- Known CAD (coronary artery disease)
- Known ischemic stroke (prior)
- Hyponatremia - now corrected
- Currently: Hypotension on noradrenaline + amiodarone infusion
- Wide-complex tachycardia at 145 bpm (machine says AF, QRS 142 ms)
- Oliguria - 100 mL overnight
How CAD + Stroke Changes Everything
1. The Wide Complex Tachycardia is Almost Certainly VT
CAD is the #1 cause of VT. Myocardial infarction creates scar tissue that acts as a substrate for re-entrant ventricular tachycardia. In a patient with known CAD presenting with:
- Wide QRS (142 ms) at 145 bpm
- Haemodynamic instability requiring vasopressors
- Oliguria (end-organ hypoperfusion)
This is scar-mediated monomorphic VT until proven otherwise. The machine calling it "AF" should be set aside - automated ECG algorithms have poor sensitivity for VT.
2. The Tachycardia May Be Ischaemia-Driven
A 76-year-old with known CAD who suddenly develops a wide-complex tachycardia with haemodynamic collapse - STEMI or NSTEMI must be excluded right now.
- Acute ischaemia can trigger VT even without a new infarct
- The VT itself causes demand ischaemia, creating a vicious cycle
3. Stroke History - Major Implications for Management
| Decision | Impact of Prior Stroke |
|---|---|
| DC Cardioversion | SAFE to do for unstable VT/AF - stroke history is not a contraindication to electrical cardioversion |
| Anticoagulation for AF | Her CHA₂DS₂-VASc score is extremely high (age 76 + female + stroke = at least 4-5 points) - she needs anticoagulation but timing is critical given recent ischaemic stroke |
| Thrombolysis | Absolutely contraindicated if stroke was recent (<3 months) |
| Anticoagulation NOW | If AF is the confirmed rhythm, full anticoagulation is indicated - but if the stroke was very recent (<2-4 weeks), discuss with neurology before starting |
4. Hyponatremia - Now Corrected, But Watch For ODS
If hyponatremia was corrected rapidly (>8-10 mEq/L in 24h), the patient is at risk for osmotic demyelination syndrome (central pontine myelinolysis). In a patient with prior ischaemic stroke, this brain is already vulnerable. Clinical signs: dysarthria, dysphagia, altered consciousness, quadriparesis - watch for these. The haemodynamic deterioration could in part reflect a neurological complication.
Revised Priority Management
IMMEDIATE - Right Now
1. Synchronised DC Cardioversion
- Patient is haemodynamically unstable (vasopressor-dependent) with wide-complex tachycardia
- Prior stroke is NOT a contraindication to cardioversion
- 200J biphasic, synchronised
- Sedate with IV midazolam 1-2 mg + fentanyl 25 mcg (titrate carefully - she is already hypotensive)
- Goal: restore sinus rhythm, improve cardiac output, reduce vasopressor requirement
2. Troponin + 12-lead post-cardioversion immediately
- Rule out ACS/STEMI as the trigger for VT
- A post-conversion 12-lead will reveal baseline BBB, old infarct pattern, or ischaemic changes
3. STAT Magnesium
- Hypomagnesaemia is common after diuresis, poor intake, and illness
- Low Mg²⁺ causes refractory AF and increases TdP risk with amiodarone
- Replace IV if <0.8 mmol/L: MgSO₄ 2g IV over 10-20 min
AFTER CARDIOVERSION
| Action | Rationale |
|---|---|
| Bedside echo (POCUS) | LV function? Wall motion abnormality = ischaemia/old infarct |
| Troponin serial (0h/3h/6h) | Exclude ACS driving the arrhythmia |
| Coronary angiogram if troponin rises | Revascularisation may be needed |
| Neurology review | Re-stroke risk assessment, safe anticoagulation window post-stroke |
| Anticoagulation planning | If confirmed AF: CHA₂DS₂-VASc ≥4 - DOAC or heparin, timing per neurology |
| Sodium recheck | Confirm correction rate was safe; watch for ODS signs |
| Renal review | Oliguria + AKI - may need CRRT if creatinine rising |
Amiodarone Infusion - Continue or Stop?
- If the rhythm is VT: amiodarone is appropriate (continue)
- If the rhythm is AF with BBB: amiodarone is appropriate (continue), but rate may be inadequate - she is already on it
- If QTc post-cardioversion is >500 ms: reduce dose and consider whether amiodarone is contributing to QRS widening
- Do NOT add any other QT-prolonging drugs
The Bigger Picture
This woman has multiple simultaneous crises converging:
CAD + ischaemia
↓
VT / AF → ↓ cardiac output
↓
Hypotension → ↑ noradrenaline (vasopressor)
↓
Renal hypoperfusion → oliguria → AKI
↓
± electrolyte disturbances → perpetuate arrhythmia
Cardioversion breaks this cycle. Everything else (anticoagulation, renal support, ischaemia work-up) follows from achieving rhythm control.
Bottom line: Cardiovert now. Get troponin + echo. Involve cardiology, nephrology, and neurology urgently. The stroke history adds complexity to anticoagulation decisions but does not delay electrical treatment of the arrhythmia.
This is a shared conversation. Sign in to Orris to start your own chat.