Give common heart disease name and their ecg changes and images
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram heart disease changes myocardial infarction atrial fibrillation
Reading File
Finding Sources
Finding Sources
Searching Images
STEMI ST elevation myocardial infarction ECG 12-lead
Searching Images
ventricular hypertrophy ECG changes left right bundle branch block
Searching Images
atrial fibrillation ECG irregularly irregular no P waves
Searching Images
complete heart block third degree AV block ECG
Searching Images
Wolff-Parkinson-White WPW syndrome delta wave ECG
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
I now have comprehensive information and images. Let me compile the complete answer.
Common Heart Diseases & Their ECG Changes
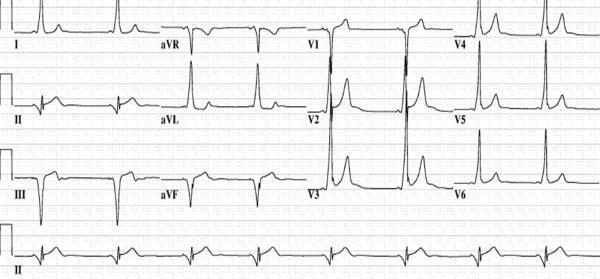
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes:
- Hyperacute T waves — earliest change (tall, peaked T waves)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Pathological Q waves — develops over hours (>0.04 s wide, >25% R wave depth) — sign of necrosis
- T-wave inversion — evolves after acute phase
- Reciprocal ST depression in opposite leads
Localisation by ECG (from Tintinalli's Emergency Medicine):
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anteroseptal | V1–V3 | LAD proximal |
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Lateral | I, aVL | LCx |
| Inferior | II, III, aVF | RCA |
| Posterior | Tall R in V1–V2, R/S ≥1 | LCx/RCA |
| Right ventricular | II, III, aVF + V3R–V6R elevation | RCA |
ECG Images — Anterior STEMI:



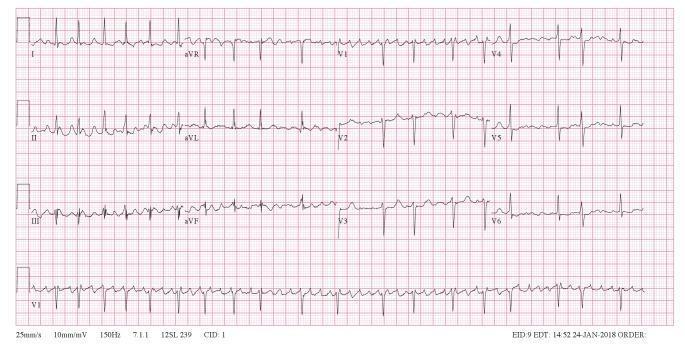
2. 💓 Atrial Fibrillation (AF)
ECG Changes:
- Absent P waves — replaced by chaotic fibrillatory (f) waves (best seen in V1)
- Irregularly irregular R-R intervals — hallmark feature
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Rate: Ventricular response varies; rapid (>100 bpm) = AF with RVR
ECG Images:
3. 🔒 Complete Heart Block (3rd-Degree AV Block)
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes march independently
- P waves regular at faster atrial rate (60–100 bpm)
- Ventricular escape rhythm: slow bradycardia (20–40 bpm)
- Wide QRS if escape from ventricle (>120 ms); narrow if junctional escape
- No fixed PR interval
ECG Images:

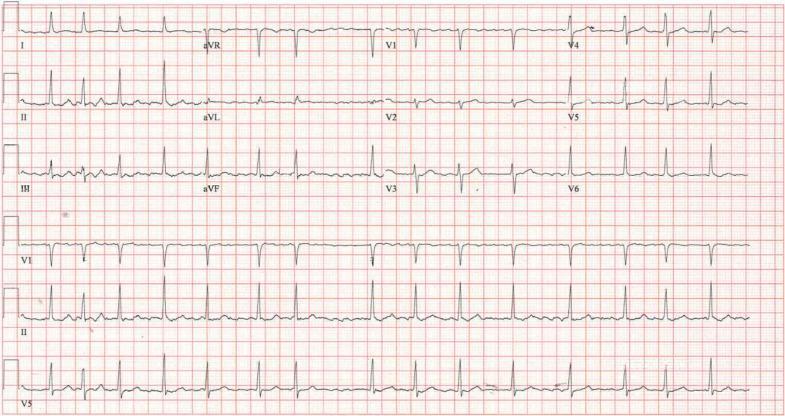
4. ⚡ Wolff-Parkinson-White (WPW) Syndrome
ECG Changes:
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke at beginning of QRS (pre-excitation via accessory pathway)
- Wide QRS (>120 ms) due to fusion beat
- Secondary ST-T changes (discordant with QRS)
- Risk: Pre-excited AF → rapid conduction → VF
ECG Images:

5. 🫁 Pulmonary Embolism (PE)
ECG Changes:
- Sinus tachycardia — most common finding (~40% of cases)
- S1Q3T3 pattern — S wave in lead I + Q wave + T-wave inversion in lead III (right heart strain)
- T-wave inversions V1–V4 — RV strain pattern
- Incomplete/complete RBBB — due to acute RV dilation
- Right axis deviation, P pulmonale
- AF — occurs in 10–35% of patients
ECG Images:


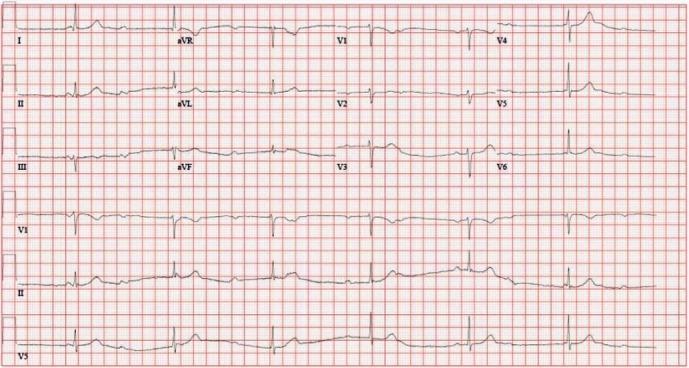
6. 🏋️ Left Ventricular Hypertrophy (LVH)
ECG Changes:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥ 35 mm
- Cornell criteria: R in aVL + S in V3 ≥ 28 mm (men) or ≥ 20 mm (women)
- Left axis deviation
- ST depression + T-wave inversion in lateral leads (V5–V6, I, aVL) — "strain pattern"
- Left atrial enlargement (P-mitrale: wide, notched P wave in II; biphasic P in V1)
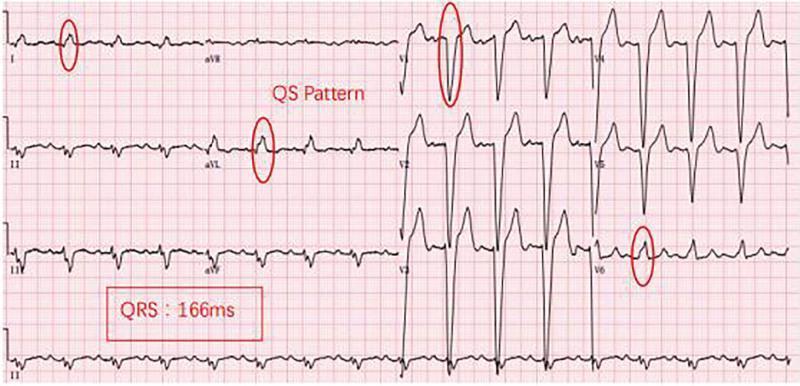
7. 🔀 Left Bundle Branch Block (LBBB)
ECG Changes:
- Wide QRS ≥120 ms
- Broad notched/slurred R in lateral leads (I, aVL, V5–V6) — "M-shaped"
- Deep S/QS in right precordial leads (V1–V3)
- ST and T changes discordant to QRS (opposite direction)
- Loss of normal septal Q waves in lateral leads
- New LBBB in chest pain = STEMI equivalent until proven otherwise
ECG Image:
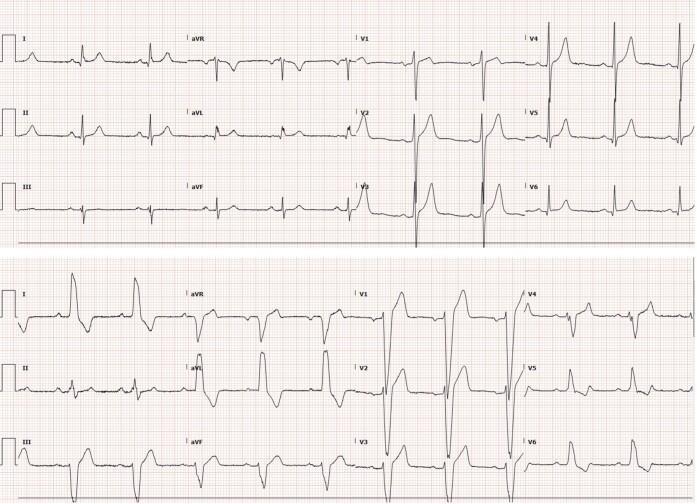
8. ➡️ Right Bundle Branch Block (RBBB)
ECG Changes:
- Wide QRS ≥120 ms
- RSR' ("rabbit ears") pattern in V1–V2
- Broad slurred S wave in lateral leads (I, V5–V6)
- T-wave inversion in V1–V3 (secondary change)
- Can be normal variant or indicate RV pressure overload
ECG Image:
Quick Reference Summary
| Disease | Key ECG Finding |
|---|---|
| STEMI | ST elevation + reciprocal depression + Q waves |
| NSTEMI / Unstable Angina | ST depression / T-wave inversion (no elevation) |
| Atrial Fibrillation | Irregularly irregular, no P waves |
| Complete Heart Block | AV dissociation, slow escape rhythm |
| WPW | Short PR + delta wave + wide QRS |
| Pulmonary Embolism | S1Q3T3 + sinus tachycardia + RBBB pattern |
| LVH | Voltage criteria + lateral strain pattern |
| LBBB | Wide QRS + broad R lateral + QS V1–V3 |
| RBBB | Wide QRS + RSR' in V1 + broad S lateral |
Sources: Tintinalli's Emergency Medicine (9th ed.) — ECG ST-Segment Criteria Table 49-4; Ganong's Review of Medical Physiology; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.