Explain hypersensitivity in simplest as non medico
Imagine your body has a security guard - your immune system. Its job is to protect you from dangerous invaders like bacteria and viruses.
Hypersensitivity is when that security guard becomes overly suspicious and aggressive - it starts attacking harmless things (like pollen, dust, certain foods, or even your own body) as if they were deadly enemies.
The 4 Types - In Simple Language
Think of 4 different "overreaction styles":
Type 1 - The Instant Panic Attack
"Oh no, BEES!" → Immediate alarm
- Happens within minutes
- The guard sees pollen/peanuts/bee sting → hits the emergency alarm instantly
- Body releases chemicals (histamine) → sneezing, itching, swelling, or in severe cases - full shutdown (anaphylaxis)
- Examples: Hay fever, peanut allergy, asthma, bee sting allergy
Type 2 - Friendly Fire
"Wait, I'm shooting my own team!"
- The guard mistakes your own body cells as the enemy and attacks them
- Happens with blood, organs, or tissues
- Examples: Blood transfusion reactions (wrong blood type), some drug allergies that destroy blood cells
Type 3 - Garbage Pile Buildup
"Too much trash left lying around"
- When the guard kills enemies, it normally cleans up the mess. Here, the cleanup fails - dead enemy clumps pile up in tissues
- Those clumps then trigger inflammation and damage
- Takes hours to days to show up
- Examples: Certain autoimmune diseases, farmer's lung (breathing in mold)
Type 4 - The Slow Burn
"I'll hold a grudge... for days"
- No alarm chemicals this time - instead, the guard sends in soldiers (T-cells) who are slow but persistent
- Takes 2-3 days to react
- Examples: Poison ivy rash, skin reactions to nickel jewelry, TB skin test reaction
Quick Summary Table
| Type | Nickname | Speed | Common Example |
|---|---|---|---|
| 1 | Instant Panic | Minutes | Peanut allergy, hay fever |
| 2 | Friendly Fire | Hours | Wrong blood transfusion |
| 3 | Garbage Pile | Hours-Days | Some autoimmune diseases |
| 4 | Slow Burn | 2-3 Days | Poison ivy, nickel rash |
The bottom line: Your immune system is supposed to protect you - but in hypersensitivity, it's doing too much of a good thing, causing damage to your own body in the process. It's not weak - it's actually overworking.
Explain as medico
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full medical-level explanation.
Hypersensitivity - Medical Overview (Gell & Coombs Classification)
Definition
Hypersensitivity is an exaggerated or augmented immune response that is harmful to the host. It requires a presensitised state - classically manifesting on second (or subsequent) antigen exposure. The term encompasses reactivity to:
- Exogenous environmental antigens (allergens)
- Antigens from another species (xenoantigens)
- Self antigens (autoimmunity)
The underlying effector mechanisms are identical to those used in normal host defense - the pathology arises because they are too intense, misdirected, or occur at inappropriate anatomical sites.
"Hypersensitivity responses lead to tissue damage: immunopathology." - Roitt's Essential Immunology
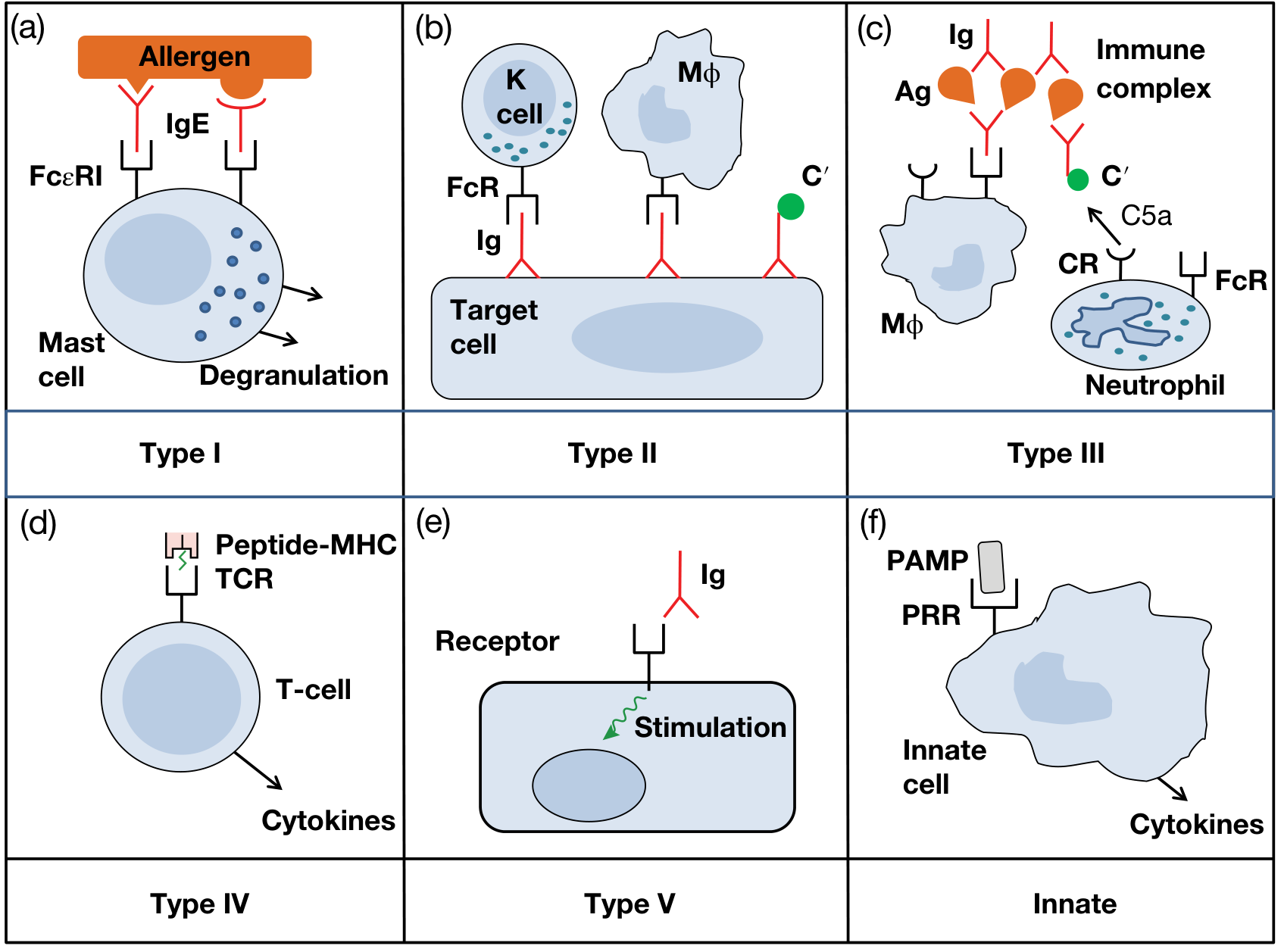
Classification: Gell & Coombs (1963) - Types I to IV
Types I, II, III = Antibody-mediated | Type IV = T cell-mediated
Type I - Immediate (IgE-mediated) Hypersensitivity
Mechanism
Sensitisation phase:
- Allergen processed by APCs → drives Th2 polarisation → IL-4/IL-13 → class switching in B cells to produce IgE
- IgE binds via its Fc portion to high-affinity FcεRI receptors on mast cells and basophils (also low-affinity FcεRII/CD23 on B cells, eosinophils)
- Host is now sensitised - no symptoms yet
Effector/Elicitation phase (seconds-minutes):
- Second antigen exposure → allergen cross-links cell-surface IgE molecules
- FcεRI aggregation in lipid rafts → ITAM activation → Lyn, Syk, Fyn tyrosine kinase cascade
- PLCγ activation → DAG + IP3 → PKC activation + Ca²⁺ release from ER
- Mast cell degranulation - release of preformed and newly synthesised mediators
Mediators
| Category | Mediators | Effect |
|---|---|---|
| Preformed (granules) | Histamine, tryptase, heparin, chymase | Vasodilation, ↑ vascular permeability, bronchospasm |
| Newly synthesised (lipid) | PGD2, LTC4, LTD4, LTE4, TXA2 | Bronchoconstriction, vasodilation, chemotaxis |
| Cytokines | IL-4, IL-5, IL-13, TNF-α, GM-CSF, CCL11 (eotaxin) | Late-phase inflammation, eosinophil recruitment |
| Late-phase | LTB4 | Leukocyte chemotaxis |
Biphasic response:
- Early phase (0-30 min): Mast cell degranulation, histamine dominant
- Late phase (4-12 hrs): Eosinophil/neutrophil influx driven by lipid mediators and cytokines
Clinical Manifestations
- Systemic anaphylaxis (parenteral allergen exposure)
- Atopy: Hayfever (allergic rhinitis), asthma, atopic eczema, urticaria, food allergy
- Atopy has strong familial/genetic predisposition; associated with elevated serum IgE
Treatment
- Epinephrine (reverses bronchoconstriction, anaphylaxis)
- Antihistamines (H1-receptor antagonists)
- Corticosteroids (suppress late-phase)
- Omalizumab - humanised anti-IgE monoclonal Ab (targets Cε3 domain, blocks FcεRI binding)
- Desensitisation immunotherapy (shifts Th2 → Th1; induces IgG "blocking" antibodies; Treg induction)
Type II - Antibody-Dependent Cytotoxic Hypersensitivity
Mechanism
-
IgG (or IgM) antibodies directed against antigens on cell surfaces or extracellular matrix
-
Tissue damage via three effector pathways:
- Complement activation (classical pathway) → MAC-mediated cell lysis, opsonisation with C3b/C4b for phagocytosis
- ADCC (Antibody-Dependent Cellular Cytotoxicity) - K cells/NK cells bearing FcγRIII (CD16) bind IgG-coated targets and lyse them
- Opsonisation - IgG/C3b → Fc/complement receptors on macrophages/neutrophils → enhanced phagocytosis
-
In some Type II variants, antibody binding to surface receptors stimulates or blocks function without cytolysis (sometimes called "Type V" or stimulatory hypersensitivity - e.g., Graves' disease: anti-TSH receptor Ab → thyroid stimulation)
Clinical Examples
| Condition | Antibody Target |
|---|---|
| ABO transfusion reaction | RBC alloantigens (A/B blood group) |
| Rh hemolytic disease of newborn | D antigen on fetal RBCs |
| Autoimmune hemolytic anaemia | RBC surface antigens |
| Goodpasture syndrome | Type IV collagen (GBM + alveolar BM) |
| Drug-induced cytopenias (penicillin) | Drug-hapten on RBC/platelet surface |
| Myasthenia gravis* | AChR at NMJ (blocking) |
| Graves' disease* | TSH receptor (stimulatory) |
Often classified under stimulatory/Type V
Type III - Immune Complex-Mediated Hypersensitivity
Mechanism
- Soluble antigens combine with circulating antibody (IgG/IgM) → form immune complexes (ICs)
- Normally ICs are cleared by the mononuclear phagocyte system; in Type III, this clearance fails
- IC deposition in vessel walls, glomeruli, synovium, or skin
- Deposited ICs activate:
- Classical complement pathway → C3a, C5a (anaphylatoxins) → mast cell degranulation, vascular permeability
- C5a → neutrophil and monocyte chemotaxis
- Neutrophils attempt phagocytosis of ICs → frustrated phagocytosis → lysosomal enzyme release → tissue damage
- Platelet aggregation → microthrombi, ischaemia
Onset: Hours to days (Arthus reaction: local; serum sickness: systemic)
Arthus reaction - local IC deposition after intradermal Ag in presensitised host; intense neutrophilic inflammation, haemorrhagic necrosis
Serum sickness - systemic IC disease; fever, urticaria, arthralgia, glomerulonephritis; classically seen 7-10 days after heterologous serum administration
Clinical Examples
- Serum sickness, drug reactions (e.g., sulfonamides)
- Post-streptococcal glomerulonephritis
- SLE (anti-dsDNA ICs in kidneys)
- Rheumatoid arthritis (RF-IgG complexes in joints)
- Hypersensitivity pneumonitis/Farmer's lung (inhaled fungal/organic antigens)
- Cryoglobulinaemia
Type IV - Delayed-Type Hypersensitivity (DTH) / Cell-Mediated
Mechanism
- The only T cell-mediated type; no antibody involved
- Two subtypes:
TD (Delayed - CD4⁺ Th1 mediated):
- Sensitisation: APCs present peptide-MHC II to naive CD4⁺ T cells → Th1 priming
- Re-exposure → antigen-specific Th1 cells activated → release IFN-γ, TNF-β, IL-2, GM-CSF
- IFN-γ activates macrophages → oxidative burst, lysosomal enzymes, pro-inflammatory cytokines → tissue destruction
- Chronic activation → granuloma formation (collections of activated macrophages, epithelioid cells, giant cells, surrounded by lymphocytes)
- Onset: 48-72 hours (hence "delayed")
TC (Contact - CD8⁺ CTL mediated):
- Hapten-modified keratinocytes present peptide-MHC I → CD8⁺ CTL priming
- Re-exposure → CD8⁺ CTL directly kills hapten-bearing cells via perforin/granzymes
- Classic example: allergic contact dermatitis (nickel, urushiol in poison ivy)
Subtypes of Type IV (extended classification)
| Subtype | Primary Cell | Timeframe | Example |
|---|---|---|---|
| IVa | Th1 (IFN-γ, macrophage activation) | 48-72h | Tuberculin PPD reaction |
| IVb | Th2 (IL-4/IL-5, eosinophilia) | 48-72h | Some forms of eczema |
| IVc | CD8⁺ CTL (perforin/granzymes) | 48-72h | Contact dermatitis, SJS |
| IVd | Neutrophilic (IL-8/GM-CSF) | 24-48h | AGEP (pustular drug reaction) |
Clinical Examples
- Tuberculin test (Mantoux): Induration at 48-72h = Type IV (classic teaching example)
- Allergic contact dermatitis (nickel, rubber, urushiol)
- Granulomatous diseases: TB, sarcoidosis, leprosy (tuberculoid), Crohn's disease
- Graft rejection (chronic)
- Type 1 diabetes mellitus (CD8⁺ CTL destruction of β cells)
Type V - Stimulatory Hypersensitivity (Roitt's Addition)
- Antibodies bind to cell surface receptors and mimic the natural ligand → receptor stimulation or inhibition without cytolysis
- Not always listed in standard 4-type classification, but mechanistically distinct from Type II
- Examples:
- Graves' disease: TSI (thyroid-stimulating immunoglobulin) activates TSHR → hyperthyroidism
- Myasthenia gravis: anti-AChR Ab blocks receptor → flaccid paralysis
Comparative Summary Table
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Mediator | IgE | IgG/IgM (cell-surface) | IgG/IgM (soluble Ag-Ab complexes) | T cells (Th1/CTL) |
| Antigen | Exogenous allergen | Cell surface / matrix | Soluble circulating Ag | Intracellular/contact |
| Effector mechanism | Mast cell degranulation | Complement, ADCC, opsonisation | IC deposition → complement, neutrophils | Cytokines, CTL, macrophage activation |
| Onset | Seconds-minutes | Minutes-hours | Hours-days | 48-72 hours |
| Complement involved? | No (sometimes via C3a/C5a) | Yes | Yes | No |
| Prototype disease | Anaphylaxis, asthma | ABO transfusion reaction | Serum sickness, SLE | Tuberculin test, contact dermatitis |
| Key cells | Mast cells, basophils, eosinophils | NK cells, phagocytes | Neutrophils, macrophages | CD4⁺ Th1, CD8⁺ CTL, macrophages |
Clinical Pearl - Multiple Types in One Disease
Many diseases involve overlapping types:
- Asthma: Type I (IgE/mast cell) + Type IVb (Th2 eosinophilic)
- SLE: Type II (anti-RBC, anti-platelet) + Type III (anti-dsDNA IC in kidneys) + Type IV (T cell-mediated tissue damage)
- Atopic dermatitis: Type I + Type IVb
"In a particular disease state more than one type of hypersensitivity may be operating." - Roitt's Essential Immunology, 13th Ed.
Sources: Roitt's Essential Immunology 13e | Jawetz, Melnick & Adelberg's Medical Microbiology 28e | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.