Inguinal canal anatomy in depth with surgical relevence master me in this topic
Reading File
Finding Sources
Finding Sources
Searching the Web
inguinal canal anatomy surgical relevance layers walls contents 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile the definitive master-level response.
The Inguinal Canal: A Master-Level Anatomy & Surgical Reference
Sources: Bailey & Love's Surgery 28e, Fischer's Mastery of Surgery 8e, Mulholland & Greenfield's Surgery 7e, Schwartz's Principles of Surgery 11e, THIEME Atlas of Anatomy, Campbell-Walsh Urology
1. Overview and Embryological Basis
The inguinal canal is an oblique intermuscular passage, approximately 4-6 cm long, running downward and medially through the lower anterior abdominal wall, just above the inguinal ligament. It begins at the deep (internal) inguinal ring and ends at the superficial (external) inguinal ring.
Its existence is a direct consequence of testicular descent. During fetal life, the testis descends retroperitoneally from the posterior abdominal wall, dragging with it a tube of peritoneum - the processus vaginalis - which passes through the abdominal wall layers to form the canal. The processus vaginalis normally obliterates after birth. Failure of this obliteration is the embryological basis for indirect inguinal hernia - which is why all inguinal hernias in children are indirect. The peritoneal tube that wraps around the testis forms the tunica vaginalis; partial obliteration produces a communicating hydrocele.
In females, the round ligament of the uterus passes through the canal to insert into the labia majora - the canal is smaller but the same anatomical principles apply.
2. Boundaries of the Inguinal Canal
The canal has four walls, a floor, a roof, and two openings.
| Structure | Component |
|---|---|
| Anterior wall | External oblique aponeurosis (entire length); reinforced laterally by internal oblique fibres |
| Posterior wall | Transversalis fascia (entire length); reinforced medially by conjoint tendon (falx inguinalis) |
| Floor (inferior wall) | Inguinal ligament (inrolled lower free edge of external oblique aponeurosis = Poupart's ligament) |
| Roof (superior wall) | Arching fibres of internal oblique and transversus abdominis |
Key surgical point: The anterior wall is weak medially (where the superficial ring is); the posterior wall is strong medially (reinforced by the conjoint tendon). Conversely, the anterior wall is strong laterally (external oblique + internal oblique). This complementary reinforcement pattern is what normally prevents herniation.
3. The Two Rings
Deep (Internal) Inguinal Ring
- An oval defect/outpouching in the transversalis fascia, at the midpoint of the inguinal ligament (midway between the ASIS and pubic tubercle), approximately 1.25 cm above this ligament
- The inferior epigastric vessels run just medial to it - this is the most important surgical landmark separating direct from indirect hernias
- The transversalis fascia evaginates through this ring to form the internal spermatic fascia around the cord
- The iliopubic tract forms its inferior margin
- Medially: the interfoveolar ligament (thickening of transversalis fascia)
Superficial (External) Inguinal Ring
- A triangular/inverted-V-shaped defect in the external oblique aponeurosis, just above and medial to the pubic tubercle
- Boundaries: medial crus (superomedially), lateral crus (inferolaterally), intercrural fibres (superiorly), reflected inguinal ligament (completes it inferiorly)
- The spermatic cord/round ligament exits here
4. Contents of the Inguinal Canal
Male
The spermatic cord contains:
- Ductus (vas) deferens - muscular tube, rolled feel on palpation
- Testicular artery (from aorta at L2)
- Pampiniform venous plexus - drains to testicular vein (left side drains to renal vein, right to IVC)
- Lymphatics - drain to para-aortic nodes (not inguinal nodes - important oncologically)
- Genital branch of genitofemoral nerve (L1-L2) - runs posterior to the cord, deep to cremasteric fascia; innervates cremaster muscle and lateral scrotum skin
The coverings of the spermatic cord (from inside out) directly reflect the abdominal wall layers:
| Cord covering | Derived from |
|---|---|
| Internal spermatic fascia | Transversalis fascia |
| Cremasteric muscle and fascia | Internal oblique muscle and fascia |
| External spermatic fascia | External oblique investing fascia |
Additional structures in the canal:
- Ilioinguinal nerve (L1) - lies anterior to the cord, exits through the superficial ring
- Processus vaginalis remnant / tunica vaginalis
Female
- Round ligament of the uterus (with its artery, a branch of the uterine artery)
- Ilioinguinal nerve
- Genital branch of genitofemoral nerve
- Lymphatics
5. The Inguinal Ligament (Poupart's Ligament)
Formed by the inrolled inferior free edge of the external oblique aponeurosis running from the ASIS to the pubic tubercle. Its medial end fans out to form:
- Lacunar ligament (Gimbernat's ligament) - triangular, fills the angle between the inguinal ligament and the pectineal line; the medial boundary of the femoral ring
- Pectineal (Cooper's) ligament - thickening of the periosteum/fascia covering the pectineal line; used in McVay repair
6. Key Surgical Ligaments and Structures
| Structure | Description | Surgical use |
|---|---|---|
| Cooper's ligament (pectineal ligament) | Tough fibrous band on the superior pubic ramus/pectineal line | McVay (Cooper's ligament) repair; posterior mesh fixation in TEP/TAPP |
| Iliopubic tract | Thickened band of transversalis fascia running parallel to and behind the inguinal ligament | Inferior border of deep ring; anterior wall of femoral sheath; key landmark in laparoscopic repair |
| Conjoint tendon (falx inguinalis) | Fused aponeurosis of internal oblique + transversus abdominis, inserts on pubic crest/tubercle | Reinforces medial posterior wall; used in Bassini and Shouldice repairs |
| Interfoveolar ligament | Vertical thickening of transversalis fascia medial to deep ring | Medial boundary of deep ring |
Fischer's Mastery note: During a Shouldice repair, it is critical that the rectus abdominis, external oblique, internal oblique, transversus abdominis, and its aponeurosis are identified as separate and distinct layers - they must not be treated as a single "conjoint tendon."
7. Hesselbach's (Inguinal) Triangle
The most surgically important landmark in the groin.
Boundaries:
- Medially: Lateral border of rectus abdominis
- Superolaterally: Inferior epigastric vessels
- Inferiorly: Inguinal ligament (Hesselbach's original description used the pectineal ligament as the base - more useful when viewing from within the abdomen laparoscopically)
Surgical significance: Direct inguinal hernias bulge through Hesselbach's triangle, medial to the inferior epigastric vessels. The floor of the triangle is formed by transversalis fascia and the aponeurosis of transversus abdominis - in a direct hernia, this ballooning of transversalis fascia is termed a "pseudo-sac" (not a true peritoneal sac). The most translucent part of the triangle has no muscle - only peritoneum and transversalis fascia.

Relationships of the deep inguinal ring, inferior epigastric vessels, and femoral canal - Bailey & Love's Surgery
8. Nerve Anatomy - Critical for Surgical Safety
Three Key Anterior Approach Nerves
1. Iliohypogastric nerve (T12-L1)
- Runs in the plane between internal oblique and external oblique
- Crosses the inguinal canal anterosuperiorly
- Cutaneous supply: skin above the pubis and lateral buttock
- At risk during skin incision and when opening external oblique; can be divided or crushed by retractors
- Injury: numbness/pain in suprapubic area
2. Ilioinguinal nerve (L1)
- Lies within the inguinal canal, anterior to the spermatic cord
- Exits through the superficial ring
- Cutaneous supply: medial thigh, base of penis/scrotum, mons pubis/labia majora in females
- Most commonly injured nerve in open hernia repair (ilioinguinal nerve is present in the canal; absent in <3% of the population; arises with iliohypogastric 25% of the time)
- Injury: genital/inner thigh sensory loss
3. Genital branch of genitofemoral nerve (L1-L2)
- Runs posterior to the spermatic cord, deep to cremasteric fascia
- Enters via the deep inguinal ring
- Motor: cremaster muscle (cremasteric reflex)
- Sensory: lateral scrotum/labia majora
- At risk during dissection around the deep ring
Triangle of Pain and Triangle of Doom (Laparoscopic landmarks)
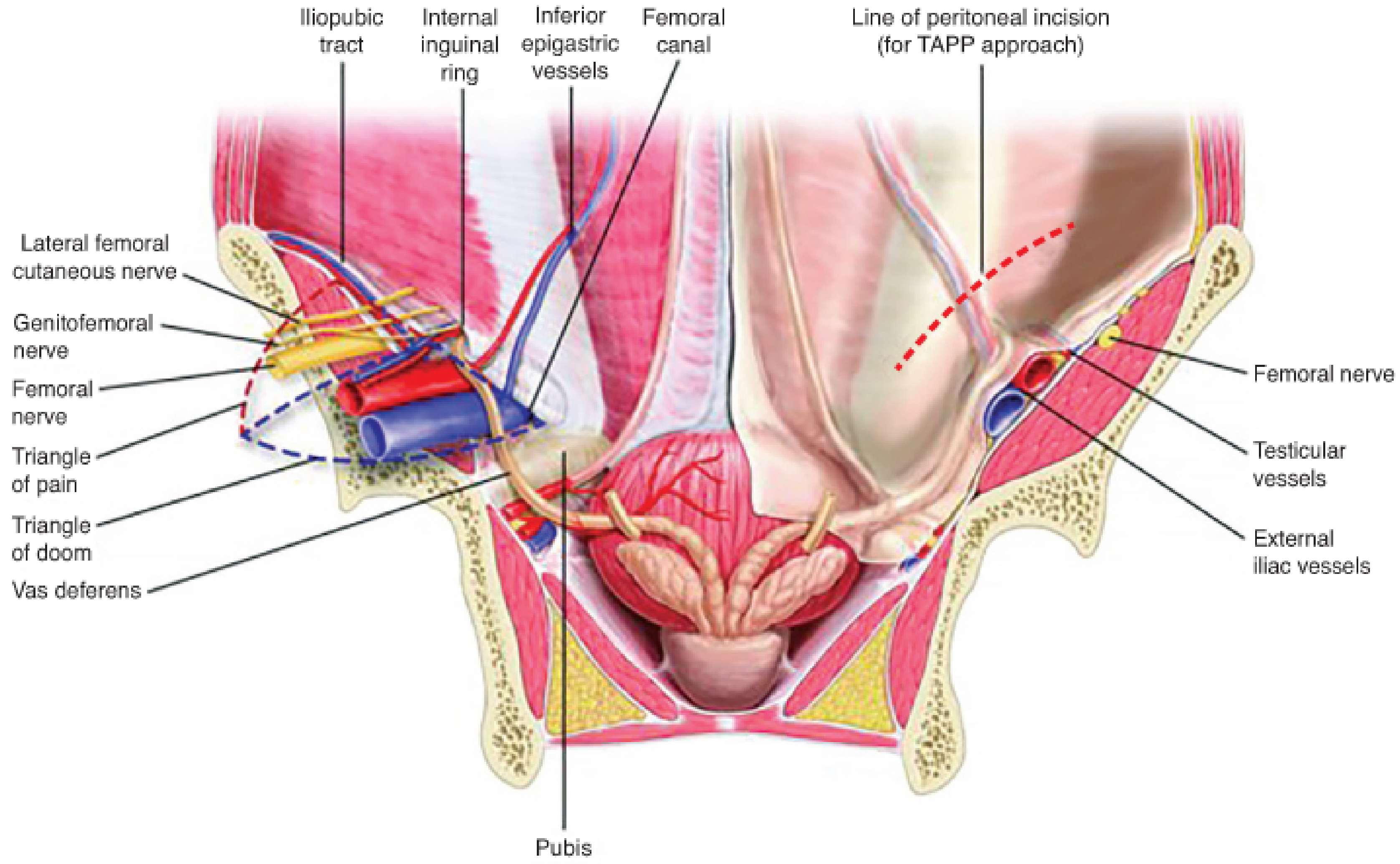
Posterior (laparoscopic) view showing Triangle of Pain, Triangle of Doom, inferior epigastric vessels, and line of peritoneal incision for TAPP - Fischer's Mastery of Surgery
Triangle of Doom (medial to cord, between vas deferens and testicular vessels):
- Contains external iliac artery and vein - potentially catastrophic injury
- Rule: never staple/tack medial to the vas deferens
Triangle of Pain (bounded by gonadal vessels medially, iliopubic tract superiorly, peritoneal reflection inferiorly/laterally):
- Contains: lateral femoral cutaneous nerve, femoral branch of genitofemoral nerve, femoral nerve
- Rule: never staple/tack below the iliopubic tract lateral to the gonadal vessels
9. Mechanism Preventing Herniation
The inguinal canal is an inherent weakness - the following mechanisms normally compensate:
- Obliquity of the canal: The deep and superficial rings do not face each other directly. When intra-abdominal pressure rises, the anterior and posterior walls are pressed together like a "shutter" valve
- Muscular shutter mechanism: Internal oblique and transversus abdominis arch over and contract to compress the deep ring from above ("flap valve")
- Conjoint tendon: Descends to reinforce the medial posterior wall when muscles contract
- Transversalis fascia sling: Surrounds the deep ring like a sling
Failure of any one mechanism predisposes to hernia formation.
10. Types of Inguinal Hernia
Indirect (Lateral) Inguinal Hernia
- Exits lateral to inferior epigastric vessels, through the deep inguinal ring
- Follows the path of testicular descent through the entire canal
- Sac passes within the spermatic cord (covered by all three cord coverings: internal spermatic fascia, cremasteric fascia, external spermatic fascia)
- Can extend all the way to the scrotum (complete/scrotal hernia)
- Congenital (patent processus vaginalis) or acquired (deep ring stretching)
- Most common type in all age groups; more common on the right (delayed right-sided testicular descent)
Direct (Medial) Inguinal Hernia
- Exits medial to inferior epigastric vessels, through Hesselbach's triangle
- Bulges directly through the posterior wall (transversalis fascia)
- Always acquired - due to weakness/atrophy of transversalis fascia with age, COPD, obesity, chronic straining
- Does NOT enter the deep ring; therefore never descends to the scrotum
- Covered by thinned transversalis fascia (pseudo-sac) + external spermatic fascia only - NOT cremasteric fascia
- Lower risk of strangulation compared to indirect
Sliding Hernia
- Retroperitoneal organs form part of the wall of the hernia sac
- On the left: sigmoid colon; on the right: caecum
- The bladder can slide into a direct hernia
- Surgical hazard: bowel/bladder may be mistaken for sac and injured during dissection
Pantaloon Hernia
- Both direct and indirect components coexist, straddling the inferior epigastric vessels
- Bowstringing of the vessels between two sacs gives a "pantaloon" appearance
Femoral Hernia
- Exits through the femoral canal, inferior to the inguinal ligament, medial to the femoral vein
- More common in females (wider pelvis, wider femoral ring)
- High risk of strangulation due to rigid, unyielding ring
- Appears as a lump below and lateral to the pubic tubercle (inguinal hernia is above and medial to pubic tubercle)
11. Classification - European Hernia Society (EHS)
| Code | Meaning |
|---|---|
| P / R | Primary or Recurrent |
| L / M / F | Lateral (indirect) / Medial (direct) / Femoral |
| 1 / 2 / 3 | Defect ≤1 fingerbreadth (≤1.5cm) / 1-3 fingerbreadths / ≥3 fingerbreadths |
Example: PL2 = primary indirect hernia, 1.5-4.5 cm defect
12. Surgical Repairs - A Systematic Overview
Open Non-Mesh (Tissue) Repairs
Bassini's Repair (historical standard)
- Sutures the conjoint tendon to the inguinal ligament (shelving edge of Poupart's)
- Tension-based - largely abandoned due to high recurrence
Shouldice Repair
- Current gold standard for tissue repair; best performed at the Shouldice Hospital (recurrence <1%)
- Four-layer continuous suture technique with stainless steel wire or polypropylene
- Layer 1 & 2: Transversalis fascia divided and double-breasted on itself
- Layer 3 & 4: Internal oblique and transversus abdominis sutured to inguinal ligament
- Requires careful identification of each separate layer (external oblique, internal oblique, transversus abdominis as distinct entities)
- No mesh; suitable for young patients, infected fields
McVay (Cooper's Ligament) Repair
- Sutures the transversus abdominis aponeurosis/transversalis fascia to Cooper's ligament
- Simultaneously repairs direct, indirect, and femoral hernias
- Requires a relaxing incision (in anterior rectus sheath) to reduce tension
Desarda Repair
- A 1-2 cm strip of external oblique aponeurosis is isolated (attached at both ends) and sutured to the conjoint tendon and inguinal ligament
- The strip tightens dynamically with abdominal muscle contraction
- Currently considered equivalent to Shouldice
Open Mesh Repairs
Lichtenstein Tension-Free Repair (most widely performed open repair worldwide)
- Flat polypropylene mesh (8 × 15 cm) placed over the posterior wall of the inguinal canal, posterior to the spermatic cord
- Mesh is slit to wrap around the cord at the deep ring (creating a new deep ring)
- Fixed with loose sutures to the inguinal ligament inferiorly and conjoint tendon superiorly
- Eliminates tension - lower recurrence vs Bassini
- Chronic groin pain: reported up to 20% (mesh-nerve interaction, particularly ilioinguinal nerve)
- Currently recommended by the 2018 European Hernia Society guidelines for unilateral primary inguinal hernia in males
Mesh Plug Repair
- Cone-shaped plug placed in the defect, covered by a flat mesh patch
- Higher risk of mesh migration, meshoma, erosion into bladder
- Not recommended by EHS 2018 guidelines
Laparoscopic Repairs
TEP (Totally Extraperitoneal)
- Balloon dissector develops the preperitoneal (Retzius) space without entering the peritoneal cavity
- Mesh (≥10 × 15 cm) placed in the preperitoneal plane covering the deep ring, Hesselbach's triangle, and femoral canal
- Smaller peritoneal violation risk, but narrow working space; steeper learning curve
TAPP (Transabdominal Preperitoneal)
- Enter the peritoneum first (laparoscopically), then incise peritoneum above hernia defect to access the preperitoneal space
- Better visualization; easier for bilateral hernias and recurrent hernias
- Peritoneum must be closed over the mesh at the end
Advantages of laparoscopic over open (Bailey & Love):
- Reduced acute and chronic pain (up to 5 years post-op)
- Faster return to activity
- Lower wound complication rate
- Particularly beneficial for bilateral hernias and recurrences after previous open repair
- Long learning curve required (80-100 cases for TEP)
Robotic approach: Growing adoption; ergonomic benefits for the surgeon but no demonstrated patient benefit over standard laparoscopic, with significantly higher cost.
13. Laparoscopic View of the Inguinal Region (Posterior Anatomy)
From a posterior (laparoscopic) viewpoint, the key peritoneal folds are:
- Median umbilical fold: Obliterated urachus
- Medial umbilical fold: Obliterated umbilical arteries
- Lateral umbilical fold: Inferior epigastric vessels (the key landmark - medial to deep ring)
The lateral inguinal fossa (lateral to the lateral umbilical fold) = location of the deep inguinal ring = site of indirect hernias.
The medial inguinal fossa (between medial and lateral umbilical folds) = Hesselbach's triangle = site of direct hernias.
14. Complications of Inguinal Hernia Repair
| Complication | Mechanism | Key nerve/structure |
|---|---|---|
| Chronic post-operative inguinal pain (CPIP) | Nerve entrapment in mesh/scar; immediate = fixation injury, delayed = scar entrapment | Ilioinguinal, iliohypogastric, genitofemoral |
| Recurrence | Inadequate repair, tension, missed hernia, inadequate mesh overlap | All types |
| Testicular atrophy | Injury to testicular artery or venous compression by tight deep ring closure | Testicular artery in spermatic cord |
| Vas deferens injury | Inadvertent suturing or diathermy | Vas in spermatic cord |
| Neuropathic pain - lateral thigh | Fixation below iliopubic tract laterally | Lateral femoral cutaneous nerve (Triangle of Pain) |
| Vascular catastrophe | Fixation medial to vas (Triangle of Doom) | External iliac vessels |
| Mesh infection/meshoma | Foreign body, plug migration | - |
| Urinary retention | Spinal anesthesia or local edema | - |
15. Special Considerations
Incarceration vs. Strangulation
- Incarcerated: Hernia contents cannot be reduced; no vascular compromise yet
- Strangulated: Vascular compromise present - surgical emergency; omentum (Richter's hernia - partial bowel wall), small bowel, bladder or ovary can be involved
- Richter's hernia: Only the antimesenteric wall of the bowel is caught - bowel can strangulate without complete obstruction
Paediatric Hernia
- Always indirect; herniorrhaphy (high ligation of the processus vaginalis) is sufficient - no floor repair needed
- Incarceration risk is highest in infants <1 year
- Contralateral exploration: ~30% have patent processus vaginalis on the other side; can be assessed laparoscopically through the hernia sac
Femoral Hernia Management
- All femoral hernias require repair given high strangulation risk
- Approaches: infrainguinal (low approach), transinguinal (through the inguinal canal, McVay), preperitoneal (posterior), laparoscopic
Watchful Waiting
- For asymptomatic/minimally symptomatic inguinal hernias in men, watchful waiting is acceptable
- Sudden onset of pain = emergency repair; elective repair preferred before incarceration
16. Summary Mnemonics
Walls of inguinal canal - "MALT":
- M - Muscles (roof: internal oblique + transversus abdominis)
- A - Aponeurosis (anterior wall: external oblique)
- L - Ligament (floor: inguinal ligament)
- T - Transversalis fascia (posterior wall, + conjoint tendon medially)
Contents of spermatic cord - "3 arteries, 3 nerves, 3 others":
- 3 arteries: Testicular artery, artery to vas (from inferior vesical), cremasteric artery (from inferior epigastric)
- 3 nerves: Genital branch of genitofemoral, ilioinguinal nerve (outside the coverings), autonomic fibres on vas
- 3 others: Vas deferens, pampiniform plexus, lymphatics
Coverings of indirect vs. direct hernia sac:
- Indirect: peritoneum → internal spermatic fascia → cremasteric fascia & muscle → external spermatic fascia (3 layers; sac is WITHIN the cord)
- Direct: peritoneum → thinned transversalis fascia → external spermatic fascia (2 layers; sac is OUTSIDE/adjacent to the cord)
Relation to pubic tubercle:
- Inguinal hernia: above and medial to pubic tubercle
- Femoral hernia: below and lateral to pubic tubercle
Sources: Bailey and Love's Short Practice of Surgery 28th ed., p. 1087-1091 | Fischer's Mastery of Surgery 8th ed., pp. 6045-6170 | Mulholland & Greenfield's Surgery 7th ed., pp. 3632-3655 | THIEME Atlas - General Anatomy, pp. 231-232 | Schwartz's Principles of Surgery 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.