Abg analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, structured guide to ABG (Arterial Blood Gas) analysis.
Arterial Blood Gas (ABG) Analysis
Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| PaO2 | 70 - 95 mmHg (age-dependent) |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
Age correction for PaO2 (sitting): PaO2 = 104.2 - (0.27 × age in years) Age correction for A-a gradient: P(A-a)O2 = (age/4) + 4
Step-by-Step Interpretation
Step 1: Assess pH
- < 7.35 = Acidemia
- > 7.45 = Alkalemia
- 7.35-7.45 = Normal (but may still have a mixed disorder)
Step 2: Identify the Primary Disorder
Look at PaCO2 and HCO3-:
| Disorder | pH | PaCO2 | HCO3- |
|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ | ↑ (compensatory) |
| Respiratory Alkalosis | ↑ | ↓ | ↓ (compensatory) |
| Metabolic Acidosis | ↓ | ↓ (compensatory) | ↓ |
| Metabolic Alkalosis | ↑ | ↑ (compensatory) | ↑ |
Key rule: The compensation is always in the same direction as the primary disturbance. For example, in metabolic acidosis (↓HCO3-), the respiratory compensation is hyperventilation (↓PaCO2).
Step 3: Check for Adequate Compensation
Use these formulas to determine if compensation is appropriate:
| Primary Disorder | Expected Compensation Formula |
|---|---|
| Metabolic Acidosis | Expected PaCO2 = (1.5 × HCO3-) + 8 ± 2 (Winter's formula) |
| Metabolic Alkalosis | Expected PaCO2 = (0.7 × HCO3-) + 21 ± 2 |
| Acute Respiratory Acidosis | HCO3- rises 1 mEq/L per 10 mmHg rise in PaCO2 |
| Chronic Respiratory Acidosis | HCO3- rises 3.5 mEq/L per 10 mmHg rise in PaCO2 |
| Acute Respiratory Alkalosis | HCO3- falls 2 mEq/L per 10 mmHg fall in PaCO2 |
| Chronic Respiratory Alkalosis | HCO3- falls 5 mEq/L per 10 mmHg fall in PaCO2 |
If measured PaCO2 is above the Winter's formula result in metabolic acidosis, there is a superimposed respiratory acidosis.
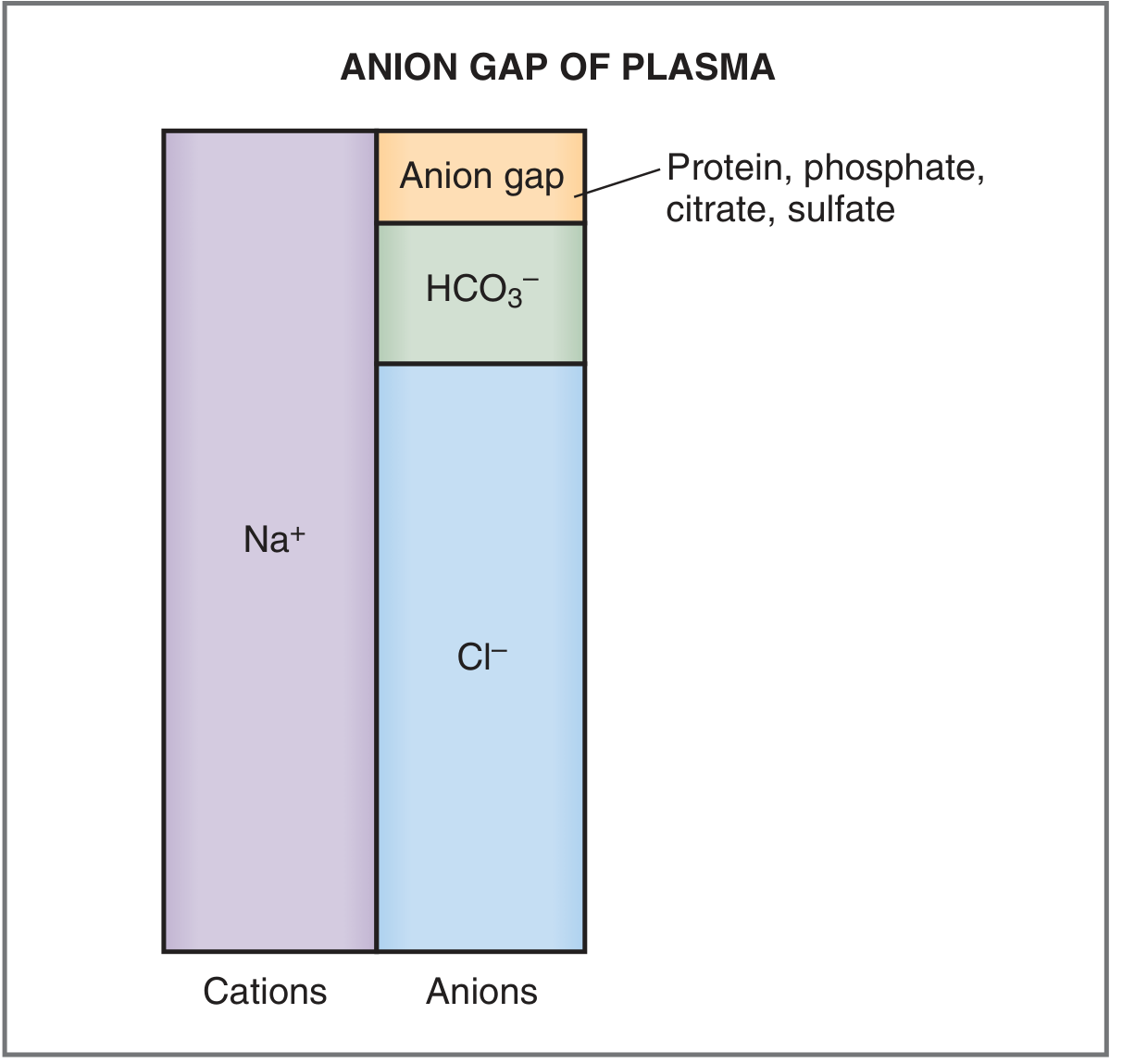
Step 4: Calculate the Anion Gap (in Metabolic Acidosis)
Anion Gap (AG) = [Na+] - ([HCO3-] + [Cl-])
Normal AG = 8-16 mEq/L (typically cited as ~12 mEq/L)
High Anion Gap Metabolic Acidosis (HAGMA)
Mnemonic: MUDPILES or GOLDMARK
| Cause | Key Feature |
|---|---|
| Diabetic ketoacidosis | Ketones in urine/blood |
| Lactic acidosis | Lactate > 2 mmol/L |
| Salicylate poisoning | History, tinnitus |
| Methanol poisoning | Osmolar gap present |
| Ethylene glycol poisoning | Osmolar gap + oxalate crystals |
| Chronic renal failure | Phosphate/sulfate retention |
Normal Anion Gap Metabolic Acidosis (NAGMA) = Hyperchloremic
Common causes: Diarrhea, Renal Tubular Acidosis (RTA)
- In NAGMA, HCO3- loss is replaced by Cl- (measured anion), so the gap stays normal.
Step 5: Assess Oxygenation
Alveolar-arterial (A-a) gradient:
P(A-a)O2 = FiO2 × (PB - PH2O) - (PaO2 + PaCO2/0.8)
At room air (FiO2 = 0.21, sea level): simplified to roughly
P(A-a)O2 = 150 - PaO2 - (PaCO2/0.8)
Mechanisms of Hypoxemia
| Mechanism | A-a Gradient | Example |
|---|---|---|
| V/Q mismatch | Increased | Pneumonia, PE |
| Diffusion impairment | Increased | Interstitial lung disease |
| Right-to-left shunt | Increased | AVM, intracardiac shunt |
| Hypoventilation | Normal | Neuromuscular weakness, opioid overdose |
| Low inspired O2 (altitude) | Normal | High altitude |
| Hepatopulmonary syndrome | Increased | Liver cirrhosis |
Henderson-Hasselbalch Equation
pH = 6.1 + log10 ([HCO3-] / 0.003 × PaCO2)
This shows that pH is determined by the ratio of HCO3- to CO2, not by the absolute values alone.
Venous Blood Gas (VBG) vs ABG
VBGs are increasingly used as a safer alternative, but with limitations:
- Venous pH averages ~0.03 lower than arterial pH (good correlation)
- PvCO2 averages 3-8 mmHg higher than PaCO2 (less reliable correlation)
- VBGs are unreliable in: hypotensive patients, severe hypercapnia
- A normal PvCO2 can be used to rule out hypercapnia
Common Mixed Disorders
A mixed disorder exists when the measured compensation falls outside the expected range, OR when two primary disturbances coexist.
Examples:
- Respiratory acidosis + Metabolic alkalosis: COPD patient on chronic diuretics
- Metabolic acidosis + Respiratory alkalosis: Sepsis (lactic acidosis + hyperventilation)
- Metabolic acidosis + Metabolic alkalosis: DKA patient with protracted vomiting
Quick Summary Table
| Disorder | pH | Primary Change | Compensation |
|---|---|---|---|
| Metabolic Acidosis | ↓ | ↓ HCO3- | Hyperventilation (↓ PaCO2) |
| Metabolic Alkalosis | ↑ | ↑ HCO3- | Hypoventilation (↑ PaCO2) |
| Respiratory Acidosis | ↓ | ↑ PaCO2 | Renal ↑ HCO3- retention |
| Respiratory Alkalosis | ↑ | ↓ PaCO2 | Renal ↑ HCO3- excretion |
Sources: Goldman-Cecil Medicine (Table 89-1, ABG & A-a gradient), Costanzo Physiology 7th Ed. (Acid-Base Disorders, p. 330-332)
This is a shared conversation. Sign in to Orris to start your own chat.