OG 33.1 Classify, describe, and discuss the etiology, pathology, clinical features, differential diagnosis, investigations, and staging of cervical carcinoma, OBG, according to Datta and Shaw's textbook.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the essential content. Let me compile the comprehensive answer.
OG 33.1 - Cervical Carcinoma: Classification, Etiology, Pathology, Clinical Features, Differential Diagnosis, Investigations, and Staging
(Based on Berek & Novak's Gynecology and Robbins & Cotran Pathologic Basis of Disease - the most authoritative OBG/pathology references available; Datta and Shaw's specific text is not in the library but the content below mirrors standard Indian OBG curriculum)
1. CLASSIFICATION
By Histologic Type
| Type | Frequency |
|---|---|
| Squamous cell carcinoma | ~80% |
| Adenocarcinoma | ~15% |
| Adenosquamous carcinoma | Rare |
| Neuroendocrine (small/large cell) | Rare |
| Malignant melanoma, sarcoma | Very rare |
Squamous Cell Carcinoma - Subtypes
- Large cell keratinizing - nests with keratin pearls; best prognosis
- Large cell nonkeratinizing - individual cell keratinization, no pearls
- Small cell type - includes poorly differentiated SCC and small-cell anaplastic carcinoma (resembles oat-cell carcinoma of the lung; worst prognosis)
By Gross Morphology
- Exophytic (fungating) - polypoidal/cauliflower mass projecting out
- Endophytic (infiltrative/ulcerative) - crater-like ulcer or barrel-shaped cervix
- Microinvasive - only detectable by microscopy (stage IA)
2. ETIOLOGY
Human Papillomavirus (HPV) - Primary Cause
- HPV detected in up to 99% of squamous cervical carcinomas
- HPV is causative for both squamous and adenocarcinoma of the cervix
- >100 HPV types exist; >30 affect the lower genital tract
- 15 high-risk subtypes: HPV 16 and 18 account for ~70% of cervical carcinomas
- HPV 16: predominantly squamous carcinoma
- HPV 18: predominantly adenocarcinoma
Mechanism of HPV Carcinogenesis
- E6 viral protein binds and degrades p53 tumor suppressor → prevents cell cycle arrest and apoptosis when DNA is damaged
- E7 viral protein binds Rb (retinoblastoma protein) → disrupts transcription factor E2F → unregulated cell proliferation
- Both steps are essential for malignant transformation of cervical epithelium
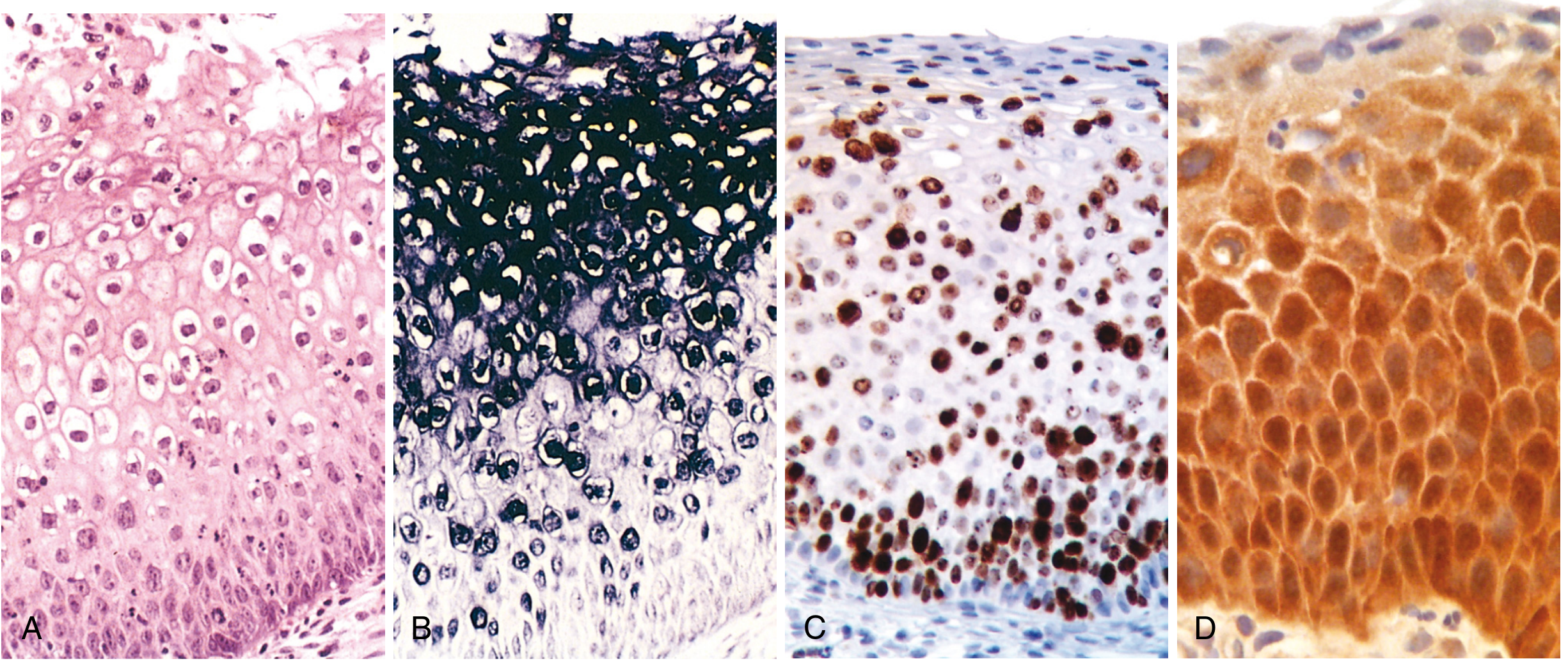
- High-risk HPV also upregulates p16 (CDK inhibitor) - detected on immunohistochemistry as a surrogate marker
Other Risk Factors
| Risk Factor | Comment |
|---|---|
| Young age at first intercourse (<16 years) | Immature metaplastic epithelium at transformation zone is more vulnerable |
| Multiple sexual partners | Increases HPV exposure |
| High parity | Cervical trauma, hormonal effects |
| Cigarette smoking | Carcinogenic metabolites in cervical mucus; local immunosuppression |
| Low socioeconomic status | Limited screening access |
| Chronic immune suppression (HIV/AIDS) | CDC designates cervical cancer as AIDS-defining illness |
| Herpes simplex virus, Chlamydia trachomatis | Co-factors, not primary cause |
| Oral contraceptives | Debated; may increase adenocarcinoma risk |
Rare HPV-Independent Adenocarcinoma
- Gastric-type differentiation, frequent STK11 and TP53 mutations
- Associated with Peutz-Jeghers syndrome (germline STK11 mutations)
3. PATHOLOGY
Gross Pathology
- Early invasive carcinoma: cervix may appear grossly normal or show subtle irregularity
- Advanced disease: exophytic (fungating) cauliflower-like mass or endophytic infiltrating/ulcerative mass
- Barrel-shaped cervix: bulky tumor expanding the endocervical canal
Microscopic Pathology
Squamous Cell Carcinoma:
Nests and tongues of malignant squamous epithelium (keratinizing or nonkeratinizing) invading the underlying cervical stroma.
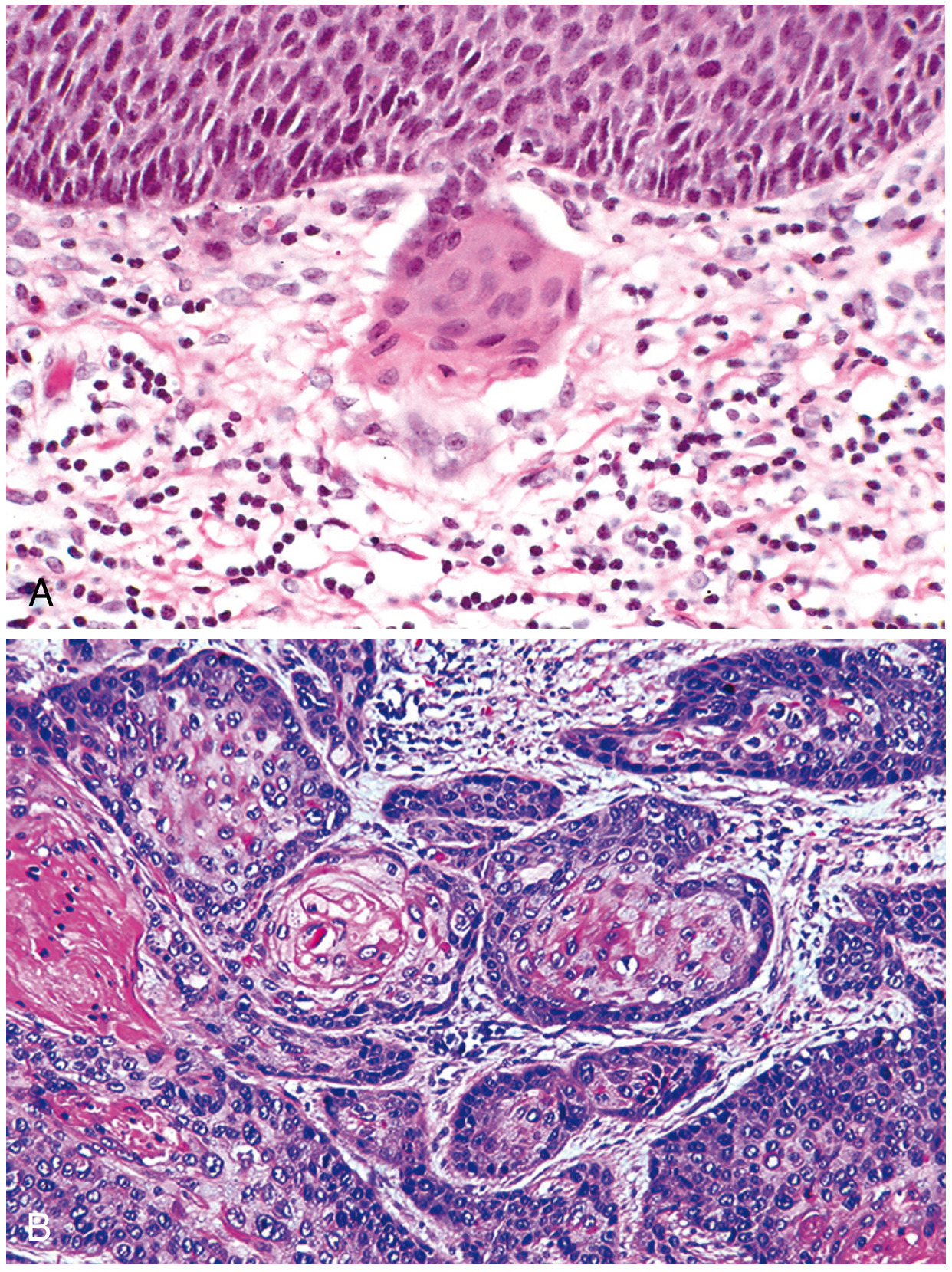
Adenocarcinoma:
- Proliferation of malignant endocervical glandular epithelium
- Large hyperchromatic nuclei with relatively mucin-depleted cytoplasm → dark glands compared with normal endocervix
- ~80% endocervical-type with mucin production
- Remaining: endometrioid, clear cell, intestinal cell types
- Well-differentiated: tall columnar cells lining branching glands
- Poorly differentiated: pleomorphic cells in irregular nests/solid sheets - may need mucicarmine/PAS staining to confirm glandular differentiation
Special variants of adenocarcinoma:
- Minimal deviation adenocarcinoma (adenoma malignum): extremely well-differentiated, may be missed on biopsy, associated with Peutz-Jeghers syndrome
- Villoglandular papillary adenocarcinoma: young women, well-defined borders, superficially invasive, favorable prognosis
Adenosquamous Carcinoma:
- Intermixed malignant glandular AND squamous components
- Poorer prognosis than pure SCC or adenocarcinoma
- Responds well to cisplatin-based chemoradiation
Neuroendocrine Carcinoma:
- Small cell type (resembles pulmonary small cell) and large cell type
- Positive for high-risk HPV - unique among neuroendocrine carcinomas
- Scanty cytoplasm, coarse chromatin, absent/small nucleoli, high mitotic rate
- Aggressive behavior; shorter progression time from in situ to invasive
- Immunohistochemistry/electron microscopy required for diagnosis
Patterns of Spread
- Direct extension: vagina, parametrium, pelvic sidewall, bladder (anterior), rectum (posterior), uterine corpus (superior)
- Lymphatic spread: paracervical → obturator → internal/external iliac → common iliac → para-aortic nodes; Stage IIIC now includes pelvic (IIIC1) and para-aortic (IIIC2) nodal metastasis
- Hematogenous spread: lungs, liver, bones - seen in advanced/recurrent disease
4. CLINICAL FEATURES
Symptoms
| Symptom | Details |
|---|---|
| Abnormal vaginal bleeding | Most common symptom; post-coital bleeding is classic and early; intermenstrual or post-menopausal bleeding |
| Vaginal discharge | Watery, blood-stained, or frankly purulent/offensive in advanced cases |
| Pelvic pain | Indicates parametrial or pelvic sidewall involvement |
| Backache/lower limb pain | Para-aortic node/lumbosacral plexus involvement |
| Dyspareunia | Local invasion |
| Urinary symptoms | Frequency, haematuria, ureteral obstruction causing hydronephrosis (Stage IIIB) |
| Rectal symptoms | Constipation, rectal bleeding, fistula (very advanced) |
| Leg oedema | Lymphatic/venous obstruction from pelvic sidewall disease |
Signs
- Early disease: Cervix may appear normal, or a small erosion/nodule at transformation zone
- Gross tumor: Exophytic cauliflower mass or ulcerated crater, bleeds on contact
- Barrel-shaped cervix: Firm, bulky, barrel-shaped - suggests endocervical growth
- Per vaginal examination: induration of vaginal walls, fornix involvement
- Per rectal examination: parametrial induration, "frozen pelvis" (bilateral parametrial extension to pelvic walls)
- Inguinal lymphadenopathy: rare, indicates advanced disease
- Cachexia, anaemia: advanced/recurrent disease
Colposcopic Findings of Invasion
- Abnormal blood vessels: looped, branched, corkscrew, J-shaped, or reticular vessels - most characteristic finding
- Irregular surface contour: loss of surface epithelium, ulceration, papillary surface
- Color tone change: yellow or orange tinge rather than the normal white aceto-white reaction
- Abnormal vessels show obtuse/right-angle branching with caliber sometimes enlarging after branching (opposite of normal tree-like arborization)
5. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Cervical polyp | Pedunculated, smooth, bleeds on contact; benign on biopsy |
| Cervical ectropion (erosion) | Red granular area around os; no induration; Pap smear normal |
| Nabothian cysts | Smooth, yellowish cysts; benign |
| Chronic cervicitis | Diffuse inflammation, no mass; responds to antibiotics |
| Tuberculosis of cervix | Ulcerative lesion; AFB on biopsy; associated systemic TB |
| Syphilitic chancre | Painless hard ulcer; serological tests positive (VDRL/TPHA) |
| Condylomata acuminata | HPV-related warts; biopsy differentiates |
| Endometrial carcinoma | Post-menopausal bleeding; origin from corpus; D&C/biopsy |
| Vaginal carcinoma | Primary in vaginal wall, not cervix |
| Pelvic inflammatory disease (PID) | No visible mass; responds to antibiotics; bilateral adnexal tenderness |
| Pyometra/hematometra | Distended uterus; no cervical mass per se |
| Cervical pregnancy | Positive pregnancy test; ultrasound shows gestational sac in cervix |
Important: The definitive diagnosis is always histopathology from cervical biopsy. Clinical differentiation alone is insufficient.
6. INVESTIGATIONS
A. Diagnostic Investigations
1. Cervical Cytology (Pap Smear)
- Screening tool; not diagnostic
- Abnormal Pap triggers further evaluation
- ~30% of cervical cancer cases in the US occur in women who never had a Pap smear
2. Colposcopy
- Mandatory for suspected early invasive cancer with grossly normal cervix
- Acetic acid application: reveals acetowhite epithelium, abnormal vascular patterns
- Schiller's iodine test: normal glycogen-rich epithelium stains brown; abnormal areas remain unstained (iodine-negative)
- Colposcopically directed biopsy: can diagnose frank invasion
3. Cervical Biopsy (Punch Biopsy)
- Directed biopsy from most abnormal area under colposcopy
- For visible lesions: direct punch biopsy without colposcopy
- Two biopsy specimens separated by 7 mm both showing invasion → proceed directly to treatment
4. Cone Biopsy (Conization)
- Indicated when: colposcopy is unsatisfactory, biopsy-colposcopy discordance, depth of invasion unclear, suspected stage IA2 vs IB1
- Both diagnostic and therapeutic for microinvasive disease
- LLETZ/LEEP: preferred modality
5. Endocervical Curettage (ECC)
- When squamocolumnar junction is not visible (postmenopausal)
B. HPV Testing
- HPV DNA testing: high-risk HPV types detected by hybrid capture or PCR
- Co-testing (Pap + HPV): preferred screening in women ≥30 years
- HPV 16/18 genotyping: risk stratification
C. Staging Investigations (FIGO 2018 - includes imaging)
Mandatory/Basic:
- Chest X-ray: rule out pulmonary metastases
- Intravenous urography (IVU): hydronephrosis/ureteral obstruction → Stage IIIB
- Cystoscopy: bladder mucosal involvement → Stage IVA
- Proctoscopy/Sigmoidoscopy: rectal mucosal involvement → Stage IVA
- Complete blood count, renal function tests, liver function tests
- Barium enema: for rectal involvement (less commonly used now)
Advanced Imaging (incorporated in FIGO 2018):
- MRI pelvis: gold standard for local staging; assesses tumor size, parametrial invasion, vaginal extension, bladder/rectal involvement, and lymph nodes
- CT chest/abdomen/pelvis: lymph node metastases, distant metastases
- PET-CT: best for detecting nodal and distant metastases; superior sensitivity for lymph nodes
- Ultrasound: limited role; may detect hydronephrosis
- Fine-needle aspiration (FNA): radiographic-guided FNA of enlarged lymph nodes on CT/MRI/PET to confirm metastatic disease
Note: The FIGO 2018 staging now formally incorporates imaging and pathologic measurements (not just clinical examination as in the 2008 system).
Surgical Staging (not universally feasible):
- Pelvic and para-aortic lymph node assessment
- More accurately identifies metastatic disease than clinical staging
- Frozen section analysis of lymph nodes during radical hysterectomy
7. STAGING (FIGO 2018)
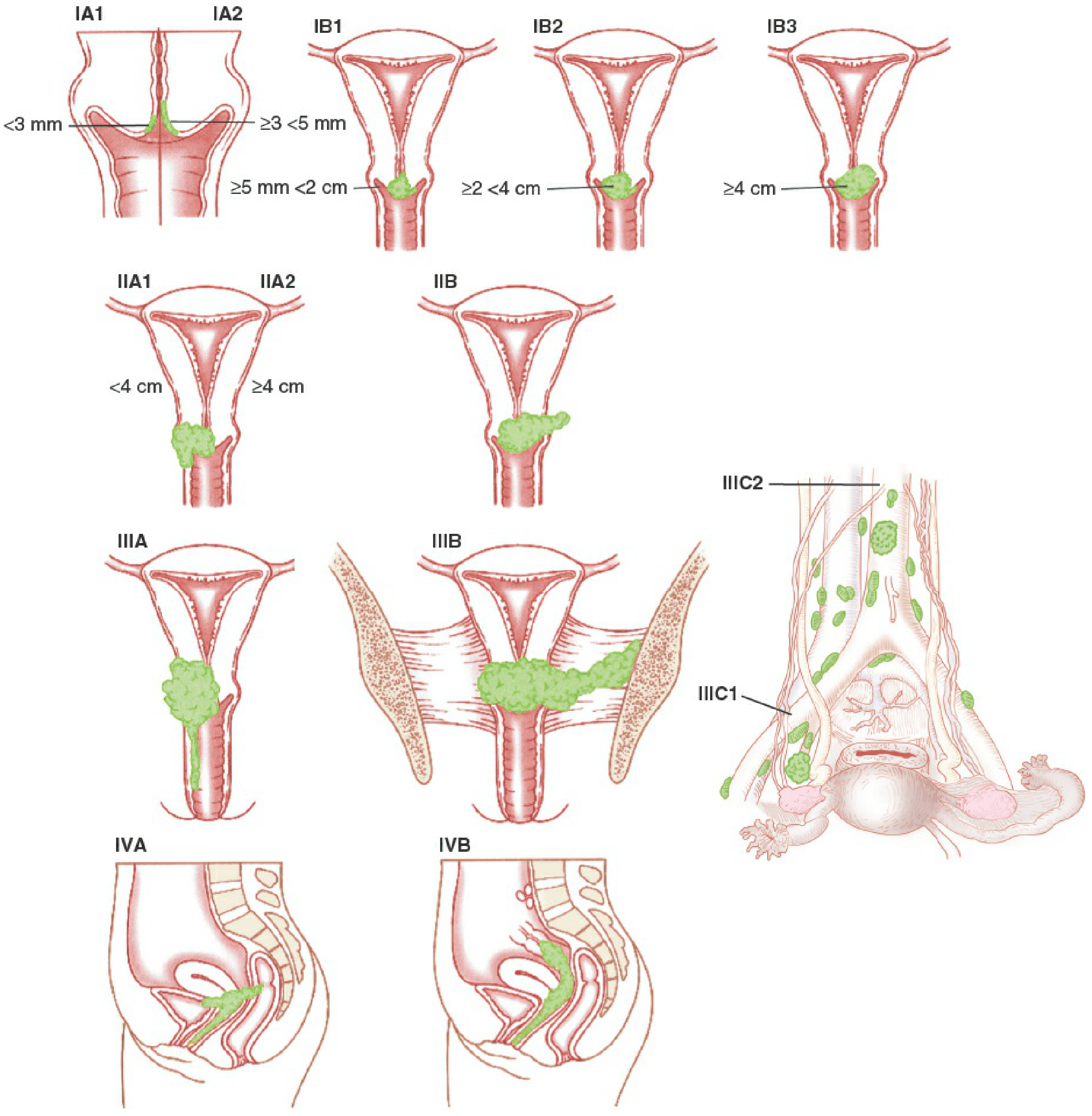
FIGO 2018 Staging System
| Stage | Description |
|---|---|
| I | Carcinoma strictly confined to the cervix (extension to uterine corpus is disregarded) |
| IA | Invasive carcinoma diagnosed ONLY by microscopy; maximum depth of invasion <5 mm |
| IA1 | Measured stromal invasion <3 mm in depth |
| IA2 | Measured stromal invasion ≥3 mm and <5 mm in depth |
| IB | Invasive carcinoma with deepest invasion ≥5 mm, limited to cervix uteri |
| IB1 | Invasive carcinoma ≥5 mm depth, and <2 cm in greatest dimension |
| IB2 | Invasive carcinoma ≥2 cm and <4 cm in greatest dimension |
| IB3 | Invasive carcinoma ≥4 cm in greatest dimension |
| II | Carcinoma invades beyond uterus, but NOT to lower third of vagina or pelvic wall |
| IIA | Upper two-thirds of vagina involved; no parametrial invasion |
| IIA1 | Tumor <4 cm in greatest dimension |
| IIA2 | Tumor ≥4 cm in greatest dimension |
| IIB | Parametrial involvement (but not to pelvic wall) |
| III | Carcinoma extends to lower third of vagina/pelvic wall; causes hydronephrosis; includes node metastasis |
| IIIA | Involvement of lower third of vagina; no extension to pelvic wall |
| IIIB | Extension to pelvic wall AND/OR causes hydronephrosis or non-functioning kidney |
| IIIC | (NEW in 2018) Involvement of pelvic and/or para-aortic lymph nodes |
| IIIC1 | Pelvic lymph node metastasis only |
| IIIC2 | Para-aortic lymph node metastasis |
| IV | Carcinoma has extended beyond the true pelvis or involves mucosa of bladder or rectum |
| IVA | Spread to bladder or rectal mucosa (bullous oedema alone does not qualify) |
| IVB | Distant metastases (including inguinal lymph nodes, peritoneal dissemination, lung, liver, bone) |
Key Changes from FIGO 2008 to FIGO 2018
- Horizontal spread no longer considered in Stage IA - only depth of invasion used (2008 used both depth ≤5mm AND horizontal extent ≤7mm)
- Stage IB subdivided into 3 substages (IB1, IB2, IB3 instead of old IB1 <4cm / IB2 ≥4cm) to better guide fertility-sparing surgery selection
- New Stage IIIC added for lymph node metastasis (pelvic = IIIC1, para-aortic = IIIC2) because lymph node positivity significantly worsens prognosis
- Imaging and pathologic findings formally incorporated (not just clinical examination)
Incidence by Stage at Diagnosis
- Stage I: 38%
- Stage II: 32%
- Stage III: 26%
- Stage IV: 4%
Staging Rules
- When doubt exists about stage allocation, assign the earlier stage
- Once treatment begins, stage must not be changed based on subsequent findings (to avoid falsely improving stage-specific survival statistics)
Sources: Berek & Novak's Gynecology (pp. 2217-2233); Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 924-925)
This is a shared conversation. Sign in to Orris to start your own chat.