Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG electrocardiogram waveform components P wave QRS T wave
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive guide to ECG basics and interpretation, drawn from Goldman-Cecil Medicine, Costanzo Physiology, and Braunwald's Heart Disease.
What is an ECG?
The electrocardiogram (ECG/EKG) records tiny voltage differences on the body surface that reflect the timing and sequence of cardiac depolarization and repolarization. Because different parts of the myocardium activate at different times (atria before ventricles, specific ventricular sequences), measurable potential differences arise between electrode sites.
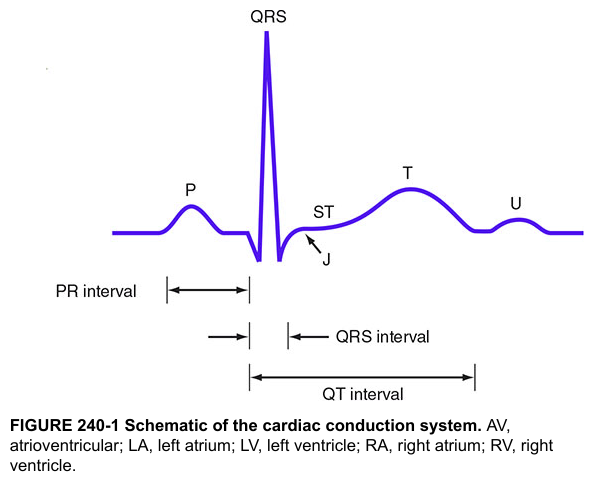
The ECG Waveform
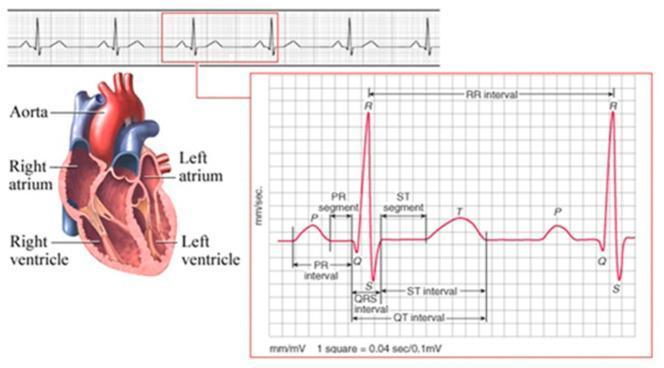
| Wave/Segment | Represents |
|---|---|
| P wave | Atrial depolarization |
| PR segment | Conduction through AV node (isoelectric) |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization |
| T wave | Ventricular repolarization |
| U wave | Possibly Purkinje fiber repolarization (not always seen) |
| J point | Junction of QRS end and ST segment start |
Atrial repolarization is not visible on a normal ECG — it is buried within the QRS complex.
Normal Intervals (Table 42-1, Goldman-Cecil)
| Parameter | Normal Range |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 0.12 sec (120 ms) |
| PR interval | 0.09–0.20 sec (90–200 ms) |
| QRS duration | 0.075–0.11 sec (75–110 ms) |
| QTc (male) | 390–450 ms |
| QTc (female) | 390–460 ms |
| QRS axis | −30° to +90° |
Paper Speed & Grid
- Horizontal axis (time): 1 small box = 0.04 sec; 1 large box = 0.2 sec
- Vertical axis (voltage): 1 small box = 0.1 mV; 10 mm = 1 mV
Heart Rate Calculation
- Formula: HR = 60,000 ÷ RR interval (ms)
- Quick method: Count large boxes between R waves → 1 box = 300 bpm, 2 = 150, 3 = 100, 4 = 75, 5 = 60, 6 = 50
The 12 Leads
A standard ECG has 12 leads recorded over 10 seconds:
Limb leads (frontal plane):
- Bipolar: I, II, III
- Augmented unipolar: aVR, aVL, aVF
Precordial leads (horizontal plane):
- V1–V6 across the chest wall
Lead groupings for regional analysis:
| Region | Leads |
|---|---|
| Septal | V3, V4 |
| Anterior | V2, V3, V4 |
| Lateral | I, aVL, V5, V6 |
| Inferior | II, III, aVF |
QRS Axis
- Normal: −30° to +90°
- Left axis deviation (LAD): −30° to −90°
- Right axis deviation (RAD): +90° to +180°
Quick method: If QRS is positive in both leads I and II → axis is normal.
QTc (Corrected QT)
The QT interval varies with heart rate and must be corrected. Bazett's formula:
QTc = QT ÷ √RR (RR in seconds)
Prolonged QTc raises risk of Torsades de Pointes. Measured in leads II, V5, V6 — report the longest value.
Stepwise Approach to ECG Interpretation
(Goldman-Cecil Medicine, Table 42-2)
- Estimate heart rate
- Rhythm: regular vs. irregular
- P waves: present? morphology, axis, duration
- P-QRS relationship: 1:1? PR interval consistent?
- Pauses or premature beats
- Measure intervals: PR, QRS, QT/QTc
- QRS axis: estimate from limb leads
- QRS progression: R-wave transition in V1→V6 (normally at V3–V4)
- Regional QRS analysis: Q waves, voltage, bundle branch patterns
- ST segments: elevation or depression (regional groupings)
- T waves: morphology, concordance/discordance with QRS
Key Clinical Pearls
| Finding | Significance |
|---|---|
| PR > 200 ms | 1st-degree AV block (AV conduction delay) |
| Short PR | Pre-excitation (WPW), junctional rhythm |
| Wide QRS > 120 ms | Bundle branch block or ventricular rhythm |
| LBBB (new) | High-risk — evaluate for cardiac disease |
| ST elevation | Myocardial infarction, pericarditis |
| QTc prolongation | Risk of Torsades; drug effects, electrolyte disturbances |
| J wave (Osborn) | Hypothermia, hypercalcemia |
| Broad P wave | Intra-atrial conduction delay, atrial enlargement |
Sources: Goldman-Cecil Medicine (International Ed.), Chapter 42 — Electrocardiography; Costanzo Physiology 7th Ed., Chapter 4; Braunwald's Heart Disease, 2-Vol Set; Harrison's Principles of Internal Medicine, 21st Ed.
Would you like to go deeper into any specific area — arrhythmias, bundle branch blocks, ischemia patterns, axis deviation, or lead placement?
This is a shared conversation. Sign in to Orris to start your own chat.