Galezzi fracture etiology mechanism of injury associated injury signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Searching the Web
Galeazzi fracture anatomy mechanism treatment diagram X-ray
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the material I need to write a comprehensive, well-illustrated answer. Let me compile the full response.
Galeazzi Fracture: A Complete Clinical Review
1. Definition and Historical Context
A Galeazzi fracture (also called Galeazzi fracture-dislocation) is a fracture of the middle to distal third of the radial shaft combined with dislocation or subluxation of the distal radioulnar joint (DRUJ). It was first described by Ricardo Galeazzi, an Italian surgeon, in 1934.
Other names used in the literature:
- "Fracture of necessity" (Campbell) - reflecting the absolute need for surgery in adults
- "Piedmont fracture" - named after the location where it was widely studied
- "Reverse Monteggia fracture" - because Monteggia involves ulna + radial head, while Galeazzi involves radius + DRUJ
Galeazzi fractures account for ~7% of all forearm fractures in adults. Isolated radial shaft fractures without DRUJ involvement are actually rare - the combination should be assumed until proven otherwise.
- Rosen's Emergency Medicine, 10th Ed.
- Tintinalli's Emergency Medicine
- Campbell's Operative Orthopaedics, 15th Ed. 2026
2. Relevant Anatomy
The forearm is a complex mechanical unit. The radius and ulna articulate at both ends:
- Proximal radioulnar joint (PRUJ) - at the elbow (radial head)
- Distal radioulnar joint (DRUJ) - at the wrist (ulnar head articulates with sigmoid notch of radius)
The DRUJ is stabilized by:
- Triangular fibrocartilage complex (TFCC) - the primary DRUJ stabilizer
- Dorsal and volar radioulnar ligaments
- Pronator quadratus (PQ) - muscle stabilizer
- Interosseous membrane (IOM)
- Extensor carpi ulnaris (ECU) subsheath
The deforming muscles act after a Galeazzi fracture to maintain displacement:
- Pronator quadratus - pronates the distal fragment
- Brachioradialis - shortens and angulates the radius
- Abductor pollicis longus (APL) and Extensor pollicis brevis (EPB) - displace the distal fragment
This anatomy diagram from Campbell's Operative Orthopaedics shows the surgical approach (volar Henry approach) with key structures:
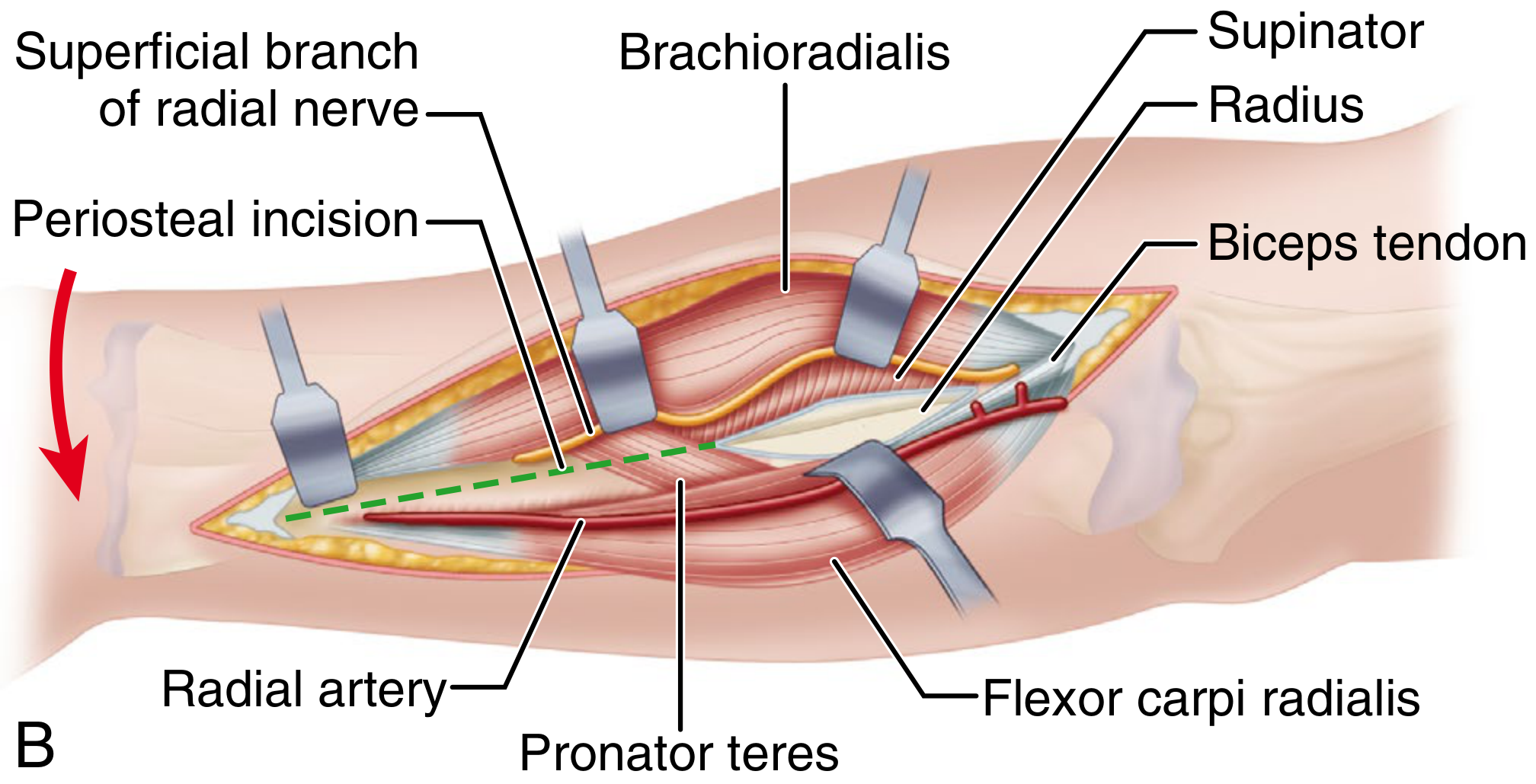
Anatomical relationships during the volar (Henry) approach to the radial shaft - Campbell's Operative Orthopaedics 15th Ed.
3. Etiology and Mechanism of Injury
Primary Mechanisms
There are two recognized mechanisms:
Mechanism 1 - Fall on an outstretched hand (FOOSH) in hyperpronation (most common):
- Patient extends their arm to brace for impact
- The forearm is in forced hyperpronation at the moment of contact
- The axial load combined with hyperpronation creates a bending force on the distal radius
- The DRUJ is simultaneously disrupted by the rotational and shear forces
Mechanism 2 - Direct blow:
- A direct impact to the dorsolateral aspect of the forearm
- Less common but well recognized
- Typically seen in motor vehicle collisions, high-energy sports, or occupational injuries
Why the DRUJ Dislocates
When the radius fractures, the distal fragment is pulled out of alignment by the deforming muscles (PQ, brachioradialis, APL, EPB). As the radius shortens, the TFCC and radioulnar ligaments are stretched and torn, allowing the ulna to dislocate - most commonly dorsally relative to the radius.
The distance from the fracture to the wrist joint matters:
-
Fracture less than 7.5 cm from the articular surface: DRUJ is unstable in 55% of cases
-
Fracture more than 7.5 cm from the articular surface: DRUJ is unstable in only 6% of cases
-
Miller's Review of Orthopaedics, 9th Ed.
4. Classification
OTA/AO Classification (most used):
| Code | Description |
|---|---|
| 22-A2.3 | Simple radius fracture + DRUJ dislocation |
| 22-A3.3 | Simple fracture of both radius (distal zone) + DRUJ dislocation |
| 22-B2.3 | Wedge fracture of radius + DRUJ dislocation |
| 22-B3.3 | Wedge fracture of both bones + DRUJ dislocation |
Classification by Direction of Radial Displacement (Campbell's):
The fracture can be classified based on direction of radial fragment displacement:
- Type I (Dorsal) - Dorsal angulation of the distal fragment (most common). Ulna dislocates dorsally.
- Type II (Volar) - Volar angulation of the distal fragment. Ulna dislocates volarly.
This distinction matters for post-operative immobilization position.
5. Associated Injuries
A Galeazzi fracture is rarely an isolated bony injury. Associated injuries include:
| Structure | Injury |
|---|---|
| TFCC | Tear (primary DRUJ stabilizer - most common soft tissue injury) |
| Ulnar styloid | Fracture at the base (indicates DRUJ avulsion) |
| Interosseous membrane | Tear (can contribute to proximal migration of radius - Essex-Lopresti variant) |
| Anterior interosseous nerve (AIN) | Stretch injury - loss of thumb/index DIP flexion |
| Radial nerve (superficial branch) | Stretch or contusion |
| Extensor/flexor tendons | Rare entrapment in DRUJ blocking reduction |
| Radial artery | Rare vascular injury in high-energy mechanisms |
| Elbow | Must examine - rule out associated proximal injury (Essex-Lopresti) |
Key point: Always examine the entire forearm and elbow, not just the wrist. The Essex-Lopresti lesion (radial head fracture + IOM disruption + DRUJ injury = longitudinal radioulnar dissociation) must be excluded.
6. Signs and Symptoms
History
- Mechanism of injury (fall, direct blow, MVC)
- Dominant vs. non-dominant hand
- Occupation and activity level (relevant for surgical planning)
Physical Examination Findings
Local findings:
- Swelling and tenderness over the distal radial shaft - the fracture site
- Visible deformity - angulation or shortening of the forearm
- Prominent ulnar head at the wrist - due to DRUJ dislocation (the ulna becomes visually and palpably prominent)
- Tenderness at the DRUJ - can be subtle when other pain is dominant
Functional findings:
- Pain with forearm rotation (pronation and supination)
- Reduced grip strength
- In cases with nerve involvement: weakness of thumb IP flexion (AIN injury)
DRUJ instability testing:
- Piano key sign - depressing the prominent ulnar head produces a "bouncy" rebound, indicating DRUJ instability
- DRUJ stress test - with elbow at 90 degrees, anteroposterior translation applied to the distal ulna in neutral, pronation, and supination - compare to contralateral side
Neurological examination (from Rosen's Emergency Medicine):
| Nerve | Motor Test | Sensory Test |
|---|---|---|
| Radial | Wrist extension | Thumb and first finger web space |
| Ulnar | Wrist flexion + adduction | Little finger |
| Median | Wrist flexion + abduction | Thumb, index, middle fingers |
| Anterior interosseous | Distal phalanx flexion (thumb + index finger) | None |
7. Investigations and Evaluation
Plain Radiographs (First-Line)
Obtain:
- AP and lateral of the entire forearm (from elbow to wrist)
- AP and lateral of the wrist
Radiographic findings to look for:
On the AP view:
- Fracture of the radial shaft at the middle-to-distal third
- Widening of the DRUJ space (>2 mm - normal is 1-2 mm)
- Radial shortening (>5 mm relative to the ulna compared with the contralateral side indicates DRUJ disruption)
- Fracture at the base of the ulnar styloid - avulsion of the TFCC attachment
On the Lateral view:
- Dorsal displacement of the ulnar head relative to the radius
- Dorsal or volar angulation of the radial fracture
The combination AP + Lateral X-ray showing Galeazzi fracture (pre-operative):

AP and lateral views demonstrating a classic Galeazzi fracture-dislocation - Orthobullets
Full forearm X-ray showing displaced Galeazzi fracture:
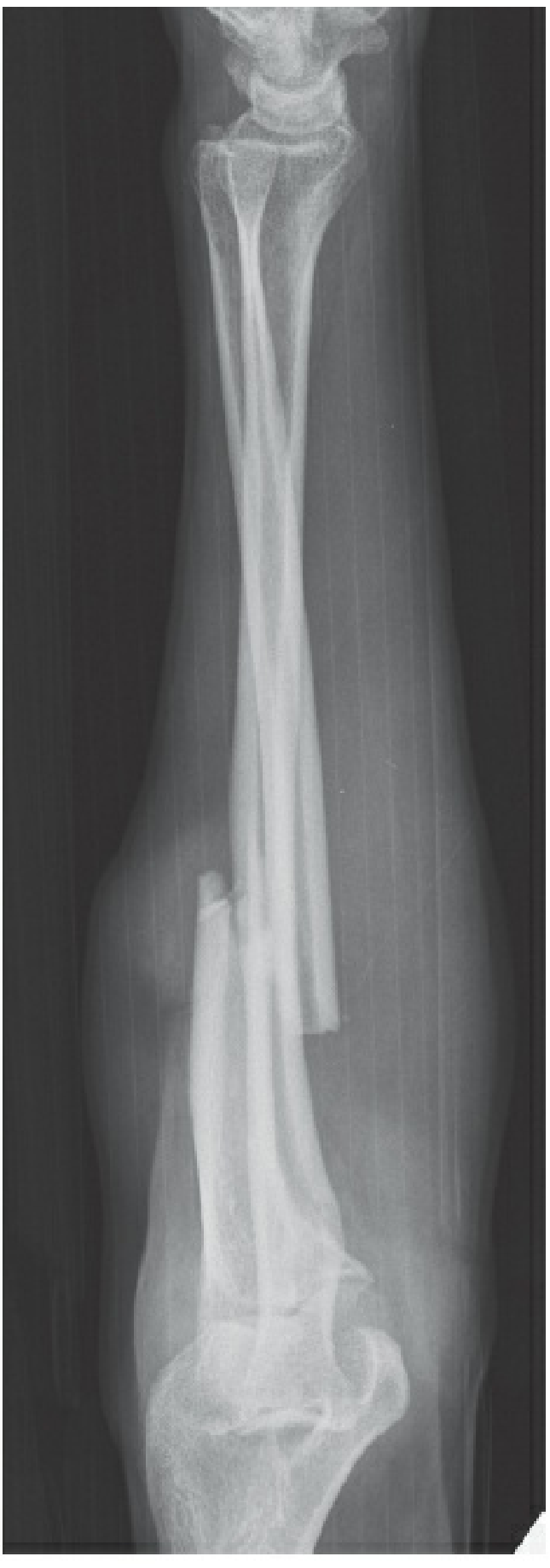
AP radiograph - distal third radial shaft fracture with displacement and DRUJ disruption - Rockwood & Green's Fractures in Adults 10th Ed.
Lateral forearm view showing comminution and DRUJ involvement:

Lateral view with comminuted radial fracture - Rockwood & Green's
Radiographic Signs Summary Table
| Finding | View | Significance |
|---|---|---|
| Radial shaft fracture (distal 1/3) | AP + Lateral | Primary injury |
| DRUJ widening >2 mm | AP | DRUJ disruption |
| Radial shortening >5 mm | AP | DRUJ torn |
| Ulnar styloid base fracture | AP | TFCC avulsion |
| Ulnar head dorsal dislocation | Lateral | DRUJ dislocated |
CT Scan
- Not routinely required for diagnosis
- Indicated when DRUJ incongruity is uncertain on plain films
- Useful for pre-operative planning in complex or comminuted fractures
- Helps visualize intra-articular extension, bony interposition in DRUJ
MRI
- Rarely needed acutely
- Valuable for evaluating TFCC tear extent when surgical DRUJ repair is planned
- Can identify IOM tears when Essex-Lopresti injury is suspected
Intraoperative Assessment
Post-fixation of the radius, DRUJ stability is assessed under fluoroscopy and direct examination:
- Test AP translation at neutral, pronation, and supination
- Compare to contralateral side
- If DRUJ remains unstable after good radial fixation - suspect soft tissue interposition (ECU, EDC, EDQ tendons, periosteum, or avulsed TFCC fragment)
8. Treatment
Principle: "Fracture of Necessity"
Campbell's famous term "fracture of necessity" captures the fundamental principle: in adults, operative treatment is mandatory. Closed reduction and casting in adults universally fail because the deforming forces (PQ, brachioradialis, APL, EPB) cannot be controlled in a cast, leading to re-displacement.
In children: Closed reduction and long-arm casting can succeed because periosteal integrity is maintained and deforming muscle forces are less powerful.
Adult Treatment Algorithm
Galeazzi Fracture (Adult)
│
▼
ORIF of Radial Shaft
(3.5-mm DCP via volar Henry approach)
│
▼
Fluoroscopic assessment of DRUJ
│
┌───┴───┐
Stable DRUJ Unstable DRUJ
│ │
▼ ┌───┴───┐
Long-arm Reducible? Not Reducible
splint in │ (soft tissue
supination Yes │ interposition)
3-6 weeks │ │
┌──┴──┐ Open DRUJ
Large TFCC reduction
ulnar injury + TFCC repair
styloid │
fragment │
│ K-wire
ORIF transfixation
styloid (2 wires,
supination,
4 weeks)
Step-by-Step Surgical Management
Step 1: Fixation of the Radial Shaft (ORIF)
Approach: Volar Henry (anterior) approach in most cases because the fracture is in the distal half of the radius. The Thompson (dorsal) approach is used in some centers to reduce risk of reduced pronation.
Implant: 3.5-mm dynamic compression plate (DCP) - the gold standard. Provides rigid, anatomic fixation.
Key principle: Anatomic reduction of the radial shaft in the majority of cases will automatically reduce the DRUJ.
Post-operative X-ray after ORIF showing plate and screw fixation:

Pre- and post-operative radiographs of Galeazzi fracture ORIF with 3.5-mm DCP plate - Orthobullets
Step 2: DRUJ Assessment After Radial Fixation
With elbow at 90 degrees, test DRUJ stability:
- Stable (remains reduced through pronation/supination): immobilize in supination x 3-6 weeks
- Unstable but reducible: treat based on cause (see below)
- Irreducible: open DRUJ - remove interposing structure, then stabilize
Step 3: Management of DRUJ Instability
Option A - K-wire transfixation:
- Two 2-mm K-wires placed 1 cm apart, just proximal to sigmoid notch
- Forearm in supination
- Immobilize x 4-6 weeks, then remove wires
- "Four cortices" to allow removal if wire breaks
Option B - TFCC repair:
- Open DRUJ via chevron incision over EDQ tendon
- Primary repair of the TFCC and radioulnar ligaments
- Stabilization with sutures through the fovea
- Excellent results in 95% when performed
Option C - ORIF of ulnar styloid base fracture:
- When a large styloid fragment exists (TFCC attached to it)
- Tension band wiring or small fragment screw
- Restores TFCC attachment and DRUJ stability
Post-Operative Immobilization
| DRUJ Dislocation Direction | Immobilization Position |
|---|---|
| Dorsal (most common) | Supination |
| Volar | Pronation |
| Uncertain | Neutral or position of maximum stability |
Duration: 3-6 weeks in long-arm splint or cast, followed by supervised physiotherapy.
Pediatric Management
- Closed reduction under sedation/anesthesia
- Long-arm casting in supination x 4-6 weeks
- Surgical intervention is rarely needed
- Close follow-up with serial X-rays to ensure maintained reduction
9. Complications
| Complication | Notes |
|---|---|
| Malunion | Most common - from inadequate reduction or implant failure |
| Nonunion | Less common with rigid fixation |
| DRUJ instability (chronic) | Pain with rotation, weakness, late arthritis |
| Radioulnar impingement | From malunion causing abnormal biomechanics |
| Infection | Wound infection, osteomyelitis |
| Nerve injury | AIN palsy (thumb IP flexion weakness), superficial radial nerve |
| Tendon rupture | Extensor pollicis longus rupture (rare, similar to distal radius) |
| Compartment syndrome | Rare, watch for in high-energy injuries |
| Re-fracture | After implant removal |
| Essex-Lopresti | Missed associated injury = catastrophic longitudinal instability |
Prognosis with adequate surgery:
- Anatomic reduction of radius + stable DRUJ = good/excellent outcomes in 80-92% of patients
- Primary TFCC repair = excellent results in up to 95% of patients
10. Key Summary Points
| Feature | Detail |
|---|---|
| Definition | Distal 1/3 radial shaft fracture + DRUJ dislocation |
| Mechanism | FOOSH in hyperpronation (most common); direct blow |
| Deforming forces | Pronator quadratus, brachioradialis, APL, EPB |
| Key sign | Prominent ulnar head ("piano key sign") |
| Radiograph | AP: DRUJ widening, radial shortening, ulnar styloid fracture; Lateral: dorsal ulnar dislocation |
| DRUJ unstable if | Fracture <7.5 cm from wrist (55% risk) |
| Adult treatment | ORIF mandatory (DCP via Henry approach) |
| Pediatric treatment | Closed reduction + long-arm cast usually sufficient |
| Post-op immobilization | Supination (dorsal dislocation); Pronation (volar dislocation) |
| Eponym | "Fracture of necessity" (Campbell) |
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th Ed. - Galeazzi Fracture chapter
- Tintinalli's Emergency Medicine: A Comprehensive Study, 9th Ed. - Galeazzi's Fracture-Dislocation
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Fractures of the Distal Third of the Radius with DRUJ Dislocation
- Rockwood and Green's Fractures in Adults, 10th Ed. (2025) - Repair of Galeazzi Fracture Dislocations
- Miller's Review of Orthopaedics, 9th Ed. - Distal-third radius fracture with radioulnar dislocation
This is a shared conversation. Sign in to Orris to start your own chat.