CSOM in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic suppurative otitis media"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple top ENT textbooks. Here is the full, detailed answer on CSOM:
Chronic Suppurative Otitis Media (CSOM)
Definition
Chronic suppurative otitis media (CSOM) is a chronic inflammatory condition of the middle ear and mastoid characterized by persistent or recurrent otorrhea through a tympanic membrane (TM) perforation, lasting more than 2-6 weeks. It represents the end-stage sequelae of inadequately treated acute otitis media and Eustachian tube (ET) dysfunction, resulting in mucosal disease, TM damage, and potentially irreversible pathology of middle ear structures.
Epidemiology
- Most common in children under 2 years old
- Closely linked to areas with limited healthcare access and low socioeconomic status
- Risk factors include:
- Multiple prior episodes of acute otitis media (AOM)
- AOM in the first few months of life
- Chronic secretory otitis media
- Genetic predisposition (higher incidence in some indigenous populations)
- Craniofacial abnormalities (e.g., cleft palate)
- Immunodeficiency
Classification (Types)
CSOM is classically divided into two types based on the embryological anatomy of the middle ear cleft (described in the British literature):
1. Tubotympanic (Safe / Benign) Type
| Feature | Details |
|---|---|
| Site of TM involvement | Pars tensa |
| Type of perforation | Central (within pars tensa; margins covered by stratified squamous epithelium) |
| Discharge | Profuse, mucoid, odorless; usually responds to conservative treatment |
| Granulations | Uncommon; if present and unresponsive to treatment, may lead to complications |
| Polyp | Arises from exuberant granulations overlying promontory; can protrude into EAC |
| Hearing loss | Conductive, usually mild |
| Cholesteatoma | Extremely rare |
| Bacteriology | P. aeruginosa, S. aureus, Proteus species |
| Complications | Very unusual except in severely neglected cases |
| Imaging | Haziness of the whole middle ear cleft; truncated pneumatization |
Pathogenesis of pars tensa perforation: Eustachian tube dysfunction causes persistent negative middle ear pressure, leading to atrophy of the pars tensa. Subsequent AOM episodes rupture this weakened area, producing a permanent central perforation. The mucosa may appear boggy with discharge and granulation tissue, or it can remain stable with no mucosal disease.
2. Atticoantral (Unsafe / Malignant) Type
| Feature | Details |
|---|---|
| Site of TM involvement | Pars flaccida or posterior-superior quadrant of pars tensa |
| Type of "perforation" | Retraction pocket of the pars flaccida or posterior-superior quadrant |
| Discharge | Thick, scanty, foul-smelling; usually does not respond to conservative treatment |
| Granulations | Common around the mouth of the retraction pocket |
| Polyp | Usually soft and fleshy, easily suctioned |
| Hearing loss | Larger conductive loss; varying degrees of SNHL |
| Cholesteatoma | Common finding |
| Bacteriology | P. aeruginosa, S. aureus, anaerobes: Bacteroides, Peptococcus, Peptostreptococcus |
| Complications | Frequent; can involve intracranial and extracranial structures |
| Imaging | Scutum erosion (pars flaccida cholesteatoma on CT); medialization of ossicular chain; truncated mastoid pneumatization |
Pathogenesis of atticoantral disease: ET dysfunction causes negative middle ear pressure. The pars flaccida (Shrapnell's membrane) is the most susceptible area of TM to retraction. Retraction of the posterior-superior quadrant forms a pocket that accumulates squamous debris. Adhesions anchor the pocket medially; it loses self-cleansing ability and becomes a cyst. The pocket expands medial to the incus and malleus, forming a cholesteatoma. The ensuing enzymatic activity erodes the ossicular chain (most commonly the long process of the incus) and surrounding bone.
Clinical photographs from Shambaugh Surgery of the Ear showing TM pars tensa perforation and an EAC polyp:

FIGURE: TM perforation of the pars tensa with visible middle ear structures (tubotympanic type)
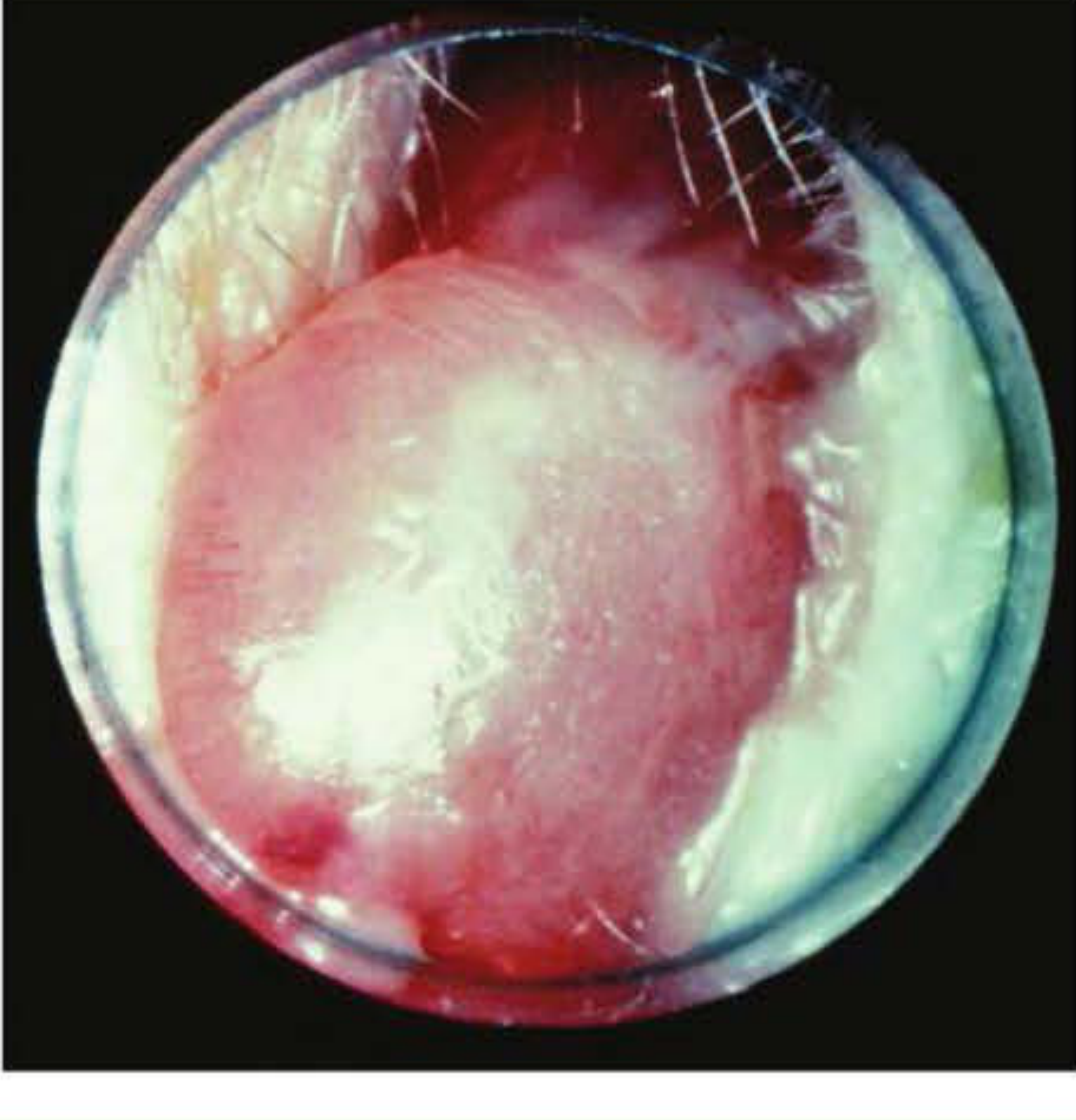
FIGURE: EAC polyp arising from exuberant granulation tissue
Pathogenesis and Pathophysiology
CSOM is initiated by ET dysfunction and the development of a persistent middle ear effusion. The sequence of events:
-
ET dysfunction - Abnormal ET function reduces aeration of the middle ear (ME) space. Nitrogen-absorbing cells in the mastoid cause volume reduction; negative pressure develops in the ME space.
-
Persistent effusion and infection - Serous or purulent effusion leads to mucosal edema. Bacterial infection (particularly polymicrobial) generates an inflammatory response. Chemical mediators promote chronic mucosal changes; the ME mucosa develops submucosal glands converting it to a secretory mucosa, perpetuating the effusion.
-
Granulation tissue formation - Bacterial toxins and inflammatory mediators interact with edematous mucosa, rupturing the basement membrane of the epithelia. Inflammatory cells and lamina propria components extrude into the ME lumen. Angiogenic and epithelial growth factors drive fibroblast recruitment, neovascularization, and polyp formation.
-
TM weakening and perforation - Enzymes in the granulation tissue and chronic effusion degrade the collagen skeleton of the TM. Negative ME pressure combined with a weakened TM causes retraction pockets and eventually perforation. Deep retraction pockets create the conditions for cholesteatoma genesis.
-
Biofilm formation - Bacterial biofilms are common in CSOM. These are highly organized, sessile bacterial communities encased within oligopolysaccharide matrices that:
- Escape phagocytosis and humoral immunity
- Show dramatically increased antibiotic resistance (produce efflux pumps)
- Are frequently polymicrobial
- Elicit ongoing host inflammatory responses via endo- and exotoxins
- Pseudomonas aeruginosa is the most common pathogen in OM biofilms
Microbiology
The bacteriology of CSOM is distinct from AOM and highly likely to harbor multiple organisms:
| Organism | Notes |
|---|---|
| Pseudomonas aeruginosa | Most common in CSOM biofilms |
| Staphylococcus aureus | Very common; including MRSA |
| Proteus species | Common in tubotympanic type |
| Anaerobes (Bacteroides, Peptococcus, Peptostreptococcus) | Common in atticoantral type |
| Haemophilus influenzae, M. catarrhalis | Also reported |
| Candida species | Fungal overgrowth in up to 35% of ears treated with topical fluoroquinolones |
| Propionibacterium acnes | Found in cholesteatoma even without clinical infection |
In cholesteatoma, studies have isolated at least one anaerobic organism in 67% of cases and at least one aerobic organism in 70%. In 57%, multiple organisms were cultured. COM associated with ventilating tubes has a different flora, often beginning with upper respiratory infection or water contamination.
Clinical Features
Symptoms
- Chronic/recurrent otorrhea - The cardinal symptom; may be intermittent, often malodorous (especially in atticoantral type)
- Hearing loss - Typically conductive, low-frequency; a mixed loss may be seen with ossicular erosion or labyrinthine involvement
- Aural fullness
- Otalgia and headache - Uncommon in uncomplicated CSOM; their presence should raise suspicion of intracranial involvement or malignancy
- Vertigo - Should raise suspicion of labyrinthitis or labyrinthine fistula
Signs
- TM perforation (central in tubotympanic; marginal/pars flaccida retraction pocket in atticoantral)
- Otorrhea often obscures the TM
- EAC edema or polyps (an aural polyp should be considered cholesteatoma until proven otherwise)
- Granulation tissue (check for scutal erosion and ossicular erosion)
- Cholesteatoma (pearl-white debris, usually arising from pars flaccida)
- Signs of complications: facial nerve paresis/paralysis, nystagmus, signs of intracranial infection
Audiometry
- Conductive hearing loss most common
- Some patients have SNHL (studies report 5-33 dB SNHL)
- Conductive loss >30 dB suggests ossicular erosion
- Occasionally, hearing can be preserved even with ossicular erosion if sound transmission occurs directly via the cholesteatoma to the oval window
Imaging
CT Temporal Bone (HRCT)
The primary imaging modality for surgical planning. Key findings:
- Tubotympanic type: Haziness of the whole middle ear cleft; truncated pneumatization
- Pars flaccida cholesteatoma: Erosion of the scutum (on axial and coronal bone window CT); medialization of the ossicular chain; truncated mastoid pneumatization

CT scan of temporal bone with pars flaccida cholesteatoma (arrow) showing erosion of the scutum and medialization of ossicular chain - Shambaugh Surgery of the Ear
- Pars tensa cholesteatoma: Erosion of the posterior-superior EAC wall; lateralization of ossicular chain; haziness medial to ossicular chain; possible erosion of the lateral semicircular canal; scutum NOT eroded
Indications for CT:
- Suspected or confirmed cholesteatoma
- Complicated CSOM (facial nerve paralysis, vertigo)
- Surgical planning
- Revision tympanomastoidectomy cases
MRI with Contrast:
Used when intracranial complications are suspected. DWI (diffusion-weighted) MRI is used to identify and follow cholesteatoma (restriction of diffusion in keratin debris).
Complications
Extracranial Complications
| Complication | Notes |
|---|---|
| Coalescent mastoiditis | Air cell septa eroded, pus collects in mastoid |
| Subperiosteal abscess | Pus tracks through mastoid cortex |
| Bezold abscess | Pus tracks through mastoid tip into deep neck |
| Temporal abscess | Pus tracks to temporal root |
| Petrous apicitis (Gradenigo syndrome) | Triad: otorrhea, retroorbital pain, abducens nerve palsy |
| Labyrinthine (perilymph) fistula | Erosion of semicircular canal; presents with vertigo, SNHL |
| Facial nerve paralysis | Dehiscent canal or cholesteatoma erosion of facial canal |
| Acute suppurative labyrinthitis | Progression beyond fistula; profound SNHL |
| Encephalocele / CSF leak | Tegmen erosion |
Intracranial Complications
| Complication | Notes |
|---|---|
| Meningitis | Most common intracranial complication |
| Brain abscess | Temporal lobe or cerebellar abscess |
| Subdural empyema | Pus between dura and arachnoid |
| Epidural abscess | Pus between temporal bone and dura |
| Lateral sinus thrombosis | Sigmoid sinus infected; Tobey-Ayer test |
| Otitic hydrocephalus | Raised ICP without cortical involvement |
| Cerebritis | Early stage; may resolve with treatment |
Intracranial and extracranial complications may result from acute or chronic infections via direct extension through bone (via Haversian canals, air cell tracts, or congenital dehiscences) or hematogenous spread. Cholesteatoma is frequently present in complications of CSOM.
Otalgia and headache in a patient with CSOM are red flag symptoms. Complications carry high morbidity and mortality but significantly decrease with early recognition and treatment.
Diagnosis
- Clinical history and otomicroscopic examination - Detailed history of otorrhea, prior ear surgery, antibiotics used. Otomicroscopy with pneumatic insufflation is the standard
- Audiometry - Full audiometric evaluation (PTA, tympanometry)
- Imaging - HRCT temporal bone (surgical planning, suspected cholesteatoma, complicated CSOM); MRI with contrast for intracranial complications
- Biopsy - Biopsy of granulation tissue unresponsive to topical therapy to rule out malignancy. Remember: persistent CSOM is a recognized risk factor for squamous cell carcinoma of the temporal bone (68% of SCC cases in one series had prior CSOM)
- Microbiological swab - For targeted antibiotic therapy
Treatment
Goals
The primary goal is to create a safe, dry ear:
- Dry = no otorrhea
- Safe = no collection of keratin debris, reduced risk of suppurative complications
Medical Treatment
-
Aural toilet (ear cleansing) - Suction debridement under microscope; removes debris, biofilm, and discharge. This alone can dry the ear in many cases.
-
Topical ototopical antibiotics (first-line):
- Fluoroquinolones (ciprofloxacin or ofloxacin drops) - Drug of choice due to P. aeruginosa coverage and safety profile
- Acetic acid/alcohol - Antiseptic properties, anti-Pseudomonal
- Polymyxin B or neomycin (+/- steroid) - Used with caution (potential ototoxicity if TM perforated)
- Typical course: 4-6 weeks following debridement
- Note: Biofilms are frequently resistant to topical medication due to multicellular defense strategies
-
Systemic antibiotics - Generally reserved for:
- Signs of complications (mastoiditis, facial nerve palsy)
- Inadequate response to topical treatment
- Immunocompromised patients
-
Water precautions - Keep water out of the affected ear
Surgical Treatment
Indications for Surgery
- Cholesteatoma combined with medically refractory CSOM - nearly absolute indication
- Retraction pockets that collect debris and progress
- Persistent otorrhea despite adequate medical treatment (multiple failed attempts)
- Symptoms suspicious for complications (vertigo, facial weakness, headache)
- Atelectatic ears with significant conductive hearing loss
- Hearing restoration
The decision requires a thorough discussion with the patient about: the nature of the disease, surgical risks, risks of continued conservative management, and realistic expectations post-operatively.
Surgical Options
The three priorities of CSOM surgery are:
- Eradication of disease
- Prevention of disease recurrence
- Preservation or restoration of hearing
| Procedure | Indication |
|---|---|
| Myringoplasty / Tympanoplasty | TM perforation repair; 60-90% success rate; best outcome if patient can insufflate through perforation |
| Tympanomastoidectomy | Suspected/confirmed cholesteatoma; refractory otorrhea; goals: remove all cholesteatoma and granulation tissue, restore ME-mastoid continuity |
| Canal wall up (CWU) mastoidectomy | Preserves posterior EAC wall; better hearing outcome; higher recurrence risk; requires staged second-look surgery |
| Canal wall down (CWD) mastoidectomy | Removes posterior EAC wall; wider access to attic/mastoid; exteriorizes unresectable cholesteatoma matrix; lower disease recurrence; requires lifetime cavity maintenance |
| Modified radical mastoidectomy (Bondy) | Preserves ME hearing mechanism where possible; externalizes epitympanic disease |
| Radical mastoidectomy | All ME contents and TM removed; used in extensive disease |
| Atticotomy (transcanal) | Small attic cholesteatoma |
CWU vs. CWD debate:
- CWD offers lower recurrence rates in some studies, but others show the anatomical position of cholesteatoma (not the canal wall) more significantly impacts recurrence
- CWU provides better aesthetics and hearing outcomes but requires strict surveillance
- An open CWD cavity is not aesthetically ideal and requires regular lifetime follow-up and debridement
Eustachian Tube Treatment
No ET treatment method has proven long-term efficacy. Options under investigation include balloon tuboplasty, laser tuboplasty, and ET stenting/implants.
CSOM and Cochlear Implantation
CSOM was historically considered a contraindication to cochlear implantation (CI). Current management options include:
- Staged approach: Stage 1 - radical mastoidectomy with ET obliteration and canal oversewing (±mastoid obliteration); Stage 2 - CI after 3-6 months when ear is dry
- Single-stage: In patients with stable, dry cavity - blind sac closure + CI can be performed simultaneously
- Bacterial and fungal biofilms on CI electrodes are a real risk; Candida species found in 35% of ears treated with topical ciprofloxacin
- All CI candidates with CSOM receive antimicrobial prophylaxis before implantation
- The major risk of canal closure/mastoid obliteration is cholesteatoma formation, which is difficult to monitor post-CI due to MRI artefacts from the device
Key Points Summary
| Feature | Tubotympanic | Atticoantral |
|---|---|---|
| Perforation site | Pars tensa (central) | Pars flaccida / post-sup (marginal retraction) |
| Discharge | Profuse, mucoid, odorless | Scanty, thick, foul-smelling |
| Cholesteatoma | Rare | Common |
| Complications | Rare | Frequent |
| CT finding | Haziness of ME cleft | Scutum erosion (pars flaccida) |
| Bacteria | Pseudomonas, Staph | Pseudomonas, Staph, anaerobes |
| "Safe/Unsafe" | Safe | Unsafe |
Sources:
- Shambaugh Surgery of the Ear, 6th ed. - Etiology, diagnosis, and medical/surgical treatment of CSOM (pp. 527-529)
- Cummings Otolaryngology Head and Neck Surgery - Complications of otitis media (p. 2704)
- K.J. Lee's Essential Otolaryngology, 11th ed. - Epidemiology, etiology, and treatment (pp. 445-447)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - CSOM and temporal bone malignancy (p. 1469)
This is a shared conversation. Sign in to Orris to start your own chat.