Pnd and orthopnea mechanism
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive explanation of both mechanisms:
Orthopnea & Paroxysmal Nocturnal Dyspnea (PND) — Mechanisms
Both symptoms arise from the same underlying problem: elevated pulmonary venous/capillary hydrostatic pressure in the setting of left heart failure. The key difference is timing and severity.
The Shared Pathophysiologic Cascade
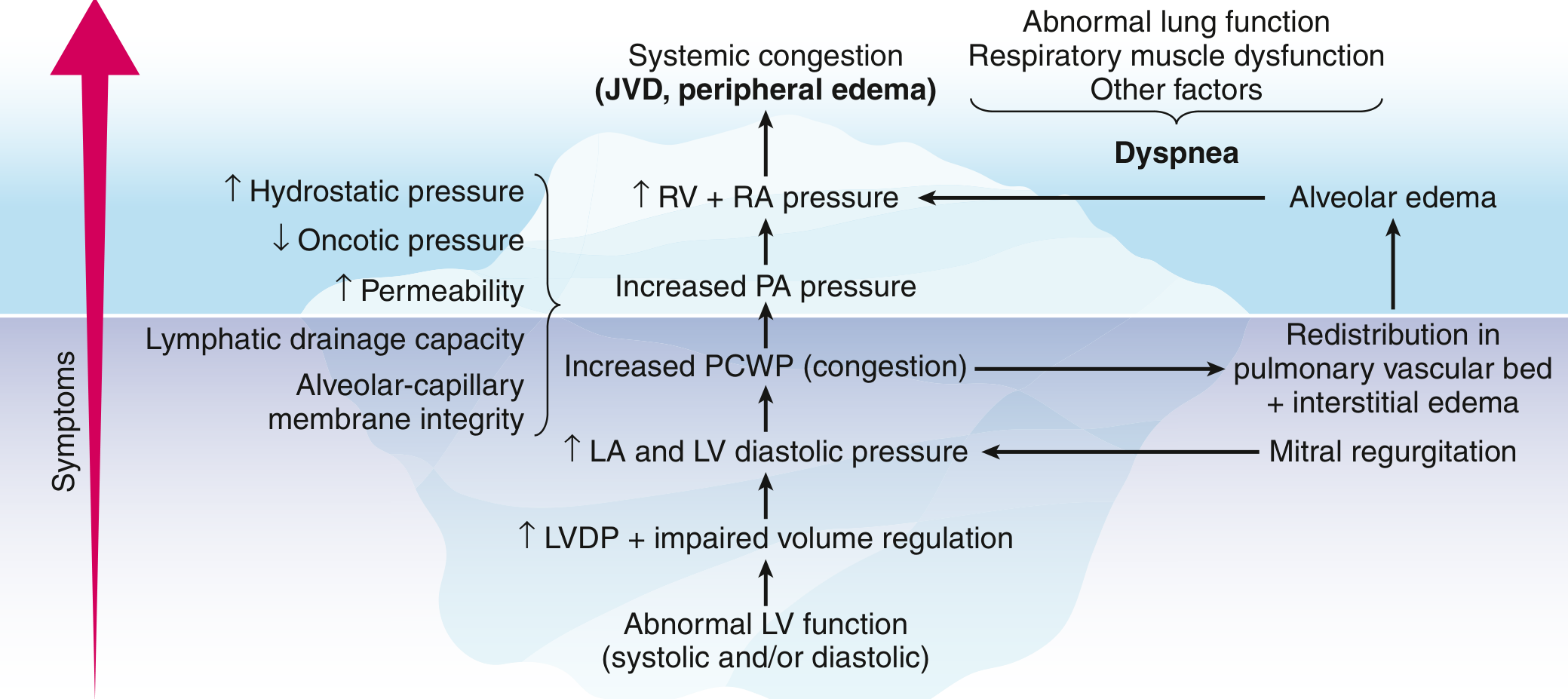
Abnormal LV function → ↑ LV diastolic pressure → ↑ LA pressure → ↑ pulmonary capillary wedge pressure (PCWP) → interstitial/alveolar edema → ↓ lung compliance → ↑ work of breathing → dyspnea
Orthopnea
Definition: Dyspnea that occurs specifically in the recumbent (lying flat) position.
Mechanism:
- When the patient lies flat, gravity no longer pools blood in the lower extremities and splanchnic bed.
- Venous return increases from the extremities and splanchnic circulation to the central (thoracic) circulation.
- This raises ventricular preload, which a failing left ventricle cannot handle.
- Pulmonary venous and pulmonary capillary hydrostatic pressures rise acutely.
- Fluid shifts into the interstitium → reduced lung compliance → increased work of breathing.
Clinical correlate: Graded by "number of pillows" the patient needs to sleep comfortably. Severe orthopnea forces the patient to sleep sitting upright. It correlates well with the severity of pulmonary congestion and is a specific symptom of heart failure.
Paroxysmal Nocturnal Dyspnea (PND)
Definition: Acute, severe shortness of breath that awakens the patient from sleep, typically 1–2 hours after lying down. Relieved by sitting upright or standing.
Mechanism — same trigger as orthopnea, but additional factors make it more dramatic and delayed:
| Factor | Explanation |
|---|---|
| Postural fluid redistribution | Same as orthopnea — recumbency increases venous return and preload |
| Delayed mobilization | Interstitial fluid from the splanchnic bed and lower extremities is gradually absorbed over 1–2 hours after lying down, so the central volume overload builds progressively |
| Alveolar edema | By the time PND strikes, fluid has moved from the interstitium into alveoli — more severe than the interstitial edema of orthopnea |
| Reduced sympathetic tone during sleep | Catecholamine support to the heart falls during sleep, unmasking cardiac decompensation |
| Reduced respiratory drive | Blunted ventilatory response during sleep means more hypoxia accumulates before the patient wakes |
Clinical significance: PND is relatively uncommon compared to orthopnea, but when present it almost always signals severe heart failure and is associated with increased mortality.
Key Differences at a Glance
| Feature | Orthopnea | PND |
|---|---|---|
| Onset | Immediate on lying flat | Delayed ~1–2 hours after sleep |
| Severity | Interstitial edema | Alveolar edema |
| Relief | Sitting up immediately | Sitting/standing; may take 15–30 min |
| Specificity for HF | High | Very high |
| Prognostic weight | Moderate | Higher (associated with ↑ mortality) |
Why PND is Worse Than Orthopnea
The extra severity of PND comes from the time course of fluid mobilization: during sleep, the gradual reabsorption of peripheral edema into the circulation overwhelms the pulmonary lymphatics and Starling forces, tipping the balance from interstitial edema (orthopnea) into frank alveolar flooding (PND). Alveolar edema causes a sudden, dramatic drop in diffusion capacity and triggers the hypoxic/hypercapnic arousal from sleep.
— Goldman-Cecil Medicine International Edition, pp. 467–468
I have a case presentation on rhd with severe ms with severe pah. Enumerate the possible questions and answer that the professors can ask
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
That covers 29 questions across 8 categories from basic science to clinical management. Here's a quick study priority guide:
🎯 Top 5 "Must-Know" Questions Professors Always Ask
- Mechanisms of PAH in MS (Q8) — the 4 mechanisms, especially reactive/"second stenosis"
- Wilkins Score (Q19) — all 4 parameters, cutoffs for PTMC vs surgery
- Auscultatory signs (Q13) — why S1 is loud, A2-OS interval correlating with severity
- Indications for PTMC vs surgery (Q20) — Class I and IIa indications especially
- Warfarin NOT DOACs in MS+AF (Q23) — professors specifically test this distinction
🔑 High-Yield Facts for PAH in Your Case
- Severe PAH (PASP >50 mmHg) is itself an indication for PTMC even in asymptomatic patients
- Reactive PAH reverses after successful PTMC; obliterative PAH does not
- RV failure from PAH significantly increases surgical risk
- The 4-mechanism cascade (passive → reactive → interstitial edema → obliterative) is the signature pathophysiology question for Group 2 PAH due to MS
This is a shared conversation. Sign in to Orris to start your own chat.