Ectopic beats
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ectopic beats" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have all the information needed. Let me compile a comprehensive answer.
Ectopic Beats
Ectopic beats are cardiac impulses that originate from a focus other than the sinoatrial (SA) node. They are among the most common arrhythmias encountered in clinical practice and are classified by their site of origin: atrial, junctional (AV nodal), or ventricular.
1. Overview and Mechanisms
Ectopic beats arise from three broad electrophysiologic mechanisms:
- Enhanced automaticity - abnormal spontaneous depolarization in non-SA tissue
- Re-entry - a self-perpetuating loop of electrical activity through tissue with differing refractory periods
- Triggered activity - afterdepolarizations (early or delayed) that reach threshold, commonly seen with digitalis toxicity or electrolyte disturbances
Tintinalli's Emergency Medicine, p. 145: "Ectopic beats originate from atrial, AV nodal, and/or ventricular tissues. These beats are frequently benign but can cause symptoms, with patients noting palpitations or an irregular heartbeat."
2. Premature Atrial Contractions (PACs)
Epidemiology
PACs are very common in the general population. In adults over 50, the average is approximately 1-2 per hour, increasing with each decade. Associated with cardiovascular disease, stress, alcohol, and caffeine. Regular physical exercise is protective.
Symptoms
Usually asymptomatic. When symptomatic, patients describe a "skipped beat," fluttering sensation in the chest or throat, heightened heartbeat awareness, or momentary dizziness.
ECG Features
| Feature | Description |
|---|---|
| P wave timing | Premature - appears earlier than expected |
| P wave morphology | Different from sinus P wave (different shape/axis) |
| PR interval | May be prolonged (relative refractory period) or normal |
| QRS complex | Usually narrow (normal); may be aberrant |
| Pause | Non-compensatory (PAC resets the SA node) |
| Non-conducted PAC | Most common cause of unexpected pause on ECG |
12-lead ECG showing frequent atrial ectopics (Braunwald's Heart Disease):
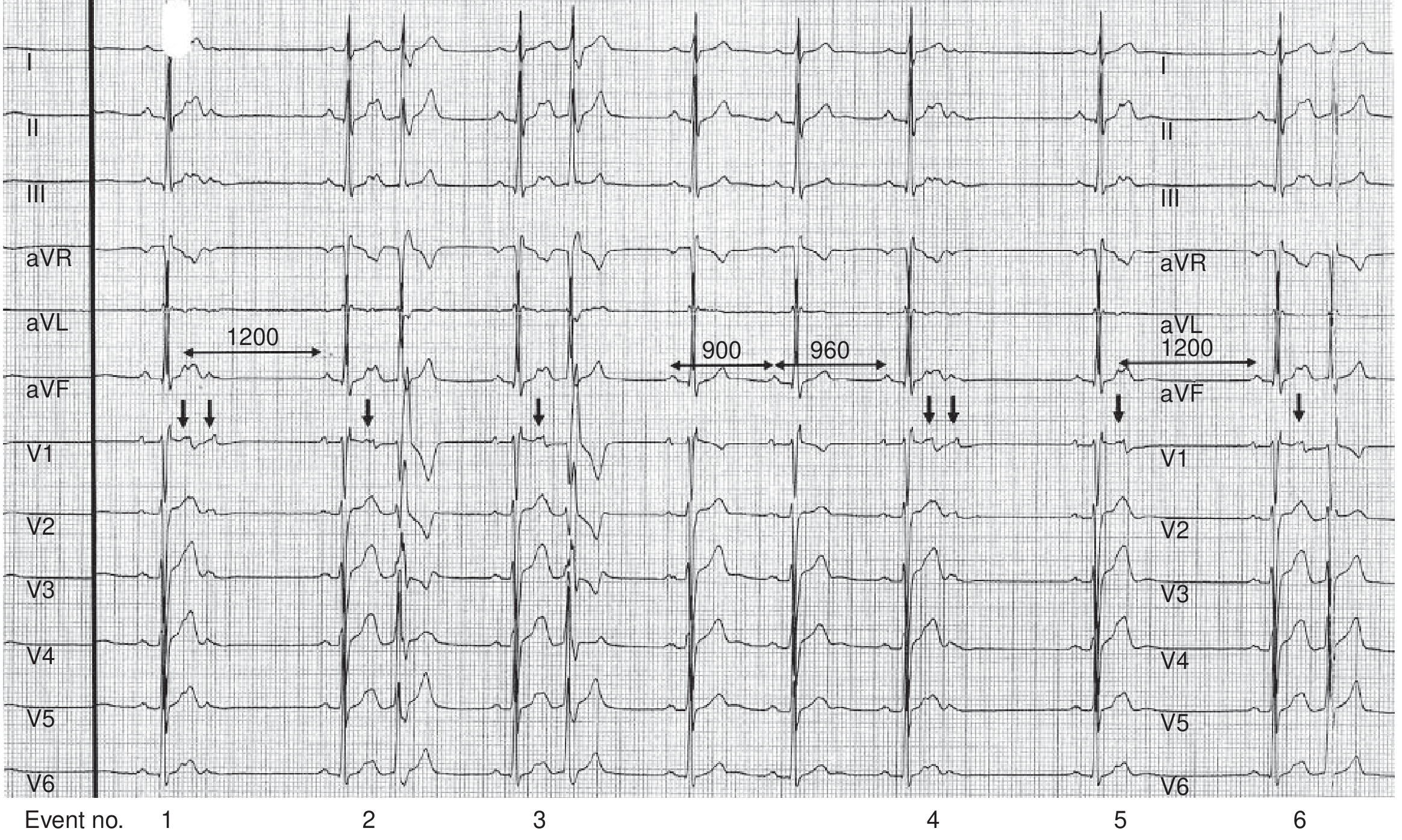
Events 1 & 4: Two atrial ectopics (the second of each pair non-conducted, creating a pause). Events 2 & 3: Conducted atrial ectopics. Note the intervals: 1200ms normal P-P, 900ms/960ms coupling intervals.
Atrial trigeminy pattern (Tintinalli's):

Patterns
- Atrial bigeminy - PAC every other beat
- Atrial trigeminy - PAC every third beat
- Non-conducted PAC in bigeminy - mimics marked sinus bradycardia
Clinical Significance and Risks
Although usually benign, frequent PACs carry important associations:
- Excess PACs (>30/hour or runs of non-sustained AT >20 beats) are associated with incident atrial fibrillation (AF), stroke, and death on 15-year follow-up
- In patients with CHADS-VASc ≥ 2, annual stroke risk is comparable to AF patients
- Frequent PACs (20-40% daily burden) may cause a reversible cardiomyopathy
- PACs originating from pulmonary vein sleeves are a key trigger of AF (Haissaguerre et al.)
Treatment of PACs
- The vast majority need only reassurance
- No evidence that treating isolated PACs reduces stroke risk or improves outcomes
- Treatment is indicated only when sufficiently symptomatic
- Step-up approach:
- Beta-blocker or calcium channel antagonist (first-line)
- Antiarrhythmic (e.g., flecainide) for refractory symptoms
- Catheter ablation for highly symptomatic patients with high ectopic burden and unifocal origin
3. Premature Ventricular Contractions (PVCs)
Description
PVCs occur when electrical impulses originate from single or multiple ventricular foci, bypassing the normal His-Purkinje system, and are identified by wide, bizarre QRS complexes.
ECG Features
| Feature | Description |
|---|---|
| P wave | Absent before QRS; occasional retrograde P wave follows QRS |
| QRS | Wide (>120 ms), bizarre morphology, different from sinus QRS |
| ST/T wave | Opposite direction to major QRS deflection (discordant) |
| Pause | Fully compensatory postectopic pause (SA node not reset) |
| Coupling interval | Fixed within ~40 ms of the preceding beat (in bigeminy/trigeminy) |
Classification by Morphology
- Isolated - occasional single PVC
- Unifocal - multiple PVCs of identical morphology (single ventricular focus)
- Multifocal - PVCs with different morphologies (>1 ventricular focus; implies more instability)
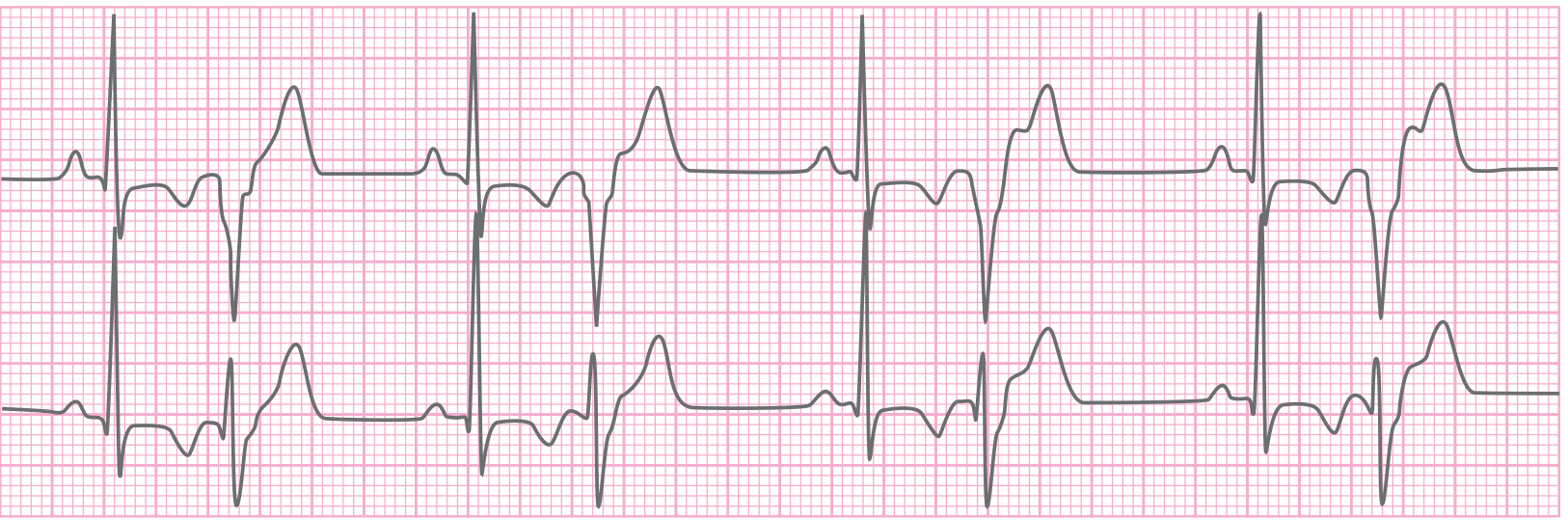
Ventricular bigeminy (Tintinalli's):
Dangerous Patterns
- R-on-T phenomenon - PVC falls on the vulnerable period of the T wave, risk of inducing ventricular fibrillation (VF)
- Non-sustained VT - 3 or more consecutive PVCs
- Couplets - 2 consecutive PVCs
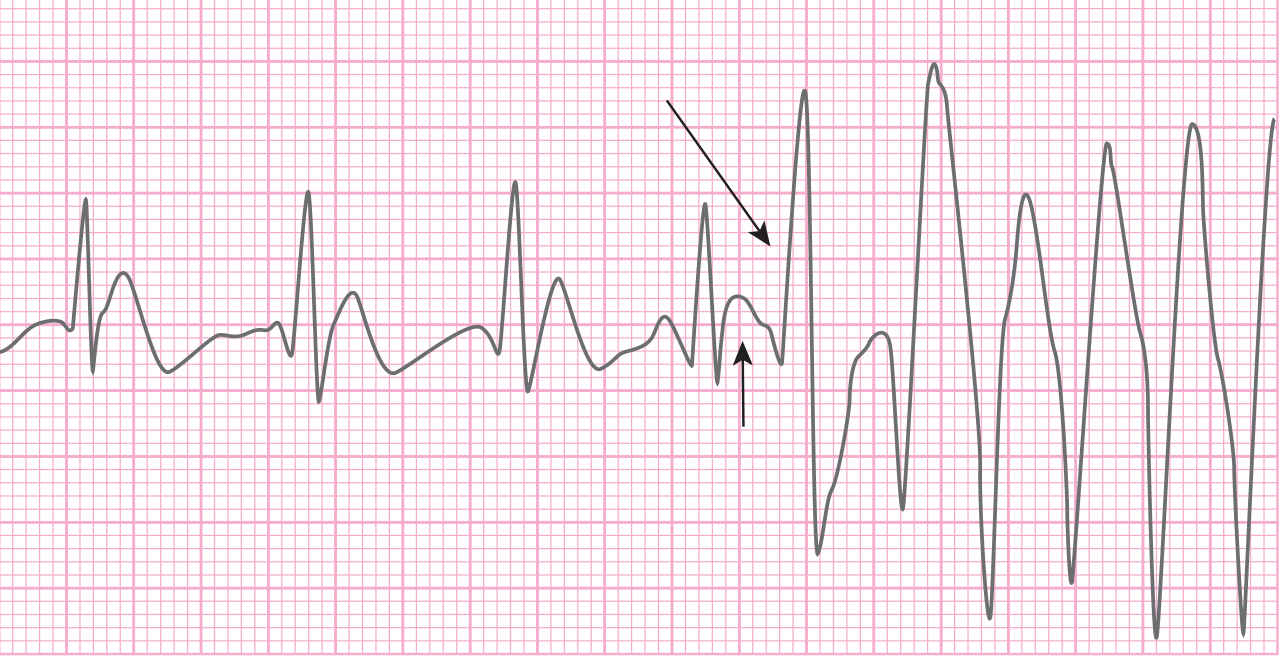
R-on-T initiating ventricular tachycardia in a STEMI patient:
PVC with underlying junctional escape below:

Clinical Significance
- Very common; infrequent PVCs can occur in structurally normal hearts
- Triggers: hypoxia, electrolyte disturbances, ischemia, sympathomimetics (cocaine, amphetamines, caffeine, nicotine), digoxin toxicity
- Correlation with severity of underlying coronary artery disease
- Independent risk factor for sudden cardiac death
- In acute coronary syndrome, PVCs indicate electrical instability, but "warning arrhythmia" patterns are not reliable predictors of subsequent VF
- PVC-induced cardiomyopathy: frequent PVCs persisting >30 months, typically >15-20% PVC burden, presenting with palpitations and heart failure symptoms - reversible with ablation
Treatment of PVCs
- Review ECG for ischemia/infarction, chamber enlargement, QT prolongation, Brugada pattern
- Treat reversible causes: hypoxia, electrolytes, drug effects
- Lifestyle modification: reduce stimulants (caffeine, nicotine) - not consistently effective
- Pharmacologic suppression of isolated PVCs with IV antiarrhythmics in acute settings does not improve survival; long-term oral antiarrhythmics increase mortality due to pro-arrhythmic properties (CAST trial principle)
- ICD: for patients with PVCs at risk of triggering malignant ventricular arrhythmias
- Catheter ablation: for PVC-induced cardiomyopathy - reduces PVC burden and allows recovery of ventricular function
4. Junctional (AV Nodal) Ectopics
Arise from the AV node or His bundle when SA node activity is suppressed or fails to reach the AV node. The junction has an intrinsic rate of 40-60 bpm.
| Rhythm | Rate | ECG |
|---|---|---|
| Junctional escape beat/rhythm | 40-60 bpm | Narrow QRS, no P wave (or inverted retrograde P near QRS) |
| Accelerated junctional rhythm | 60-100 bpm | Same morphology, faster rate |
| Junctional tachycardia | >100 bpm | Same morphology, rapid rate |
5. Differentiating Ectopic Beats from Aberrant Conduction
A wide-complex beat can be either a PVC (ventricular origin) or a supraventricular beat conducted aberrantly (e.g., with bundle branch block). Key distinguishing features favoring ventricular origin:
- AV dissociation (P waves independent of QRS) - strongly suggests VT/PVC
- Capture beats - occasional narrow QRS during wide-complex rhythm
- Fusion beats - QRS morphology between normal and ectopic
- QRS duration - very wide (>160 ms) favors ventricular origin
- Concordance - all QRS in precordial leads positive or negative favors VT
6. Summary Table
| Feature | PAC | PVC | Junctional |
|---|---|---|---|
| P wave | Early, abnormal morphology | Absent (or retrograde) | Absent or retrograde (inverted, near QRS) |
| QRS width | Narrow (usually) | Wide, bizarre | Narrow |
| Pause type | Non-compensatory | Fully compensatory | None (escape) |
| Common triggers | Caffeine, alcohol, anxiety, AF | Ischemia, electrolytes, stimulants | SA node dysfunction, digoxin |
| Serious risk | AF, stroke (if frequent) | VT, VF (R-on-T, multifocal) | Low (usually protective escape) |
Sources: Braunwald's Heart Disease (12th ed.), p. 1246; Tintinalli's Emergency Medicine, pp. 145-147
Are they harmful
Finding Sources
Finding Sources
Searching PubMed
"premature ventricular contractions" AND prognosis
Reading File
Reading File
Reading File
I have comprehensive data. Here is a clear, structured answer:
Are Ectopic Beats Harmful?
The honest answer is: usually not, but context is everything. The same type of beat carries very different implications depending on whether the heart is structurally normal or diseased.
The Reassuring Side - Most Are Benign
Harrison's Principles of Internal Medicine (2025) states directly: "In most cases, ventricular ectopy is asymptomatic and does not require specific treatment. While most commonly benign when presenting in patients with structurally normal hearts and normal ECGs..."
For PACs specifically (Braunwald's): despite associations with AF and stroke risk, "there is no evidence that treatment of isolated atrial ectopy reduces risk or improves long-term outcomes."
For healthy adults with occasional PVCs and no structural heart disease, the 4-5 year prognosis is excellent, with <1% per year risk of a cardiac event - Pfenninger & Fowler's Procedures for Primary Care.
When They Can Be Harmful
Ectopic beats become clinically concerning across several scenarios:
1. Underlying Structural Heart Disease
This is the most important risk factor. PVCs in the setting of:
- Myocardial ischemia or post-MI - PVCs are a harbinger of sustained VT or ventricular fibrillation (VF). Asymptomatic ventricular ectopic beats are a known marker for increased risk of sudden death from VF in patients convalescing from MI (Goodman & Gilman's)
- Existing cardiomyopathy - PVC frequency and complexity (couplets, NSVT) correlate with disease severity
- ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy) - Right ventricular origin PVCs with RV enlargement/dysfunction require MRI to exclude this condition
- Cardiac sarcoidosis - similar concern
2. PVC-Induced Cardiomyopathy (a silent danger)
Frequent, sustained PVCs can damage the heart over time, even in people who otherwise had a normal heart:
- Threshold: typically >15-20% PVC burden (i.e., >15-20% of all heartbeats are PVCs)
- Timeline: usually requires >30 months of persistent high burden
- Evidence (Fuster & Hurst's The Heart): a dose-response relationship has been demonstrated -
- >20,000 PVCs/24 hours - subclinical decline in ejection fraction
- >10,000 PVCs/24 hours - LV dilation
- Upper quartile PVC burden in the Cardiovascular Health Study (1,139 patients, >13-year follow-up): 3× greater odds of LVEF decline, 48% increased risk of heart failure, 31% increased risk of death
- The good news: this is reversible - successful catheter ablation normalizes LV parameters, with LVEF improvement in 47-100% of cases
3. Triggering Dangerous Arrhythmias
- R-on-T PVC - falls on the vulnerable phase of the T wave, can trigger VF
- PVC initiating VT - particularly in ischemic hearts
- PACs triggering AF, atrial flutter, or atrial tachycardia - especially in susceptible atria
4. Frequent PACs and Stroke Risk
- Excess PACs (>30/hour or runs of non-sustained AT >20 beats) are associated with incident AF, stroke, and death at 15-year follow-up (Braunwald's)
- In patients with CHADS-VASc ≥ 2, annual stroke risk becomes comparable to known AF patients
5. QRS Morphology Clues to Danger
Harrison's (2025) notes that ECG morphology itself gives prognostic information:
- Smooth, sharp QRS deflections = likely normal myocardial substrate (more benign)
- Broad, notched, slurred QRS = suggests diseased myocardial substrate (more concerning)
- RBBB-pattern PVCs are more likely to be associated with structural heart disease than LBBB-pattern PVCs
- Multifocal PVCs (multiple morphologies) suggest a myopathic process
Simple Risk Stratification Summary
| Scenario | Verdict | Action |
|---|---|---|
| Occasional PVCs/PACs, normal heart, normal ECG | Benign | Reassurance only |
| Symptomatic but structurally normal heart | Low risk | Treat symptoms (beta-blocker) |
| High PVC burden (>15-20%), prolonged duration | Risk of cardiomyopathy | Monitor; ablation if burden persists |
| PVCs post-MI or with cardiomyopathy | Potentially dangerous | Investigate; ICD if indicated |
| Multifocal PVCs with RV origin | Exclude ARVC/sarcoidosis | Cardiac MRI required |
| Frequent PACs with CHADS-VASc ≥ 2 | Stroke risk equivalent to AF | Anticoagulation consideration |
| R-on-T phenomenon | Can trigger VF | Urgent evaluation |
Bottom line: In a healthy person with a structurally normal heart, ectopic beats are mostly a nuisance. They become genuinely harmful when they occur in diseased hearts, when their burden is very high over a long time (risking cardiomyopathy), or when they trigger sustained arrhythmias. The single most important question clinicians ask is: "Is there structural heart disease?"
- Harrison's Principles of Internal Medicine 22E (2025), p. 1402
- Braunwald's Heart Disease, p. 1246
- Fuster & Hurst's The Heart 15th Ed., p. 1321
Railway spine
Finding Sources
Searching the Web
railway spine 19th century history medical condition Herbert Page John Erichsen
Reading File
Reading File
Reading File
Reading Web Page
https://hekint.org/2026/02/05/the-rise-and-fall-of-railway-s…
Excellent - I now have comprehensive material from forensic medicine textbooks, psychiatry texts, and historical sources. Here is a full answer:
Railway Spine
Definition
Railway spine was a 19th-century medical-legal diagnosis applied to a cluster of neurological and psychological symptoms occurring in survivors of railway accidents - particularly those who showed no obvious external injury. The term was coined and popularized by London surgeon John Eric Erichsen following his 1866 publication On Railway and Other Injuries of the Nervous System, and the condition is sometimes called Erichsen's Disease.
Historical Background
Why railways?
Early 19th-century railway travel was uniquely dangerous. Railway cars were flimsy wooden structures with no occupant protection, and collisions were frequent. The sheer violence of a train crash - sudden deceleration forces far exceeding anything previously known in peacetime - was unlike any prior mechanism of injury.
The medico-legal problem
Soon after major accidents, passengers began coming forward with symptoms but no visible wounds. Railways dismissed these claims as fraud, calling them "litigation neurosis" - arguing that the only real injury was the desire to sue. This created a forensic vacuum: courts needed medical expert opinion on whether suffering without visible injury was genuine.
Erichsen's formulation (1866)
Rather than dismissing these patients, Erichsen argued brilliantly that railway spine was simply a modern form of an ancient condition: "concussion of the spine." He traced the diagnosis back to 1766 (the Count de Lordat, who walked away from a carriage accident then developed progressive neurological symptoms over four years until his death). By anchoring railway spine in pre-industrial precedent, Erichsen legitimized the diagnosis and removed its association with compensation-seeking.
His proposed pathophysiology was organic: the violent forces of a collision caused microscopic "molecular derangements" in the spinal cord - too subtle to see at autopsy but sufficient to produce progressive inflammatory changes he called chronic meningitis or subacute myelitis. Since no technology existed to examine a living patient's spinal cord, his theory was essentially unfalsifiable at the time.
Clinical Features
Modern forensic medicine texts describe railway spine as concussion of the spinal cord - a transient disturbance caused by violent acceleration/deceleration or rotational forces without necessarily any visible cord damage.
Mechanism (Essentials of Forensic Medicine & Toxicology, 2026): momentary collision of the cord against the wall of the canal or transient deformity of the spinal canal profile due to violent acceleration/deceleration.
Characteristic symptom pattern (from both Erichsen's original descriptions and Herbert Page's 1883 revision):
| Category | Symptoms |
|---|---|
| Neurological | Headache, giddiness, weakness in limbs, transient paralysis (arms, hands, bladder, rectum, lower extremities), amnesia, loss of memory/concentration |
| Autonomic | Restlessness, sleeplessness, excessive sweating, polyuria, diarrhea, feeble/slow pulse, palpitations |
| Psychological | Neurasthenia, nervousness, increased startle response, tremor on excitement, melancholy, hopelessness, avoidance of noise, desire to be alone |
| Other | Loss of sexual power, derangement of special senses, ocular fatigue |
Key clinical point: Symptoms may not appear immediately - they can come on hours after the incident. Temporary paralysis typically recovers within ~48 hours unless the cord is lacerated.
The Great Controversy: Organic vs. Functional
The nature of railway spine became one of the most hotly contested medical debates of the late 19th century, argued at the Imperial Society of Physicians in Vienna in 1886.
Erichsen's organic theory
The violent impact caused invisible spinal cord damage - real structural pathology that explained all symptoms.
Herbert William Page's functional theory (1885)
Page, surgeon to the London and North-West Railway, challenged Erichsen directly. He proposed railway spine was a functional disorder - not structural damage, but a disturbance in how the nervous system operated. His key argument: fear alone could produce every symptom Erichsen attributed to cord lesions.
His famous case: a railway employee found in "a state of collapse" after apparently having his foot run over. Examination revealed "the only damage was the dexterous removal of the heel of his boot by the wheel of a passing engine." The man's terror, not injury, had produced his symptoms.
Page's symptom list from his 1883 book, presented in order of frequency, closely resembles the current DSM criteria for PTSD: sleeplessness, circulatory disturbances, headache, nervousness with increased startle response, tremor, melancholy, hopelessness, avoidance of noise, social withdrawal, memory impairment.
Jean-Martin Charcot's position
The great French neurologist sided with Page: some railway spine symptoms were caused by hysteria - a psychological mechanism, not spinal pathology.
Hermann Oppenheim's position
Germany's leading neurologist maintained that all railway spine symptoms were due to physical damage to the spine or brain. He coined the term "traumatic neurosis" in 1881 to encompass the psychiatric and neurologic symptoms arising from shock - but still attributed them to organic causes.
Resolution
Autopsy studies in two railway spine cases published in 1895 (Dercum) found no spinal pathology. Erichsen himself eventually conceded, acknowledging that "spinal concussion" had been "replaced by the term traumatic neurasthenia" and that his original term was "chosen for want of any good alternatives and an imperfect understanding of nervous system pathology."
Forensic and Legal Significance
Railway spine created an entirely new branch of forensic medicine. It established the legal and medical principle that injury without visible external damage is real and compensable. Courts regularly awarded substantial damages to plaintiffs, often presuming spinal cord injury. Medical practitioners were called as expert witnesses by both sides - creating the modern template of forensic medical testimony.
The legal battles forced medicine to grapple with a fundamental question that remains unresolved even today: how do you prove or disprove subjective suffering?
Legacy and Modern Equivalents
Railway spine is the historical ancestor of three modern diagnostic categories:
| Modern Condition | Connection to Railway Spine |
|---|---|
| Whiplash (WAD) | Direct mechanical successor - cervical hyperflexion-extension from sudden deceleration; Parikh's forensic text explicitly equates cervical momentary dislocation at C4-C6 as the mechanism |
| PTSD | Psychological successor - Carol Moeli (1881) elaborated the psychiatric consequences of railway accidents into the first description of what became PTSD; "shell shock" (1915), "combat fatigue" (WWII), and finally PTSD (DSM-III, 1980) are all lineal descendants |
| Traumatic neurosis / functional neurological disorder | Oppenheim's 1881 term coined directly from railway spine cases |
Kaplan & Sadock's Comprehensive Textbook of Psychiatry states explicitly: "In 1866, London surgeon John Eric Erichsen originated the diagnosis of 'railway spine'... Carol Moeli, a Berlin psychiatrist, elaborated in 1881 upon the specific psychiatric consequences of such events, penning the first description of what became known as post-traumatic stress disorder (PTSD)."
Summary
Railway spine matters for three reasons:
- Clinically - it established that violent deceleration forces can injure the nervous system without visible external trauma (now understood as concussive/whiplash mechanisms)
- Psychiatrically - it was the first systematic recognition that psychological trauma causes real, disabling symptoms, laying the groundwork for the entire concept of PTSD
- Medicolegally - it created the framework for compensation of invisible injury, a principle still litigated in courts worldwide
Sources: Essentials of Forensic Medicine & Toxicology (36th ed., 2026), p. 265; Parikh's Medical Jurisprudence & Forensic Medicine; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Hektoen International - Rise and Fall of Railway Spine (2026)
This is a shared conversation. Sign in to Orris to start your own chat.