Abg analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks to deliver a thorough ABG analysis guide. Let me compile this.
Arterial Blood Gas (ABG) Analysis
Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| PaO2 | 70 - 95 mmHg (age-dependent) |
| HCO3- | 22 - 26 mEq/L |
| Base Excess | -2 to +2 mEq/L |
| SpO2 | 95 - 100% |
PaO2 sitting = 104.2 - (0.27 × age in years) - Goldman-Cecil Medicine
Stepwise Approach to ABG Interpretation
(Barash Clinical Anesthesia, 9e)
Step 1 - Determine Acid-Base Status (pH)
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
- pH 7.35-7.45 = Normal (but a mixed disorder may still be present!)
Step 2 - Identify the Primary Disorder
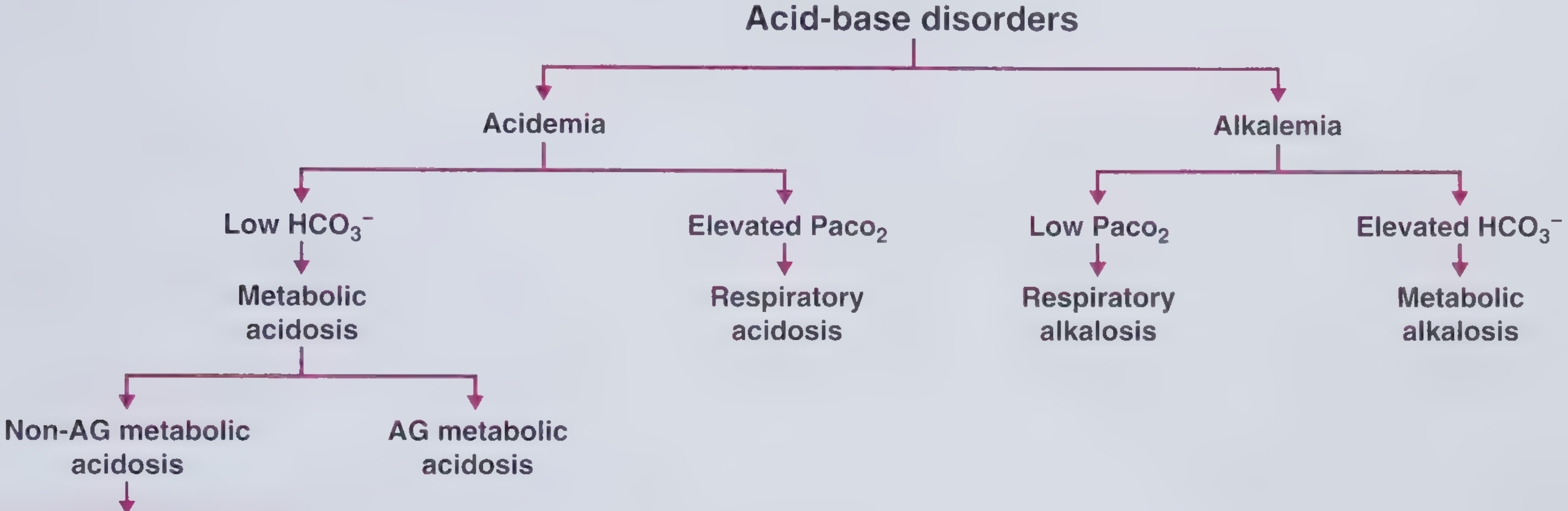
| pH | PaCO2 | HCO3- | Diagnosis |
|---|---|---|---|
| ↓ | ↑ | - | Respiratory Acidosis |
| ↓ | - | ↓ | Metabolic Acidosis |
| ↑ | ↓ | - | Respiratory Alkalosis |
| ↑ | - | ↑ | Metabolic Alkalosis |
Step 3 - Assess Compensation
The body never overcompensates. If pH normalizes completely, a mixed disorder is likely.
Compensation Formulas:
| Primary Disorder | Expected Compensation | Formula |
|---|---|---|
| Metabolic Acidosis | ↓ PaCO2 | PaCO2 = (1.5 × HCO3-) + 8 ± 2 (Winter's formula) |
| Metabolic Alkalosis | ↑ PaCO2 | PaCO2 = 40 + 0.7 × (HCO3- - 24) ± 2 |
| Acute Respiratory Acidosis | ↑ HCO3- | HCO3- rises 1 mEq/L per 10 mmHg ↑ CO2 |
| Chronic Respiratory Acidosis | ↑ HCO3- | HCO3- rises 3.5 mEq/L per 10 mmHg ↑ CO2 |
| Acute Respiratory Alkalosis | ↓ HCO3- | HCO3- falls 2 mEq/L per 10 mmHg ↓ CO2 |
| Chronic Respiratory Alkalosis | ↓ HCO3- | HCO3- falls 5 mEq/L per 10 mmHg ↓ CO2 |
Maximum respiratory compensation: PaCO2 cannot fall below ~12 mmHg. - Tintinalli's Emergency Medicine
Metabolic alkalosis compensation is least effective because hypoventilation causes hypoxemia - PaCO2 rarely exceeds 60 mmHg even in severe alkalosis. - Henry's Clinical Diagnosis
Step 4 - Calculate Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-) Normal: < 12-13 mEq/L
- Correct for low albumin: Add 2.5 mEq/L to AG for every 1 g/dL decrease in albumin below 4 g/dL.
High AG Metabolic Acidosis - Causes (MUDPILES / KUSMALE):
| Category | Examples |
|---|---|
| Renal failure (Uremia) | Chronic kidney disease |
| Ketoacidosis | DKA, alcoholic ketoacidosis, starvation |
| Lactic acidosis | Sepsis, shock, metformin toxicity |
| Ingestions/Toxins | Methanol, ethylene glycol, salicylates |
Non-Anion Gap (Hyperchloremic) Metabolic Acidosis - Causes:
- Diarrhea (GI HCO3- loss)
- Renal tubular acidosis (RTA) types 1, 2, 4
- Dilution from IV fluids
- Carbonic anhydrase inhibitors (acetazolamide)
- Ureteral diversion
- Post-hypocapnia
Step 5 - Urine Anion Gap (for non-AG acidosis)
Urine AG = Urine (Na+ + K+ - Cl-)
- Positive (+) = impaired renal acid excretion → RTA
- Negative (-) = GI HCO3- loss (e.g., diarrhea)
Step 6 - Delta-Delta Ratio (ΔΔ) for Mixed Disorders
ΔΔ = ΔAG / ΔHCO3- = (patient AG - 12) / (24 - patient HCO3-)
| ΔΔ Value | Interpretation |
|---|---|
| < 1.0 | Mixed AG + Non-AG metabolic acidosis |
| 1.0 - 2.0 | Pure AG metabolic acidosis |
| > 2.0 | AG metabolic acidosis + metabolic alkalosis (or chronic respiratory acidosis) |
Assessing Oxygenation
Alveolar-Arterial (A-a) Gradient
P(A-a)O2 = [FiO2 × (PB - 47)] - [PaO2 + PaCO2/0.8]
Normal: (Age/4) + 4 (increases with age)
| P(A-a) Gradient | Causes |
|---|---|
| Normal | Hypoventilation, high altitude/low FiO2 |
| Elevated | V/Q mismatch (pneumonia, PE), diffusion impairment (ILD), right-to-left shunt, hepatopulmonary syndrome |
Mechanisms of Hypoxemia
| Mechanism | Example | A-a Gradient |
|---|---|---|
| V/Q mismatch | Pneumonia, COPD | Elevated |
| Diffusion impairment | ILD, emphysema | Elevated |
| R-to-L shunt | AVM, intracardiac shunt | Elevated |
| Hypoventilation | CNS depression, NMJ disease | Normal |
| Low FiO2 | High altitude | Normal |
| Hepatopulmonary syndrome | Cirrhosis | Elevated |
(Goldman-Cecil Medicine)
Venous Blood Gas (VBG) vs. ABG
| Parameter | VBG vs ABG |
|---|---|
| pH | Venous ~0.03-0.05 lower |
| PCO2 | Venous 3-8 mmHg higher |
| PO2 | NOT interchangeable - VBG cannot assess oxygenation |
| Lactate | Correlates well except in mildly elevated range |
VBGs are unacceptable substitutes in hypotensive patients or severe hypercapnia. - Tintinalli's Emergency Medicine
Quick Memory Aid
ROME:
Respiratory - Opposite (pH↓, CO2↑ OR pH↑, CO2↓)
Metabolic - Equal (pH↓, HCO3-↓ OR pH↑, HCO3-↑)
Mixed Acid-Base Disorders - Key Tip
A normal pH with a clearly abnormal PaCO2 and HCO3- should always trigger suspicion for a mixed disorder. Also, an elevated AG with otherwise normal values suggests a concurrent high-AG acidosis + metabolic alkalosis canceling each other out. - Tintinalli's Emergency Medicine
Sources: Goldman-Cecil Medicine | Barash Clinical Anesthesia 9e | Tintinalli's Emergency Medicine | Frameworks for Internal Medicine | Henry's Clinical Diagnosis and Management | Ganong's Review of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.