Screening and diagnosis of OSA from AASM guidelines
Reading File
Finding Sources
Searching PubMed
"obstructive sleep apnea" AND "AASM" AND "diagnosis"
Searching the Web
AASM guidelines screening diagnosis obstructive sleep apnea 2023 2024
Finding Sources
Reading Web Page
https://emedicine.medscape.com/article/295807-guidelines
Reading Article
PMID: 40838698
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive review of OSA screening and diagnosis based on AASM guidelines, synthesized from the 2017 AASM Clinical Practice Guideline (the primary reference, endorsed by the World Sleep Society in 2021), the 2025 AASM Inpatient OSA Guideline [PMID: 40838698], and multiple medical textbooks.
Screening and Diagnosis of OSA - AASM Guidelines
1. Overview of AASM Diagnostic Framework
The AASM distinguishes two stages:
- Screening - identifying patients at increased risk using clinical tools and questionnaires
- Diagnosis - confirming OSA with objective sleep testing (PSG or HSAT)
Core principle: Clinical tools and questionnaires alone cannot diagnose OSA. Objective sleep testing is mandatory for diagnosis.
"Clinical tools, questionnaires and prediction algorithms should not be used to diagnose OSA in adults without polysomnography or home sleep apnea testing (HSAT)." - AASM 2017 Guideline (Strong Recommendation)
2. Screening
Who to Screen
Screening is indicated for patients with:
- Loud snoring (heard through closed doors)
- Witnessed apneas or gasping/choking during sleep
- Daytime hypersomnolence or fatigue
- Obesity (BMI >30 kg/m²) - 70% of OSA patients are obese; screening all obese patients is recommended
- Hypertension, especially drug-resistant
- Crowded upper airway, retrognathia, large neck circumference
- Male sex, age >50 years, menopause in women
Validated Screening Questionnaires
STOP-BANG Questionnaire
The most widely used pre-test screening tool:
| Letter | Question |
|---|---|
| S | Do you Snore loudly? |
| T | Do you often feel Tired, fatigued, or sleepy during the day? |
| O | Has anyone Observed you stop breathing during sleep? |
| P | Do you have or are you treated for high blood Pressure? |
| B | Is your BMI >35 kg/m²? |
| A | Are you Age 50 or older? |
| N | Is your Neck circumference >40 cm (female) / >43 cm (male)? |
| G | Are you Gender male? |
Interpretation:
- Score 0-2: Low risk for OSA
- Score 3-4: Intermediate risk
- Score 5-8: High probability of moderate-to-severe OSA
- The STOP-BANG has high sensitivity but low specificity; it should not replace objective testing
(Cummings Otolaryngology, p. 307; Miller's Anesthesia, p. 8339)
Epworth Sleepiness Scale (ESS)
- Measures subjective daytime sleepiness across 8 situations (0-3 scale each, max 24)
- ESS >10: Clinically significant daytime sleepiness; OSA may be suspected
- Limitation: Not sensitive or specific enough to screen for OSA on its own
- More useful for symptom quantification and treatment monitoring
Berlin Questionnaire
- Validated in primary care settings
- Three categories: snoring/apneas, daytime sleepiness, hypertension/BMI
- High-risk classification if positive in 2+ categories
"The Berlin Questionnaire has been validated in a primary care setting and identifies patients likely to have OSA. Another often used screening questionnaire is the STOP-Bang survey, which has been used in preoperative anesthesia clinics to identify patients at risk of having OSA." - Harrison's Principles of Internal Medicine 22e
3. Diagnostic Testing - AASM Decision Framework
The decision tree below (from Fishman's Pulmonary) reflects AASM guidance:
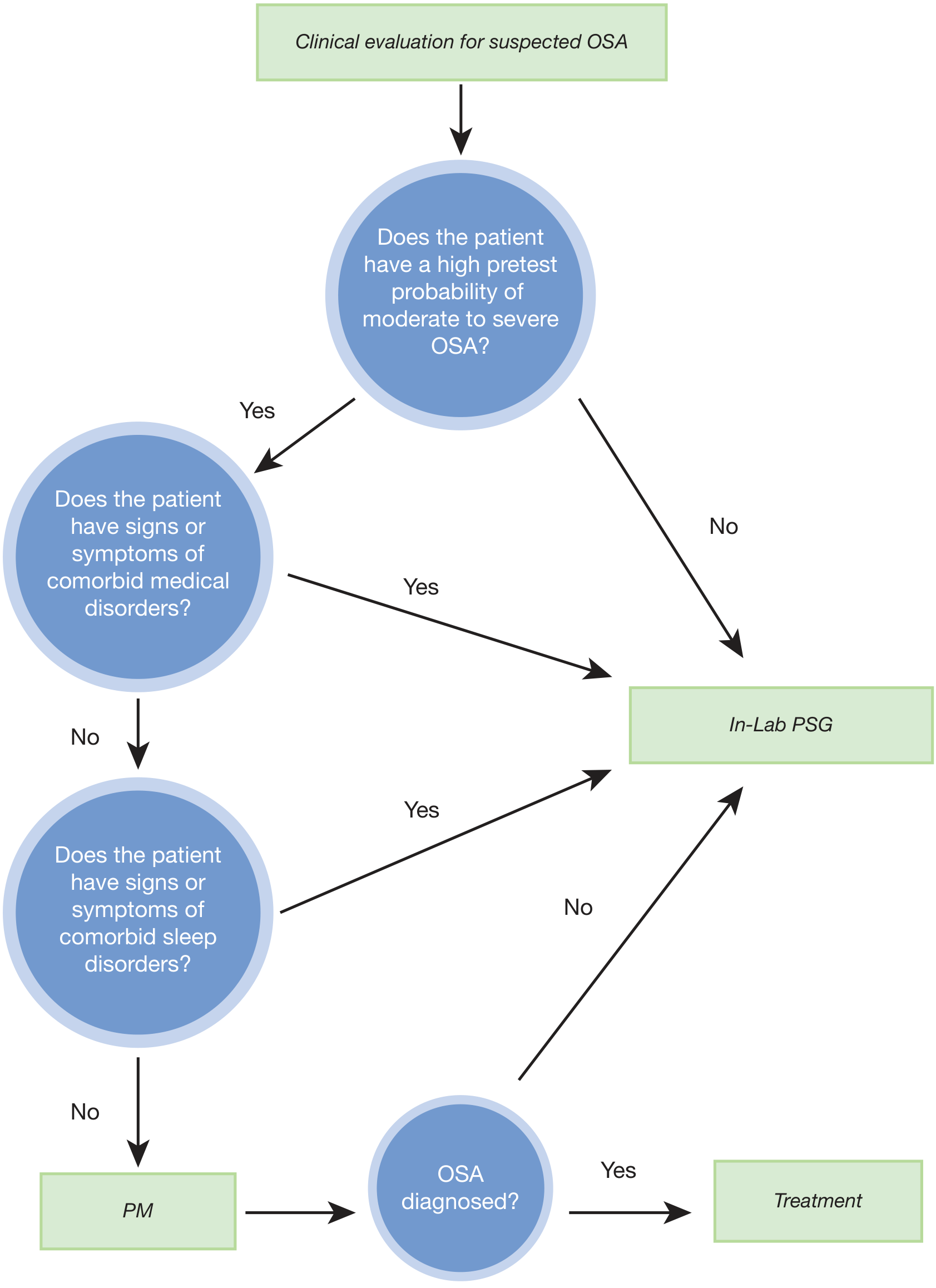
Figure: Clinical evaluation for suspected OSA - deciding between in-lab PSG and portable monitoring (HSAT). Source: Fishman's Pulmonary Diseases and Disorders
Two Diagnostic Pathways
A. Polysomnography (PSG) - Gold Standard
PSG is Type I testing, conducted in a sleep laboratory with a technician present. Parameters recorded:
- EEG (sleep staging)
- EOG (eye movements)
- Chin and limb EMG (muscle activity, arousals)
- Nasal pressure transducer + oronasal thermistor (airflow)
- Thoracoabdominal bands (respiratory effort)
- SpO2 (pulse oximetry)
- ECG
- Body position + video
PSG is strongly indicated (AASM) for:
- Suspected OSA with significant cardiorespiratory disease (CHF, COPD, pulmonary hypertension)
- Potential respiratory muscle weakness (neuromuscular disease)
- Awake hypoventilation or suspected sleep-related hypoventilation/hypoxemia
- Chronic opioid medication use
- History of stroke
- Severe insomnia complicating the study
- Prior negative or inconclusive HSAT
- Suspected comorbid sleep disorders (narcolepsy, REM behavior disorder, periodic limb movement disorder)
- Pre-surgical evaluation for upper airway surgery or oral appliance therapy
(Goldman-Cecil Medicine, Table 374-2)
B. Home Sleep Apnea Testing (HSAT) / Out-of-Center Sleep Testing (OCST)
AASM Strong Recommendation: PSG or HSAT with a technically adequate device should be used for diagnosis in uncomplicated adult patients with clinical signs indicating increased risk of moderate-to-severe OSA.
HSAT Device Classification:
| Type | Channels | Notes |
|---|---|---|
| Type I | Full PSG (EEG, EOG, EMG, ECG, airflow, effort, SpO2) | In-lab only |
| Type II | ≥7 channels including EEG, EOG, EMG, ECG, airflow, effort, SpO2 | Portable full PSG |
| Type III | ≥4 channels: ECG/HR, SpO2, ≥2 respiratory channels | Standard HSAT |
| Type IV | Airflow ± SpO2 (CMS requires ≥3 channels, 1 = airflow) | Screening only |
HSAT Advantages: Greater convenience, lower cost, replicates home sleep environment; non-inferior outcomes and PAP adherence vs PSG in uncomplicated patients (Kuna et al.)
When HSAT is NOT appropriate (proceed to PSG):
- Comorbid cardiorespiratory disease
- Suspected hypoventilation
- Neuromuscular disease
- Stroke history
- Severe insomnia
- Suspicion of other sleep disorders
- Single HSAT is negative, inconclusive, or technically inadequate
"When a single HSAT is negative, inconclusive, or technically inadequate, polysomnography should be performed for the diagnosis of OSA." - AASM 2017 (Strong Recommendation)
4. Diagnostic Criteria and Severity Classification
Diagnostic Criteria (AASM/ICSD-3)
OSA is diagnosed when:
| Scenario | AHI Threshold | Symptom Requirement |
|---|---|---|
| Uncomplicated | AHI ≥5/hr | Must have ≥1 symptom: daytime sleepiness, unrefreshing sleep, fatigue, insomnia, witnessed apneas, or co-morbidity (HTN, AF, CHF, stroke, T2DM) |
| Asymptomatic | AHI ≥15/hr | None required |
Events counted:
- Apnea: Cessation of airflow ≥10 seconds
- Hypopnea (AASM recommended): ≥30% reduction in airflow for ≥10 seconds + ≥3% SpO2 desaturation or cortical arousal
- RERA (Respiratory Effort Related Arousal): flow limitation with arousal but not meeting apnea/hypopnea criteria - counted in the RDI but not AHI
Note: CMS/Medicare uses a 4% desaturation criterion for hypopneas (more restrictive), while AASM recommends 3%.
Severity Classification
| Severity | AHI (events/hour) |
|---|---|
| Mild | 5 - 14 |
| Moderate | 15 - 29 |
| Severe | ≥30 |
(Miller's Anesthesia, p. 8339; Fuster & Hurst's The Heart)
Treatment is recommended for all patients with moderate-to-severe disease; mild OSA is treated based on symptoms and clinical context.
5. Inpatient Screening - 2025 AASM Update
The 2025 AASM Clinical Practice Guideline (Mehra et al., JCSM 2025) [PMID: 40838698] specifically addresses hospitalized patients - the first AASM guideline for this setting:
- Conditional Recommendation: For medically hospitalized adults at increased risk for OSA, in-hospital screening as part of an evaluation and management pathway incorporating diagnosis + PAP treatment is suggested (rather than no screening).
- Screening modalities: validated questionnaires (STOP-BANG) and/or overnight high-resolution pulse oximetry
- Patients with established OSA diagnosis on active treatment should continue their treatment in hospital unless contraindicated
- A discharge management plan for timely outpatient diagnosis/follow-up is recommended for newly identified cases
6. Nocturnal Oximetry as a Supplemental Tool
Overnight oximetry showing a "sawtooth pattern" of recurrent desaturations is highly suggestive of OSA but is not sufficient alone for diagnosis. It may be used as:
- Part of an inpatient screening pathway
- A triage tool to prioritize who needs formal sleep testing
- Monitoring tool post-treatment
Summary Algorithm
Clinical suspicion of OSA
↓
Screening (history + ESS + STOP-BANG + physical exam)
↓
High pretest probability of moderate-to-severe OSA?
YES ↓ NO ↓
Comorbid medical/sleep disorder? Proceed to HSAT
YES → In-lab PSG
NO → HSAT
↓
HSAT negative/inconclusive?
YES → In-lab PSG
NO → AHI ≥5 + symptoms OR AHI ≥15 → DIAGNOSIS
↓
Severity: Mild (5-14) / Moderate (15-29) / Severe (≥30)
↓
Treatment
Key Sources:
- AASM 2017 Clinical Practice Guideline for Diagnostic Testing for Adult OSA (Kapur et al., J Clin Sleep Med 2017;13:479-504) - endorsed by World Sleep Society 2021
- AASM 2025 Inpatient OSA Guideline: Mehra et al., J Clin Sleep Med 2025 [PMID: 40838698]
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Goldman-Cecil Medicine, Table 374-2
- Miller's Anesthesia, 10e
- Harrison's Principles of Internal Medicine 22e (2025)
- Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.