Dynamic elbow orthosis
dynamic elbow orthosis indications design clinical use
"elbow orthosis" AND "dynamic splinting" AND "range of motion"
"elbow orthosis" AND "contracture"
https://pmc.ncbi.nlm.nih.gov/articles/PMC9670792
Dynamic Elbow Orthosis (DEO)
Definition
Classification of Elbow Orthoses
| Type | Mechanism | Goal |
|---|---|---|
| Static | Fixed position at maximum tolerated range | Prevent further loss; maintain end-range |
| Static-progressive | Incremental positional advances | Gain ROM in small steps |
| Dynamic | Constant spring/elastic stretch load | Continuous LLPS to remodel soft tissue |
| Hinged/articulated | Free motion with mediolateral stability | Protect ligaments while allowing flexion-extension |
Mechanism of Action
- Gradual elongation of shortened capsule, ligament, and scar tissue
- Collagen fiber reorientation along lines of stress
- Reduction of fibrotic contracture without exceeding tissue injury thresholds
Indications
Orthopedic / Trauma
- Elbow contractures (flexion or extension) following fractures, dislocations, or prolonged immobilization
- Post-operative rehabilitation (ligament reconstruction, arthroplasty, radial head repair, olecranon fractures)
- Burns causing elbow joint stiffness
- Hemophilic arthropathy with restricted ROM
Neurological
- Cubital tunnel syndrome - extension night splint worn at 45 degrees reduces ulnar nerve stretch during sleep (Campbell's Operative Orthopaedics, 15th ed.)
- Stroke/TBI/SCI with elbow flexor spasticity - assists extension against spastic tone
- Cerebral palsy with elbow flexion pattern
Lateral epicondylitis
- An elbow strap (counterforce brace) is used for lateral epicondylitis; long-arm splinting at 45 degrees of flexion for cubital tunnel syndrome (Miller's Review of Orthopaedics, p. 887)
General criterion
- Pre-splinting ROM typically around 60-72 degrees; studies show average gains of 36-37 degrees, bringing post-splinting arc to ~100-108 degrees (Aetna Clinical Policy)
Design Features
- Hinged medial and lateral uprights anchored to cuffs above (humerus) and below (forearm) the joint
- Spring or tension mechanism at the hinge axis providing the stretch force
- Adjustable tension dial or spring selection to titrate load
- Blocks for varus/valgus stability (especially post-ligament reconstruction)
- Optional ROM stops to limit arc during healing phases
- Worn passively (at rest, during sleep) rather than during active use
Clinical Phases of Use
| Phase | Duration | Role of Orthosis |
|---|---|---|
| Inflammatory (post-op) | 0-2 weeks | Dynamic or static + CPM |
| Proliferative (scar maturation) | 2-6 weeks | Dynamic LLPS; collagen still elongatable |
| Remodeling | 6 weeks - 6 months | Maintain and extend active ROM arc; prevent regression |
| Late (>6 months) | >6 months | Some gains still possible; patience required |
Dynamic vs. Static-Progressive: Which to Choose?
- Static-progressive group: pre-splinting ROM 72 degrees → improved by 36 degrees
- Dynamic group (72 patients): pre-splinting ROM 63 degrees → improved by 37 degrees
- Choice depends on surgeon/patient preference; dynamic orthoses may cause more discomfort due to continuous tension (Cavalcanti et al., Acta Ortop Bras 2022 - PMID 36451794)
Compared to Plaster Splinting
- Significantly better grip strength
- Better Oxford Elbow Scores
- Comparable pain reduction at 6, 12, and 24 weeks
- Advantage: earlier mobility, better circulation, and avoidance of joint stiffness
Contraindications / Precautions
- Severe spasticity or contracture (> ~30-40 degrees fixed) making device fitment difficult
- Acute infection or open wounds at the orthosis contact sites
- Unstable fractures not yet surgically stabilized
- Skin conditions precluding prolonged contact (pressure injury risk)
- Non-compliance (device must be worn consistently for efficacy)
Key Points Summary
- Dynamic spring-loaded orthoses are the preferred non-surgical treatment for elbow flexion and extension contractures (Miller's Review of Orthopaedics, 9th ed.)
- They work by LLPS - collagen creep and stress-relaxation over weeks to months
- Gains are mostly achieved in the first 6 months, but improvement can continue beyond that
- Static-progressive and dynamic orthoses yield similar ROM outcomes; dynamic devices may be less comfortable
- They are also used to assist weak elbow flexors or extensors in neurological patients (stroke, SCI)
- Articulated designs additionally provide mediolateral stability to protect repaired ligaments while permitting flexion-extension
Diagram
Medical diagram of a dynamic elbow orthosis showing: lateral view of a human arm wearing the device with labeled components including: hinged medial and lateral uprights, humeral cuff (upper arm), forearm cuff, spring/tension mechanism at hinge axis, adjustable tension dial, ROM stops, and mediolateral stability blocks. Also show a small inset diagram comparing static vs dynamic vs static-progressive orthosis force-time curves. Clean medical illustration style with clear labels and arrows, white background.
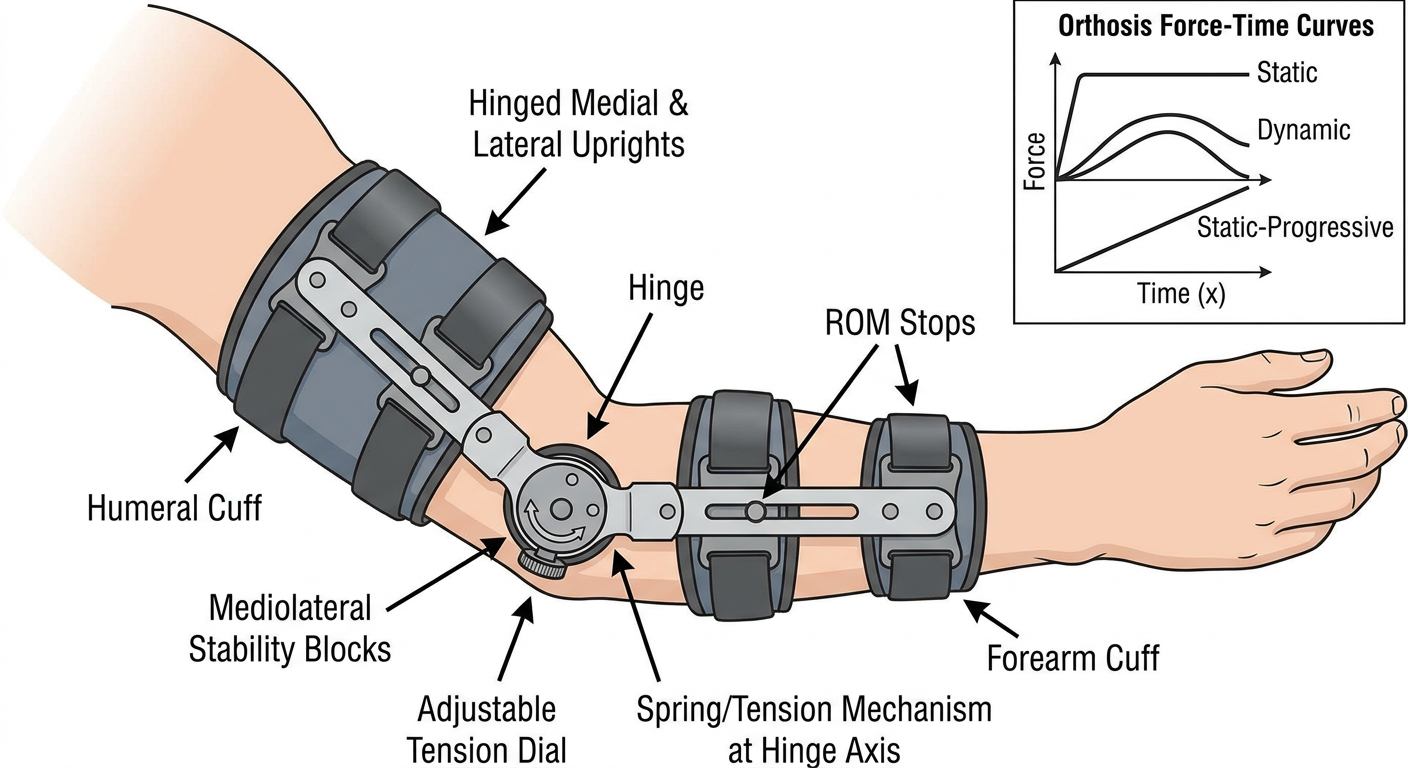
- Humeral cuff - anchors the device to the upper arm
- Forearm cuff - anchors to the forearm/wrist segment
- Hinged uprights (medial and lateral) - run along both sides of the elbow, providing mediolateral stability
- Spring/tension mechanism at the hinge axis - delivers the constant low-load prolonged stretch (LLPS)
- Adjustable tension dial - allows titration of stretch force to patient tolerance
- ROM stops - limit the arc of motion during healing phases
- The inset force-time curves show how a dynamic orthosis maintains constant stretch load, compared to static (single fixed position) and static-progressive (stepwise increments)
Diagram of tennis elbow counter force brace
Medical diagram of a tennis elbow counterforce brace (lateral epicondylitis strap) showing: anterior and lateral view of a forearm wearing the brace positioned about 2-3 cm distal to the lateral epicondyle. Label the following components: counterforce pad (pressure pad over extensor muscle bulk), adjustable velcro strap, brace placement site (2-3 cm distal to lateral epicondyle), and the lateral epicondyle landmark on the humerus. Include a small inset diagram showing the mechanism of action - how the brace compresses the extensor muscle belly, reducing tensile force transmitted to the common extensor origin at the lateral epicondyle. Show wrist extensor muscles (ECRB highlighted). Also include a small anatomical inset showing the painful site (lateral epicondyle) vs brace placement. Clean medical illustration, labeled arrows, white background.
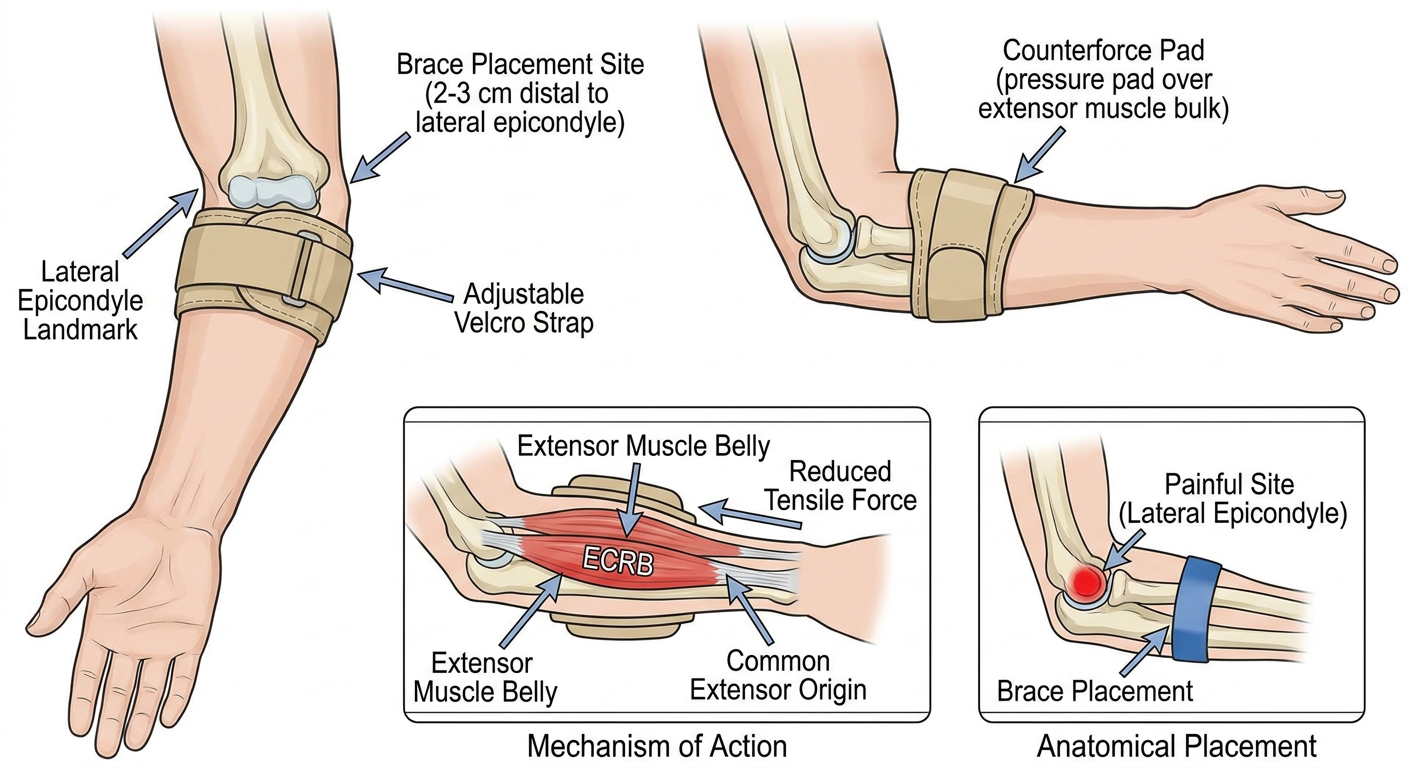
- Worn 2-3 cm distal to the lateral epicondyle - this is critical; placing it directly over the epicondyle defeats the purpose
- Sits over the extensor muscle belly, not over bone
- Counterforce pad - a firm pressure pad that compresses the extensor muscle bulk
- Adjustable Velcro strap - circumferential strap, tightened snugly but not to the point of neurovascular compromise
- The brace compresses the extensor muscle belly (primarily ECRB - extensor carpi radialis brevis), which creates a new "origin point" for the muscle
- This reduces the tensile force and stress transmitted proximally to the common extensor origin at the lateral epicondyle - the site of the tendinopathy
- By offloading the degenerated tendon attachment, pain is reduced during gripping and wrist extension activities
Orthosis tennis elbow counter force brace diagram
Detailed anatomical medical diagram of a tennis elbow counterforce brace orthosis on a right forearm. Show two views side by side: LEFT VIEW - lateral side of elbow and forearm showing the brace worn on the proximal forearm, with the elbow joint and lateral epicondyle visible above the brace. RIGHT VIEW - cross-sectional view through the forearm at the brace level showing how the pressure pad compresses the extensor muscles. Label all key structures: lateral epicondyle, common extensor origin (ECRB tendon - site of pathology), extensor carpi radialis brevis muscle belly, counterforce pressure pad, circumferential velcro strap, brace width (approximately 5-6 cm), placement zone (2-3 cm distal to lateral epicondyle). Add red dot or highlight on lateral epicondyle to mark pain site. Include arrows showing force redirection - tensile stress reduced at origin. Clean, professional medical orthopedic illustration with white background and color coding.
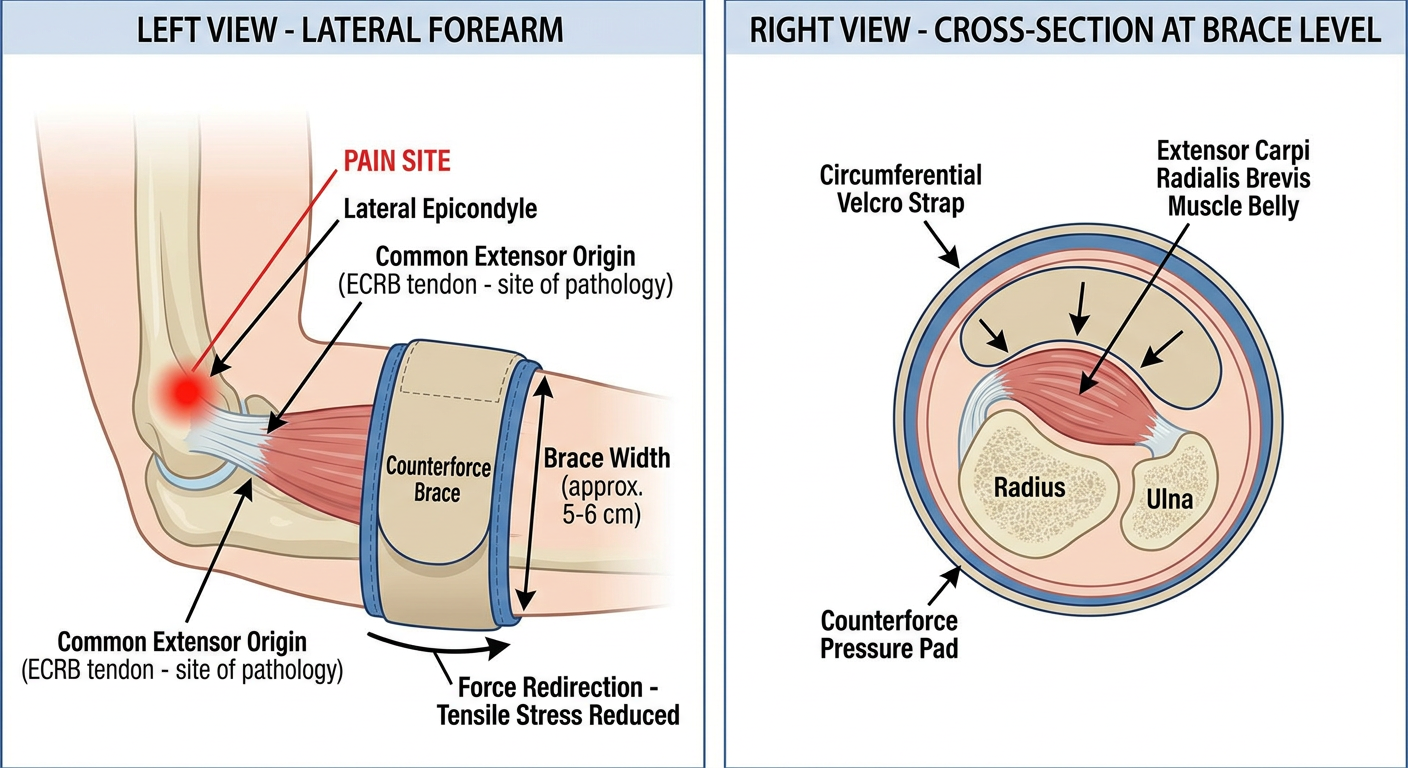
- Red dot marks the lateral epicondyle - the actual pain site
- Brace sits 2-3 cm distal to the epicondyle, over the proximal forearm
- The counterforce pad lies directly over the ECRB muscle belly
- Shows how the pad applies focal compression to the extensor muscle compartment
- The strap distributes circumferential pressure while the pad concentrates force over the extensors
- Compression of the ECRB muscle belly creates a functional new origin distal to the pathological tendon
- Reduces tensile load at the common extensor origin on the lateral epicondyle by up to 30-50%
- Worn during activity (sport, gripping tasks), removed at rest