Twin pregnancy
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
twin pregnancy complications TTTS preterm
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive review of the major complications of twin pregnancy, drawn primarily from Creasy & Resnik's Maternal-Fetal Medicine.
Complications of Twin Pregnancy
Twin pregnancies carry substantially higher morbidity and mortality than singletons. The most clinically significant complications are grouped below by whether they are exclusive to monochorionic (MC) twins or shared by all twin types.
Complications Specific to Monochorionic Twins
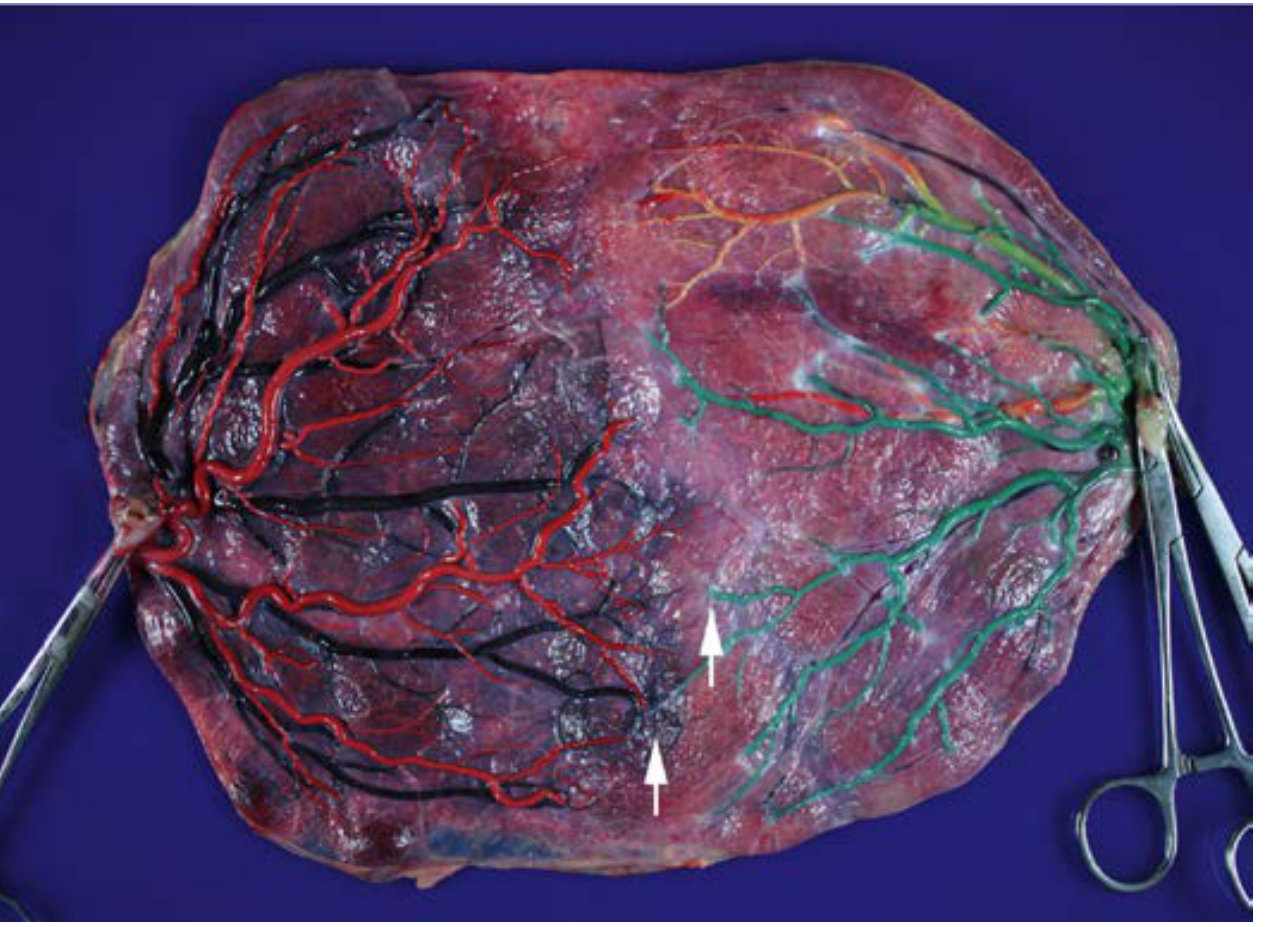
These arise because MC twins share a single placenta connected by vascular anastomoses (artery-to-artery [AA], vein-to-vein [VV], and artery-to-vein [AV]).
1. Twin-to-Twin Transfusion Syndrome (TTTS)
Incidence: ~10-15% of monochorionic-diamniotic (MCDA) twin pregnancies.
Pathophysiology:
TTTS is a chronic condition caused by unbalanced fetofetal blood transfusion from the donor twin to the recipient twin through placental vascular communications. The primary driver is net flow imbalance through unidirectional AV anastomoses. When not compensated by bidirectional AA anastomoses, the donor becomes hypovolemic and anemic while the recipient develops polycythemia and hypervolemia.
- The renin-angiotensin system is upregulated in the donor and downregulated in the recipient
- Atrial natriuretic peptide, BNP, and endothelin-1 are elevated in the amniotic fluid of the recipient twin
- Uneven placental sharing (>25% territory difference) is present in ~50% of TTTS vs. ~25% of non-TTTS MC pregnancies
- Peripheral (marginal or velamentous) cord insertion, almost always of the donor twin, is seen in ~50% of TTTS cases
The classic clinical sign is the twin oligohydramnios-polyhydramnios sequence (TOPS): oligohydramnios in the donor and polyhydramnios in the recipient.
Staging (Quintero system):
| Stage | Finding |
|---|---|
| I | Polyhydramnios (MVP ≥8 cm) + oligohydramnios (MVP ≤2 cm) |
| II | Donor fetal bladder not visible |
| III | Critically abnormal Doppler studies (absent/reversed end-diastolic UA flow, reversed DV a-wave, reversed UA flow) |
| IV | Hydrops fetalis |
| V | Demise of one or both fetuses |
Management:
- Fetoscopic laser photocoagulation (FLP) of placental anastomoses is the treatment of choice for stage II-IV TTTS before 26 weeks
- A 2024 systematic review (PMID 38400574) examined how cannula diameter in laser surgery affects outcomes
- A 2025 systematic review (PMID 40470767) specifically examined interventions to prevent preterm birth after laser surgery for TTTS
Forms of TTTS:
- Chronic TTTS - the classic form described above
- Acute perimortem TTTS - exsanguination of the surviving twin into the dead co-twin's low-pressure circulation; mediated by large AA or VV anastomoses
- Acute peripartum TTTS - blood shifts during delivery due to uterine contractions, delayed cord clamping, or fetal position changes; ranges from subclinical hemoglobin discordance to frank hypovolemic shock in the donor
2. Twin Anemia-Polycythemia Sequence (TAPS)
Incidence: ~3-6% of MC twins spontaneously; higher rates after laser treatment for TTTS (post-laser TAPS).
Pathophysiology:
TAPS is caused by only a few, very small placental anastomoses. These allow a chronic, slow transfusion of blood - too gradual to cause oligohydramnios/polyhydramnios, but producing large intertwin hemoglobin discordance. The donor becomes severely anemic; the recipient becomes polycythemic.
Key distinction from TTTS: No significant amniotic fluid discordance - the absence of TOPS is what separates TAPS from TTTS.
Diagnosis:
- MCA peak systolic velocity (MCA-PSV) >1.5 multiples of the median (MoM) in the anemic donor
- MCA-PSV <1.0 MoM in the polycythemic recipient
- Confirmed postnatally by large intertwin hemoglobin difference (>8 g/dL)
3. Twin-Reversed Arterial Perfusion (TRAP) Sequence
An extreme complication unique to MC twins where one twin (the "pump twin") perfuses an acardiac, severely malformed co-twin in a retrograde fashion via large AA anastomoses. The pump twin is at risk of high-output cardiac failure and hydrops.
Acardiac phenotypes:
- Acardius acephalus (60-75%): developed pelvis/lower limbs, no cranial or thoracic structures
- Acardius anceps (15%): well-developed body but only partial cranial development
- Acardius amorphus (rare): amorphous tissue mass
- Acardius acormus (very rare): cephalic structures only
Management options include radiofrequency ablation or laser to interrupt the vascular communication to the acardiac twin.
4. Selective Fetal Growth Restriction (sFGR)
Incidence: 10-25% of MC twin gestations.
Pathophysiology: Uneven placental sharing (one twin has a significantly smaller cotyledon territory) combined with abnormal placental angiogenesis leads to growth restriction of the smaller twin while the co-twin grows normally.
Diagnosis: No universally agreed criteria; most use:
- Estimated fetal weight <10th percentile for GA in one twin
- Abdominal circumference <5th-10th percentile
- Significant fetal weight discordance
Classification (Gratacós system based on UA Doppler):
| Type | UA Doppler of smaller twin | Risk |
|---|---|---|
| I | Positive end-diastolic flow | Good prognosis |
| II | Persistently absent/reversed end-diastolic flow | High risk of fetal deterioration and death |
| III | Intermittent absent/reversed end-diastolic flow | Unpredictable; risk of sudden fetal demise and neurological damage |
Type III sFGR carries particular concern because intermittent flow reversal is associated with increased neurological damage in the growth-restricted twin.
5. Single Intrauterine Fetal Death (sIUFD) in MC Twins
When one MC twin dies in utero, the surviving twin is at significant risk of death (~15-20%) or neurological damage (~25-30%) due to acute hemodynamic shifts through the shared placental circulation. A 2026 systematic review (PMID 40934452) updated estimates of perinatal outcomes after sIUFD in MC pregnancies.
Complications Common to All Twin Pregnancies
Preterm Birth
The single most common complication of twins overall:
- ~50% of twins deliver before 37 weeks
- ~10-15% deliver before 32 weeks (extreme prematurity)
- The greatly enlarged uterine volume causes premature activation of labor pathways
Predictors:
- Short cervical length on midtrimester ultrasound
- Positive fetal fibronectin
- Prior preterm birth
Interventions - disappointing results overall:
- Cervical cerclage (prophylactic): Systematic reviews and meta-analyses have not shown benefit for unselected twin pregnancies or those with short cervix; however, in women with asymptomatic cervical dilation 1-5 cm before 24 weeks, an RCT by Berghella et al. showed cerclage + indomethacin + antibiotics reduced preterm birth at all cutoffs and cut early preterm birth (<28 weeks) by 50%, with a 78% reduction in perinatal mortality
- Cervical pessary: A large multicenter RCT (N=1180) showed no significant reduction in spontaneous birth before 34 weeks (13.6% vs. 12.9%)
- Vaginal progesterone: Individual patient meta-analysis by Romero et al. showed benefit for women with twin gestation AND sonographic short cervix - reduces preterm birth before 30-35 weeks and neonatal mortality, without neurodevelopmental harm; NOT recommended for unselected twins
- 17-OHPC (intramuscular progesterone): No benefit in twins
- Prophylactic tocolytics: No proven benefit
Practical takeaway: In unselected twins, no intervention reliably prevents preterm birth. In twins with a sonographically short cervix, vaginal progesterone shows the strongest evidence. Cerclage is reserved for those with physical exam-indicated dilation.
Fetal Growth Restriction (in Dichorionic Twins)
- Occurs when one dichorionic twin has placental insufficiency; no shared vascular communication, so risk to co-twin is minimal
- Managed with surveillance and timing of delivery
- Discordance >20-25% in estimated fetal weight signals increased perinatal risk
Other Major Complications (All Twins)
| Complication | Notes |
|---|---|
| Gestational hypertension / preeclampsia | 2-3x higher risk than singleton |
| Gestational diabetes | Increased risk |
| Placental abruption | Especially after delivery of first twin |
| Fetal malpresentation | ~75% have non-cephalic presentation of at least one twin |
| Velamentous cord insertion | Higher in twins, especially MC |
| Increased perinatal mortality | 5-6x higher than singletons overall |
Summary Table: MC-Specific vs. All-Twin Complications
| Complication | Monochorionic Only | All Twins |
|---|---|---|
| TTTS | Yes | No |
| TAPS | Yes | No |
| TRAP sequence | Yes | No |
| sFGR (with Type II/III Doppler) | Yes | No |
| sIUFD with co-twin risk | Yes (high) | No (low in DC) |
| Preterm birth | - | Yes |
| Preeclampsia | - | Yes |
| FGR (general) | - | Yes |
| Malpresentation | - | Yes |
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (9780323828499), Chapters 5, 8, 17, 37
- PMID 38400574 - Cannula diameter and outcomes after laser surgery for TTTS (Sys Rev, 2024)
- PMID 40470767 - Interventions to prevent preterm birth after fetoscopic laser for TTTS (Sys Rev, 2025)
- PMID 40934452 - Perinatal outcome after sIUFD in MC twin pregnancy (Sys Rev, 2026)
This is a shared conversation. Sign in to Orris to start your own chat.