swine flu
Reading File
Finding Sources
Searching PubMed
"swine flu" OR "H1N1 influenza" AND pandemic
Searching the Web
swine flu H1N1 influenza overview symptoms treatment 2024
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK513241
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of swine flu (H1N1 influenza):
Swine Flu (H1N1 Influenza A)
What Is It?
Swine flu is caused by an influenza A virus of the H1N1 subtype. The term "swine flu" most commonly refers to the 2009 pandemic strain - formally designated A/California/04/2009 (H1N1)pdm09 - which was a novel reassortant virus that had never circulated in humans before. Pigs are called "mixing vessels" because they are susceptible to both avian and human influenza strains, allowing viral reassortment to generate new subtypes.
Origins and Emergence
The 2009 pandemic H1N1 virus arose from an extraordinarily complex reassortment of genomic segments from four distinct influenza lineages: North American swine influenza, North American avian influenza, human influenza (H3N2), and Eurasian swine influenza H1N1/H3N2. This produced a "triple-triple reassortant" - a virus with a completely new antigenic profile against which most people under 60 had no prior immunity.
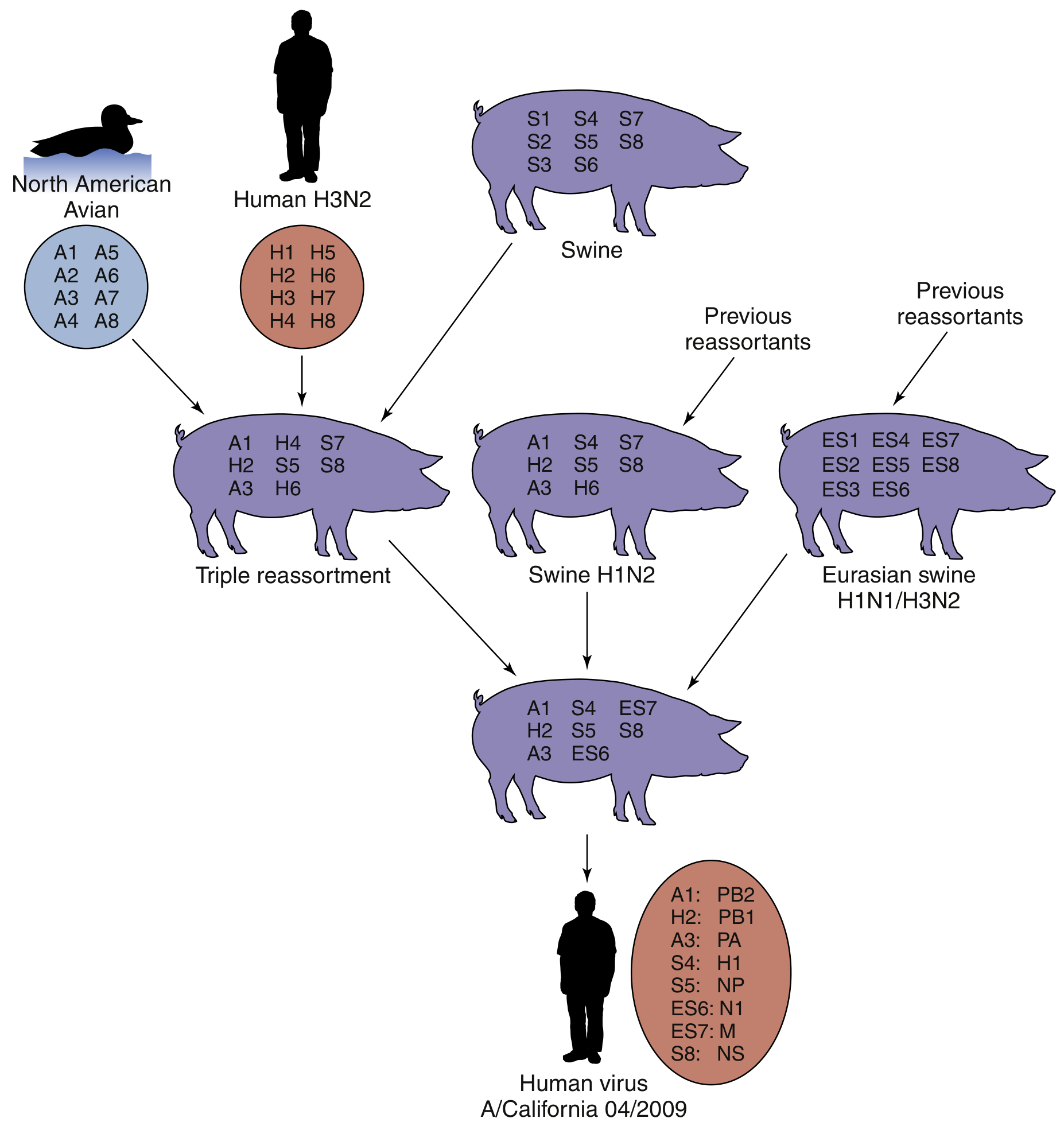
Fig. 49.5 - Generation of A/California/04/2009 (H1N1) by multiple reassortments. The pandemic H1N1 virus emerged in spring 2009 (out of season) in Mexico, first identified in California. - Medical Microbiology 9e, p. 556
- First detected in April 2009 in southern California in two children
- Quickly spread globally - the WHO declared it the first pandemic of the 21st century
- Pandemic declared over in August 2010; since then H1N1pdm09 has circulated as a seasonal influenza strain
Why H1N1 Is Uniquely Dangerous
Unlike H5N1 (avian flu), the 2009 H1N1 binds to sialic acid α2,6 galactose receptors found throughout the upper respiratory tract, making human-to-human transmission highly efficient. It also binds α2,3 galactose receptors in the lower lungs, explaining why it can cause severe lower respiratory disease. This dual receptor binding is a key reason why it spread so easily but also caused more severe illness than typical seasonal flu in some patients. - Sherris & Ryan's Medical Microbiology, 8th ed.
Transmission
- Spread by respiratory droplets (talking, coughing, sneezing) and potentially airborne
- Infectious from about 1 day before symptom onset to 7 days after
- Can survive on surfaces (e.g., countertops) for up to 1 day
- Contagion is prolonged especially in children
At-Risk Groups
| High-Risk Group | Reason |
|---|---|
| Pregnant women | Immunologic changes, impaired respiratory reserve |
| Children < 5 years | Naive immunity |
| Adults > 65 years | Multiple comorbidities (though 2009 strain spared elderly more than usual due to cross-reactive antibodies from prior H1N1 exposure) |
| Immunocompromised | Reduced viral clearance |
| Chronic cardiopulmonary disease | Less reserve |
| Healthy young adults (uniquely in 2009) | Lack of prior immunity to new strain |
Note: In the 2009 pandemic, >90% of mortalities were in the under-65 age group - the reverse of typical seasonal flu - because elderly people had cross-reactive antibodies from earlier H1N1 exposure before 1957.
Symptoms
Signs and symptoms closely resemble seasonal influenza but with some differences:
- Fever, chills, rigors
- Cough (more prominent than in seasonal flu)
- Sore throat, rhinorrhea, nasal congestion
- Myalgias/muscle pain (more prominent)
- Headache
- Fatigue, loss of appetite
- Conjunctivitis
- Gastrointestinal symptoms (nausea, vomiting, diarrhea) - more common than in seasonal flu
- Dyspnea in severe cases
In severe cases: viral pneumonia, ARDS, secondary bacterial sepsis, multi-organ failure.
Diagnosis
- Clinical diagnosis is possible during a known outbreak
- Confirmation requires respiratory specimens (nasopharyngeal swabs/aspirates)
- Real-time RT-PCR is the gold standard for subtyping
- Rapid influenza diagnostic tests (RIDTs) exist but have lower sensitivity for H1N1
Treatment
Antivirals:
- Oseltamivir (Tamiflu) and zanamivir - neuraminidase inhibitors; most effective when started within 72 hours of symptom onset; can reduce severity and mortality
- The 2009 pandemic strain was resistant to amantadine and rimantadine (M2 ion channel inhibitors) from the outset
- Peramivir (IV) for hospitalized patients who cannot tolerate oral/inhaled antivirals
Who to treat:
- Hospitalized patients
- High-risk patients (above groups)
- Severe or progressive illness
- Healthy outpatients with uncomplicated mild illness generally do not require antivirals
Supportive care: Hydration, antipyretics (avoid aspirin in children - Reye's syndrome risk), oxygen, mechanical ventilation for respiratory failure, ECMO in refractory ARDS.
Prevention
- Annual influenza vaccination - The H1N1pdm09 strain has been included in seasonal flu vaccines since 2010 (both trivalent and quadrivalent formulations)
- Hand hygiene - soap and water or alcohol-based sanitizers
- Respiratory etiquette - cover coughs/sneezes
- Avoiding close contact with sick individuals
- Swine-to-human transmission prevention - limiting direct contact with infected pigs; vaccination of swine herds
Historical Context
| Year | Event |
|---|---|
| 1918 | "Spanish flu" (H1N1) - ~50 million deaths, infected 500 million worldwide |
| 1977 | H1N1 "Russian flu" reappeared |
| April 2009 | Novel H1N1 detected in California |
| June 2009 | WHO declared pandemic (Phase 6) |
| August 2010 | Pandemic declared over; H1N1pdm09 became endemic/seasonal |
Current Status (2026)
The H1N1pdm09 strain now circulates as a seasonal influenza A virus alongside H3N2 and influenza B strains. Annual flu vaccines are updated to match circulating strains. Antiviral resistance (notably oseltamivir-resistant H1N1 with the H275Y mutation) is monitored globally by WHO surveillance networks.
Sources:
- Medical Microbiology 9e (Murray et al.), Ch. 49
- Sherris & Ryan's Medical Microbiology, 8th ed., Ch. 9
- StatPearls - H1N1 Influenza
This is a shared conversation. Sign in to Orris to start your own chat.