Explain each and everything about the histology of organs associated with the digestive tract that consists of the following topics: Salivary glands Pancreas Liver Gall bladder Along with clinical applications/ correlates
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the key content and histological images. Let me compile the comprehensive answer.
Histology of Organs Associated with the Digestive Tract
Sources: Junqueira's Basic Histology (17e) and Wheater's Functional Histology / Ross's Histology
Overview
The digestive system consists of the alimentary canal and its principal associated organs: the salivary glands, pancreas, liver, and gallbladder. These accessory organs are not part of the canal wall itself but pour their secretions into it and are essential for digestion and absorption.
1. SALIVARY GLANDS
General Organization
Exocrine glands in the oral mucosa produce saliva, which serves digestive, lubricating, and protective (immunologic) functions. There are three pairs of major salivary glands - parotid, submandibular, and sublingual - plus numerous minor salivary glands scattered throughout the oral mucosa. Major glands produce ~90% of saliva (0.75-1.50 L/day); minor glands the remaining 10%.
Each major gland is surrounded by a dense irregular connective tissue capsule from which septa extend inward, dividing the parenchyma into lobes and lobules. The septa carry larger blood vessels and excretory ducts. The secretory units (acini) are organized into lobules.
Cell Types of Secretory Acini
1. Serous Cells
- Pyramidal protein-secreting cells
- Round, basally placed nuclei
- Well-developed basal RER (strongly basophilic cytoplasm)
- Apical secretory (zymogen) granules (eosinophilic/purple)
- Joined apically by tight and adherent junctions
- Arranged in spherical serous acini with a small central lumen
- Secrete enzymes (e.g., amylase, proline-rich proteins, lactoferrin)
2. Mucous Cells
- More columnar in shape
- Flattened, compressed basal nuclei with condensed chromatin
- Cytoplasm filled with hydrophilic mucin granules - appear pale/empty in routine H&E (because mucin washes out during processing)
- Arranged in elongated mucous tubules rather than spherical acini
- Secrete mucins (glycoproteins) for lubrication
3. Myoepithelial Cells
- Located inside the basal lamina surrounding acini and proximal ducts
- Flattened, stellate cells with contractile actin-containing processes
- Contract to expel secretion into and through the duct system
The Salivon (Basic Secretory Unit)
The salivon is the fundamental functional unit and consists of:
- Acinus (secretory unit)
- Intercalated duct
- Striated duct
- Excretory duct
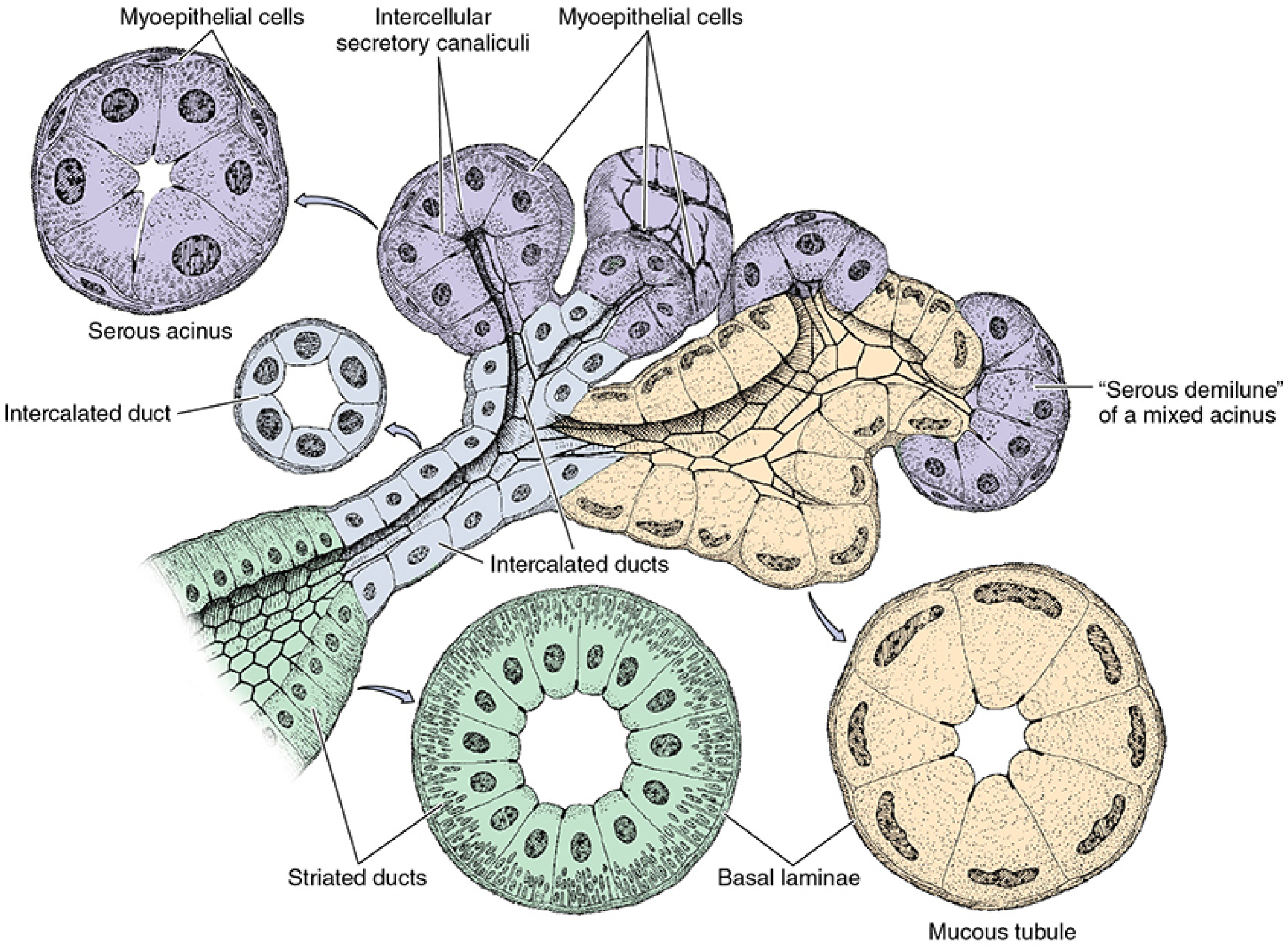
Intercalated Ducts
- Drain acini directly
- Lined by simple cuboidal epithelium
- Short, narrow, and difficult to identify in mucous glands
- Most prominent in serous glands (parotid) where they are long and narrow
- Contain occasional myoepithelial cells at their bases
- Absorb Cl⁻ from the acinar product
Striated Ducts (Intralobular)
- Lined by simple cuboidal-to-columnar epithelium
- Characteristic basal striations under light microscopy = longitudinal infoldings of the basal plasma membrane enclosing elongated mitochondria
- These folds are a morphologic adaptation for active electrolyte transport
- Function: reabsorb Na⁺ from the primary secretion; secrete K⁺ and HCO₃⁻ into the lumen
- Net result: saliva becomes hypotonic
- Diameter often exceeds that of the secretory acinus
- Most prominent in the parotid gland
Excretory Ducts (Interlobular/Interlobar)
- Travel in the interlobular connective tissue septa
- Small excretory ducts: simple cuboidal epithelium
- Progressively transition to pseudostratified columnar → stratified cuboidal → stratified columnar
- At the oral cavity opening: stratified squamous epithelium
- Parotid duct = Stensen's duct (opens opposite upper 2nd molar)
- Submandibular duct = Wharton's duct
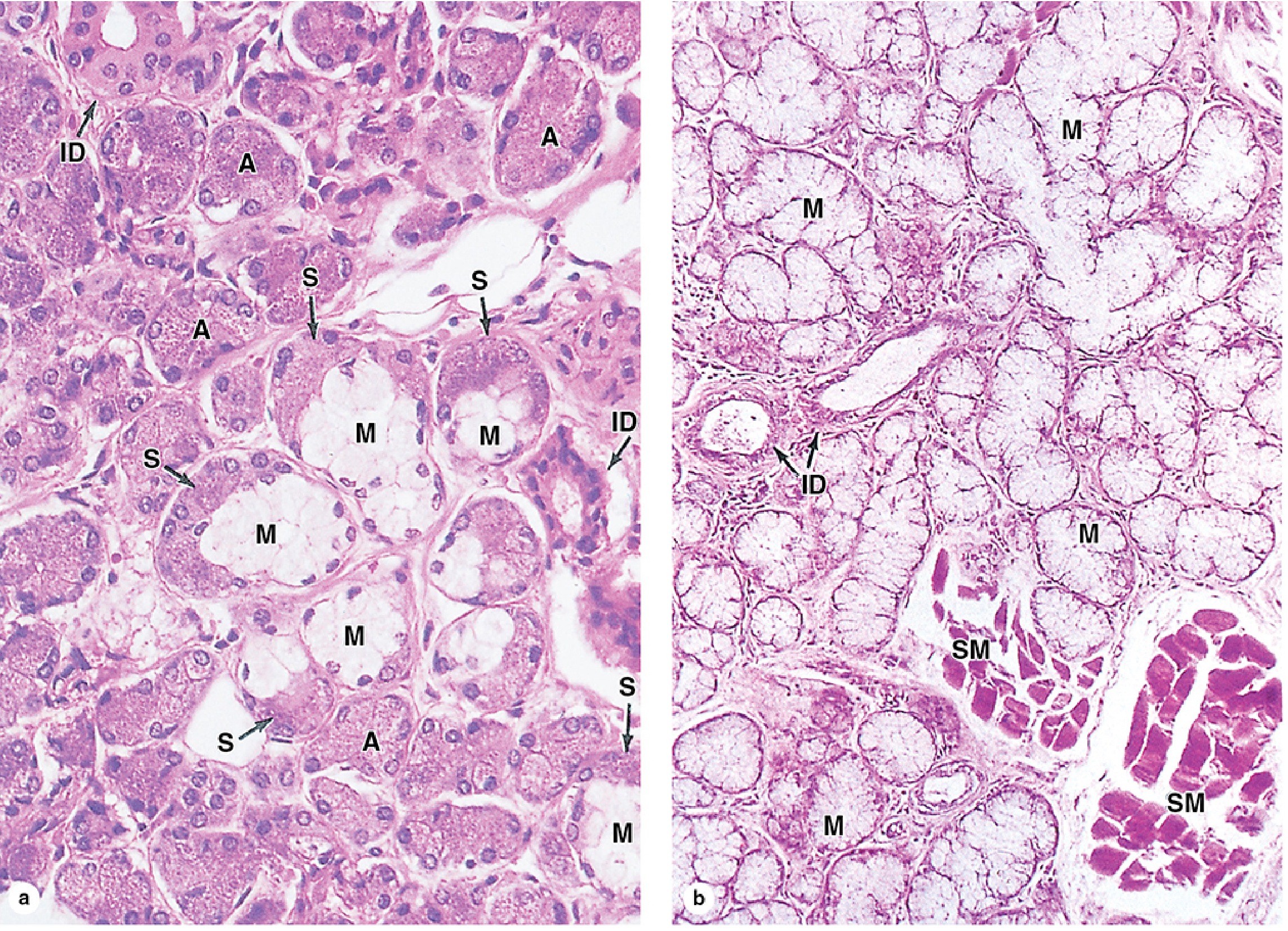
Three Types of Acini and Serous Demilunes
- Serous acini: spherical, only serous cells, small central lumen
- Mucous acini: tubular, only mucous cells
- Mixed acini: contain both - in routine H&E preparations, mucous cells swell during fixation and push serous cells to the periphery, creating crescent-shaped "serous demilunes." This is now recognized as a fixation artifact - rapid-freeze electron microscopy shows both cell types actually line the same row around the lumen.
The Three Major Salivary Glands
| Feature | Parotid | Submandibular | Sublingual |
|---|---|---|---|
| Secretion type | Pure serous | Mixed (predominantly serous) | Mixed (predominantly mucous) |
| Acini | Only serous | Serous + some mucous | Mostly mucous tubules with serous demilunes |
| Intercalated ducts | Long, prominent | Shorter | Sparse/short |
| Striated ducts | Large, conspicuous | Present | Short, inconspicuous |
| Adipose tissue | Scattered fat cells throughout (increases with age) | None | None |
| Duct | Stensen's duct (Parotid duct) | Wharton's duct | Multiple short ducts of Rivinus |
| Location | Below/anterior to ear, between mandibular ramus and temporal styloid | Floor of mouth, submandibular triangle | Floor of mouth, anterior to submandibular |
Saliva: Composition and Function
Saliva contains:
- Water (99%)
- Enzymes: salivary amylase (ptyalin), lingual lipase
- Antibacterial proteins: lactoferrin, lysozyme, peroxidase
- Immunoglobulins: secretory IgA (produced by plasma cells in lamina propria, transported through ductal epithelium)
- Mucins: for lubrication
- Electrolytes: Na⁺, K⁺, Cl⁻, HCO₃⁻ (hypotonic relative to plasma)
- Buffering capacity: helps maintain near-neutral pH in the oral cavity
Clinical Correlates: Salivary Glands
Xerostomia (Dry Mouth)
Inadequate saliva production. Causes include:
- Mumps (parotitis): paramyxovirus infects parotid gland; bilateral parotid swelling
- Radiation therapy: destruction of acinar cells (particularly serous) from head/neck radiation
- Sjögren syndrome: autoimmune lymphocytic infiltration destroys acinar and ductal cells; bilateral parotid/lacrimal gland enlargement, dry mouth and dry eyes (keratoconjunctivitis sicca)
- Drugs: anticholinergics, antihistamines, tricyclic antidepressants
Sialorrhea (Excessive Salivation)
Associated with autonomic activity of nausea, oral cavity inflammation, and rabies viral infection.
Salivary Gland Tumors
- Most common = pleomorphic adenoma (benign mixed tumor) - most frequent in the parotid gland; shows both epithelial and myxochondroid stromal components; locally recurrent if not completely excised
- Warthin tumor (papillary cystadenoma lymphomatosum): benign, almost exclusively parotid, bilateral in 10%; consists of cystic spaces lined by double-layered oncocytic epithelium within a lymphoid stroma
- Mucoepidermoid carcinoma: most common malignant salivary tumor
- Adenoid cystic carcinoma: characterized by perineural invasion; cribriform ("Swiss cheese") pattern on histology
Salivary Gland Aplasia
Disruption in epithelial-mesenchymal signaling or autonomic innervation leads to aplasia or hypoplasia; associated with cleft palate, skeletal dysplasias, branchial cleft anomalies.
2. PANCREAS
General Organization
The pancreas is a mixed exocrine-endocrine gland lying in the retroperitoneum. It has:
- Exocrine portion: ~99% of the gland; secretes digestive enzymes into the duodenum
- Endocrine portion: ~1%; the islets of Langerhans, secreting hormones into the blood
The gland is covered by a thin capsule of loose connective tissue (not a dense capsule like the parotid). Septa extend inward, dividing it into lobules, but the connective tissue is sparse relative to the parotid - this is a key distinguishing feature. Ducts and blood vessels travel in these septa.
Exocrine Pancreas
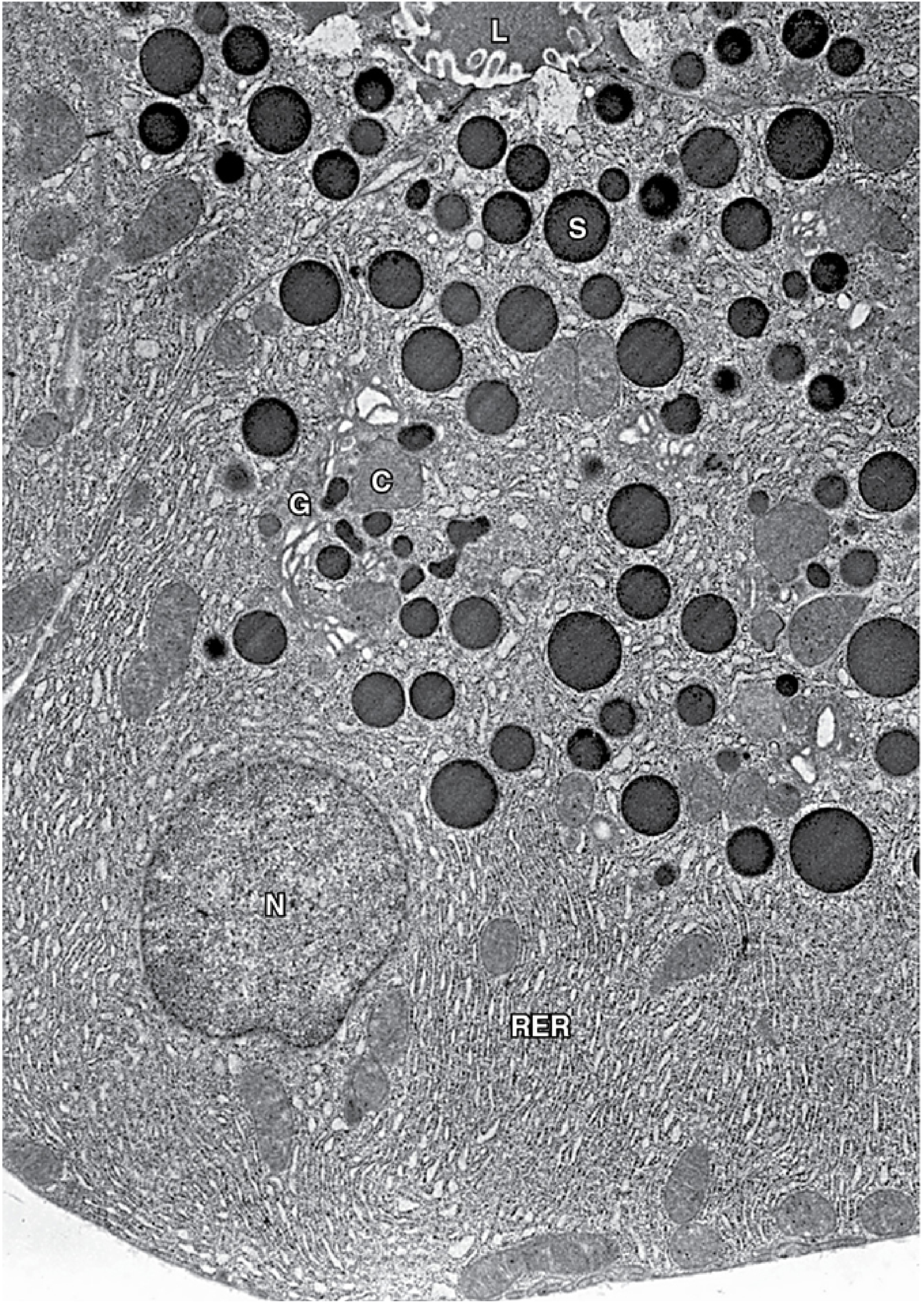
Acinar Cells
The exocrine pancreas consists of serous acini - identical in principle to parotid acini but with important distinctions:
- Pyramidal cells with round basal nuclei
- Strongly basophilic basal cytoplasm (abundant RER) - basophilia is most intense at the base
- Numerous apical zymogen granules (eosinophilic, acidophilic) containing inactive enzyme precursors (zymogens)
- Arranged around a very small central lumen
- No myoepithelial cells (unlike salivary glands)
- Secretes a wide array of enzymes:
- Proteases (trypsinogen, chymotrypsinogen, proelastase, procarboxypeptidase) - secreted as zymogens activated in the duodenum by enterokinase
- Lipase, colipase, phospholipase A2
- Amylase (active as secreted)
- Ribonuclease, deoxyribonuclease
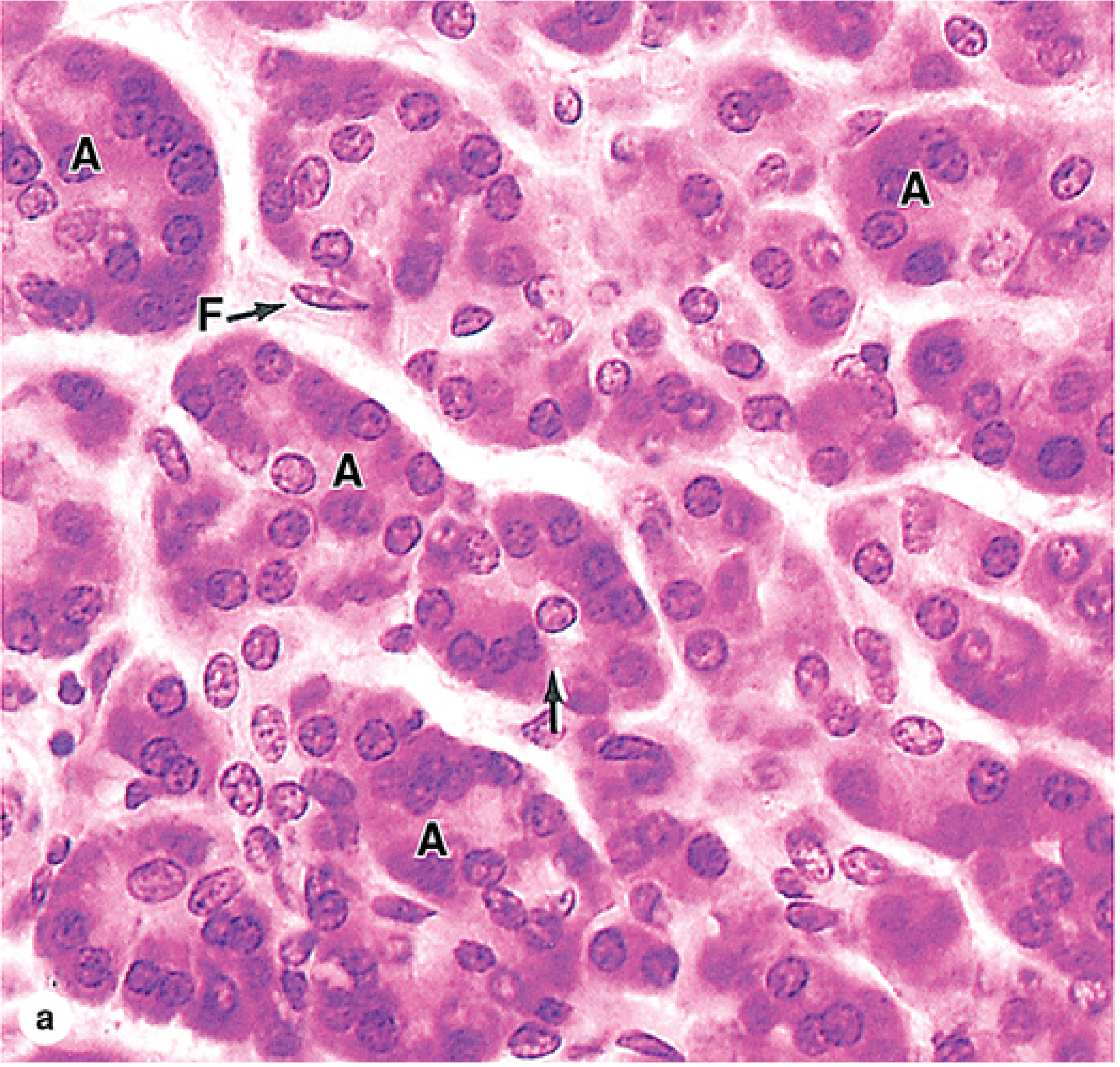
Centroacinar Cells
- Unique to the pancreas - not found in salivary glands
- Small, pale, flattened cells that represent the initial cells of the intercalated duct system inserted back into the lumen of the acinus
- Light-staining cytoplasm and oval/flat nuclei
- Under the influence of secretin (from S cells of duodenum), centroacinar and intercalated duct cells produce a copious HCO₃⁻-rich fluid that:
- Hydrates the enzymatic secretion
- Alkalinizes it (neutralizes gastric acid entering duodenum)
- Flushes enzymes into the duodenum
Duct System
| Duct | Epithelium |
|---|---|
| Intercalated duct | Simple cuboidal/squamous |
| Intralobular duct | Cuboidal |
| Interlobular duct | Columnar with goblet cells |
| Main pancreatic duct (of Wirsung) | Tall columnar with goblet cells |
| Accessory duct (of Santorini) | Columnar |
Key distinction from salivary glands: the pancreas has NO striated ducts. The pancreas also lacks the extensive electrolyte-modifying duct function of salivary glands; instead, duct cells produce the HCO₃⁻-rich fluid under secretin control.
Endocrine Pancreas - Islets of Langerhans
Islets are pale-staining, richly vascularized clusters of endocrine cells scattered throughout the exocrine tissue (more numerous in the tail). They are surrounded by a thin reticular fiber capsule.
Cell Types in Islets
| Cell Type | % of Islet | Location | Hormone | Function |
|---|---|---|---|---|
| B (β) cells | ~70% | Center of islet | Insulin | Lowers blood glucose; promotes glycogen synthesis, lipogenesis, protein synthesis |
| A (α) cells | ~20% | Periphery | Glucagon | Raises blood glucose; promotes glycogenolysis, gluconeogenesis |
| D (δ) cells | ~10% | Periphery | Somatostatin | Inhibits secretion of both insulin and glucagon; paracrine role |
| PP cells | <5% | Periphery | Pancreatic polypeptide | Inhibits pancreatic exocrine secretion |
| G cells | Rare | Present in fetal/neonatal | Gastrin | Normally found in stomach; present in pancreas early in development |
On routine H&E, islets appear as pale clusters compared to the darker (eosinophilic) acinar tissue. Special stains (Masson's trichrome, Gomori's aldehyde fuchsin) or immunohistochemistry distinguish individual cell types.
Regulation of Secretion
- CCK (cholecystokinin) - from I cells of duodenum/jejunum - stimulates enzyme secretion from acinar cells
- Secretin - from S cells of duodenum (triggered by acid) - stimulates HCO₃⁻-rich fluid from centroacinar/duct cells
- Autonomic (parasympathetic) fibers also stimulate secretion from both acinar and duct cells
Clinical Correlates: Pancreas
Acute Pancreatitis
- Premature activation of trypsinogen within the pancreas (rather than duodenum) leads to autodigestion
- Caused by: gallstones, alcohol, hyperlipidemia, medications, viral infections (mumps)
- Histology: acinar cell necrosis, fat necrosis, inflammatory infiltrate, hemorrhage (in severe cases)
- Clinical: severe epigastric pain, elevated serum lipase and amylase
Chronic Pancreatitis
- Repeated episodes of inflammation cause progressive replacement of acinar tissue by fibrosis (connective tissue)
- Islets may initially survive but eventually are lost
- Clinical: malabsorption (exocrine insufficiency), diabetes (endocrine insufficiency), steatorrhea
Type 1 Diabetes Mellitus
- Autoimmune insulitis: T-lymphocyte infiltration and destruction of β cells
- Remaining islets show selective loss of β cells while α, δ, and PP cells persist
- Islets may appear small and fibrosed
Type 2 Diabetes Mellitus
- Islet amyloid deposition (composed of islet amyloid polypeptide / amylin, co-secreted with insulin)
- Progressive β cell loss, with reduction in islet size and number
- Congo red staining and apple-green birefringence under polarized light
Pancreatic Adenocarcinoma
- 85% arise from ductal epithelium
- Histology: infiltrating glands with dense desmoplastic stroma
- Very aggressive; usually presents late
- Associated with KRAS mutation in >90% of cases
Insulinoma
- Most common islet cell tumor; benign in 90%
- β cell tumor producing excess insulin → hypoglycemia
- Whipple's triad: hypoglycemia symptoms, low blood glucose, relief with glucose
3. LIVER
General Organization
The liver is the largest internal organ (~1.5 kg, 2% of body weight). It is enclosed by Glisson's capsule - a thin fibrous connective tissue layer covered by visceral peritoneal mesothelium (except where the liver contacts the diaphragm). At the hilum (porta hepatis), Glisson's capsule thickens and carries the portal vein, hepatic artery, lymphatics, and bile ducts into the liver as part of the portal triad (portal canal).
Structural Models of Liver Organization
There are three overlapping conceptual models:
1. Classic Hepatic Lobule (Hexagonal)
- The traditional structural unit
- Roughly hexagonal prism of liver tissue centered on a central vein (terminal hepatic venule)
- Corners of the hexagon are occupied by portal triads (portal areas), each containing:
- Portal vein branch (thin-walled, large lumen)
- Hepatic artery branch (thick-walled, smaller lumen)
- Bile duct (lined by cholangiocytes - cuboidal/columnar epithelium)
- Lymphatics
- Blood flows centripetally: from portal triads → hepatic sinusoids → central vein
- Bile flows centrifugally: from bile canaliculi → bile ductules → bile ducts in portal triad
2. Portal Lobule
- Triangular unit centered on a bile duct at its center
- Corners are three adjacent central veins
- Emphasizes the exocrine (biliary) function of the liver
3. Liver Acinus (of Rappaport)
- Oval/diamond-shaped functional unit
- Centered on a terminal portal venule and its associated hepatic arteriole
- Divided into three zones based on proximity to blood supply:
- Zone 1 (periportal): Closest to portal triad; receives most oxygenated blood; most active in protein synthesis, gluconeogenesis, β-oxidation; first to be damaged by toxins, first to regenerate
- Zone 2 (mid-zonal): Intermediate
- Zone 3 (centrilobular / perivenular): Adjacent to central vein; lowest O₂; most active in glycolysis, lipogenesis, detoxification by CYP450 enzymes; most susceptible to ischemic damage and toxic injury (e.g., alcohol, acetaminophen)
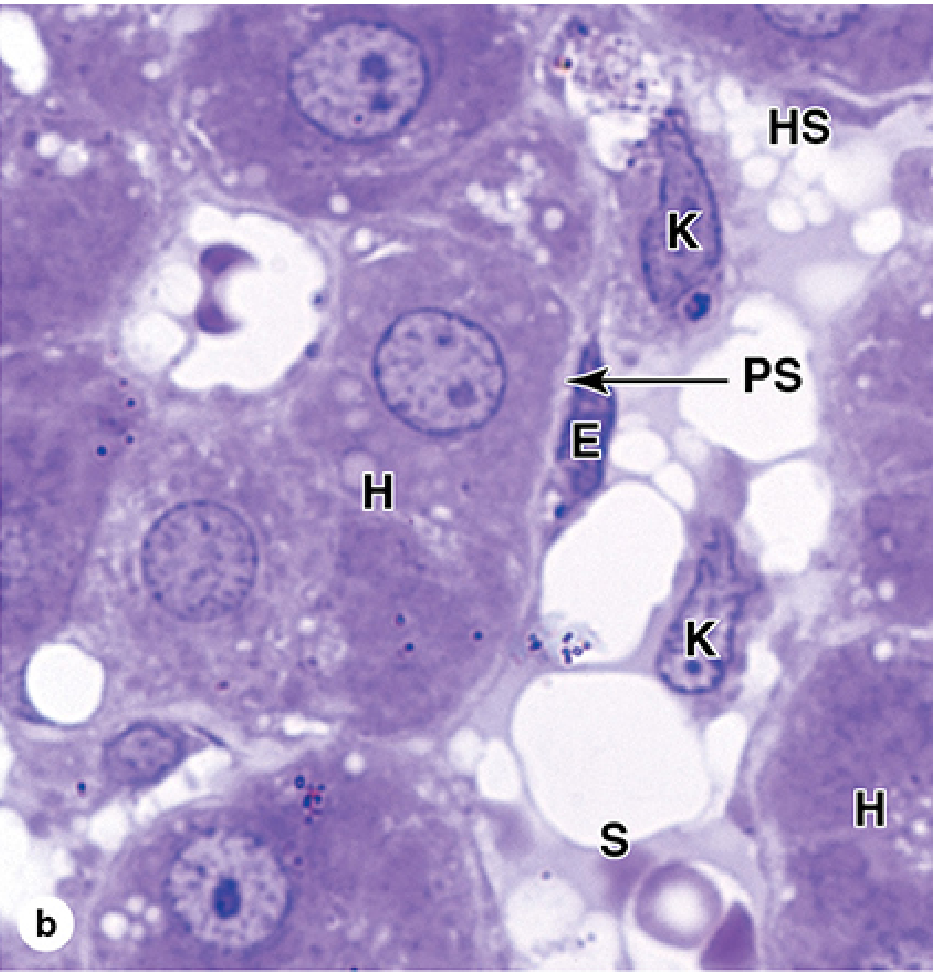
Hepatocytes
Hepatocytes are the parenchymal cells of the liver and among the most metabolically active cells in the body.
Light Microscopy
- Large polygonal cells (20-30 μm diameter)
- Round, large nucleus with prominent nucleolus; ~25% are binucleate (reflects polyploidy and active metabolism)
- Eosinophilic cytoplasm due to abundant mitochondria
- Cytoplasm may contain glycogen (clear spaces, PAS-positive) and lipid droplets
- Arranged in hepatic plates (cords) - one to two cells thick - radiating from the central vein and anastomosing with each other
Ultrastructure
- Abundant RER (protein synthesis - plasma proteins)
- Abundant SER (lipid metabolism, drug detoxification by CYP450 enzymes)
- Numerous mitochondria (~800 per cell)
- Golgi apparatus (bile component processing)
- Lysosomes and peroxisomes (oxidative reactions, H₂O₂ metabolism)
- Glycogen granules (rosettes)
- Lipid droplets (storage)
Dual Polarity of Hepatocytes
Each hepatocyte has two functional surfaces:
- Sinusoidal (basolateral) domain: faces the perisinusoidal space of Disse; exchanges substances with blood (nutrient uptake, protein secretion into blood)
- Canalicular (apical) domain: two adjacent hepatocytes form the bile canaliculus by apposing their grooved apical surfaces, sealed by tight junctions; microvilli project into the canalicular lumen
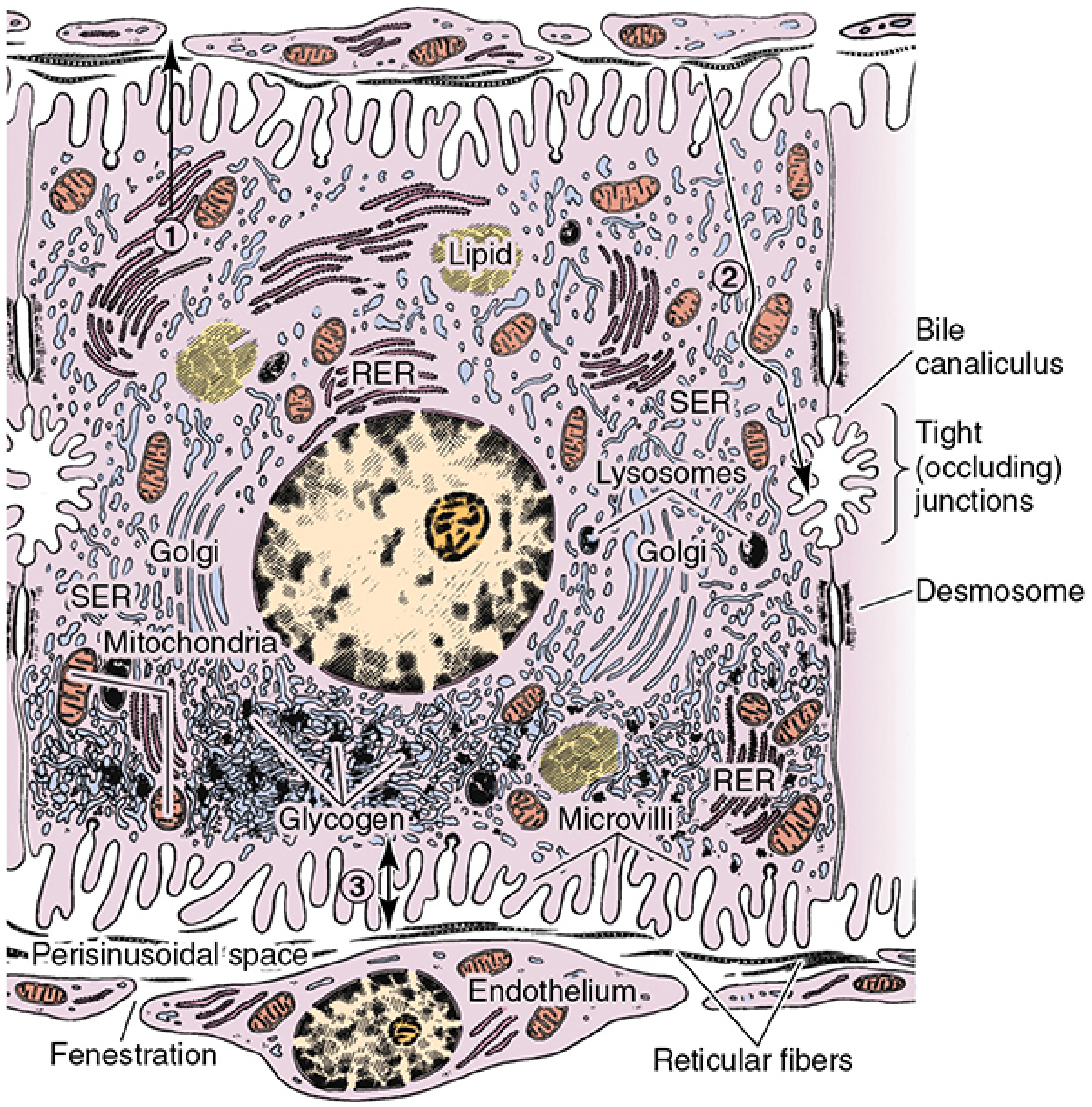
The Sinusoidal System
Hepatic Sinusoids
- Wide, irregularly shaped vascular channels between hepatic plates
- Lined by fenestrated endothelial cells (no basement membrane - "discontinuous" endothelium)
- Fenestrations allow direct exchange of proteins, lipoproteins, and other substances between blood and hepatocytes
- Between the sinusoidal endothelium and hepatocytes lies the perisinusoidal space of Disse - a narrow fluid-filled space containing reticular fibers and stellate cells
Kupffer Cells
- Specialized resident macrophages embedded in the sinusoidal endothelium
- Largest population of fixed macrophages in the body
- Stellate, with phagocytic processes projecting into the sinusoidal lumen
- Functions:
- Phagocytose effete (aged) erythrocytes, cellular debris, bacteria
- Process antigens
- Secrete cytokines (TNF, IL-1, IL-6)
- On India ink injection (experimental): appear as black stellate cells in sinusoids
Hepatic Stellate Cells (Ito Cells / Perisinusoidal Lipocytes)
- Located in the space of Disse
- Normally quiescent; store vitamin A (fat-soluble vitamin) in lipid droplets
- Small and difficult to identify in routine H&E
- When activated by liver injury → transform into myofibroblasts → secrete Type I collagen = the basis of hepatic fibrosis and cirrhosis
Bile Canaliculi and Intrahepatic Bile Ducts
- Bile canaliculi: intercellular channels formed between adjacent hepatocytes; sealed by tight junctions; 0.5-1 μm diameter but total length >1 km; microvilli project into lumen; bile flows centrifugally toward portal tracts
- Canal of Hering (bile ductules): transition zone between canaliculi and bile ducts; lined by a mix of hepatocytes and cholangiocytes; thought to contain hepatic progenitor cells
- Interlobular bile ducts: simple cuboidal-to-columnar cholangiocyte epithelium; travel with portal vein and hepatic artery branches in portal triads
- Left and right hepatic ducts: columnar epithelium
Functions of the Liver
- Exocrine: bile synthesis and secretion (bile acids, bilirubin, phospholipids, cholesterol)
- Endocrine/protein synthesis: albumin, fibrinogen, prothrombin, apolipoproteins, transferrin, complement proteins
- Carbohydrate metabolism: glycogen synthesis/glycogenolysis, gluconeogenesis
- Lipid metabolism: fatty acid oxidation, lipoprotein synthesis, ketogenesis
- Detoxification: CYP450 enzymes oxidize drugs and toxins; conjugation reactions
- Bilirubin processing: Kupffer cells phagocytose RBCs → heme → bilirubin → hepatocytes conjugate bilirubin with glucuronic acid → excreted in bile
- Iron storage: ferritin and hemosiderin in hepatocytes and Kupffer cells
- Vitamin storage: vitamin A (stellate cells), vitamins D, K, B12
Clinical Correlates: Liver
Jaundice (Icterus)
- Prehepatic (hemolytic): excess unconjugated bilirubin from RBC destruction; normal liver function
- Hepatocellular: damaged hepatocytes fail to conjugate/excrete bilirubin; both fractions elevated
- Posthepatic (obstructive): bile duct obstruction causes backpressure, bile regurgitates into blood; conjugated hyperbilirubinemia; pale stools, dark urine
Liver Cirrhosis
- End-stage result of chronic liver injury (alcohol, viral hepatitis, NASH, primary biliary cholangitis)
- Activated hepatic stellate cells produce excessive Type I collagen, replacing normal liver parenchyma with fibrotic bands
- Normal lobular architecture destroyed; formation of regenerative nodules surrounded by fibrous septa
- Consequences: portal hypertension, esophageal varices, ascites, hepatic encephalopathy, coagulopathy
Viral Hepatitis
- Hepatitis A, B, C, D, E viruses
- Histology: hepatocyte necrosis (ballooning degeneration), lobular disarray, lymphocytic infiltration, Councilman bodies (eosinophilic apoptotic hepatocytes)
- Hepatitis B/C chronic infection → cirrhosis → hepatocellular carcinoma
Non-Alcoholic Fatty Liver Disease (NAFLD/NASH)
- Steatosis: triglyceride accumulation in hepatocytes (macro/microvesicular fat droplets)
- NASH: steatosis + lobular inflammation + hepatocyte ballooning (± fibrosis)
- Zone 3 (centrilobular) predilection
Drug-Induced Liver Injury
- Acetaminophen (paracetamol) toxicity: CYP2E1 (highest in zone 3) converts excess acetaminophen to NAPQI, depleting glutathione → centrilobular (zone 3) necrosis; this is the classic histologic pattern
Hepatocellular Carcinoma (HCC)
- Most common primary liver cancer; arises on background of cirrhosis (80%)
- Associated with HBV, HCV, aflatoxin B1 exposure
- Histology: trabecular, pseudoglandular (acinar), or solid patterns; hepatocyte-like cells with large nuclei, prominent nucleoli; bile production may be seen
Wilson's Disease
- Autosomal recessive defect in ATP7B (copper transporter)
- Copper accumulates in hepatocytes → steatosis, inflammation, fibrosis; Kayser-Fleischer rings (corneal copper deposits)
- Rhodanine stain or orcein stain demonstrates copper deposits in hepatocytes
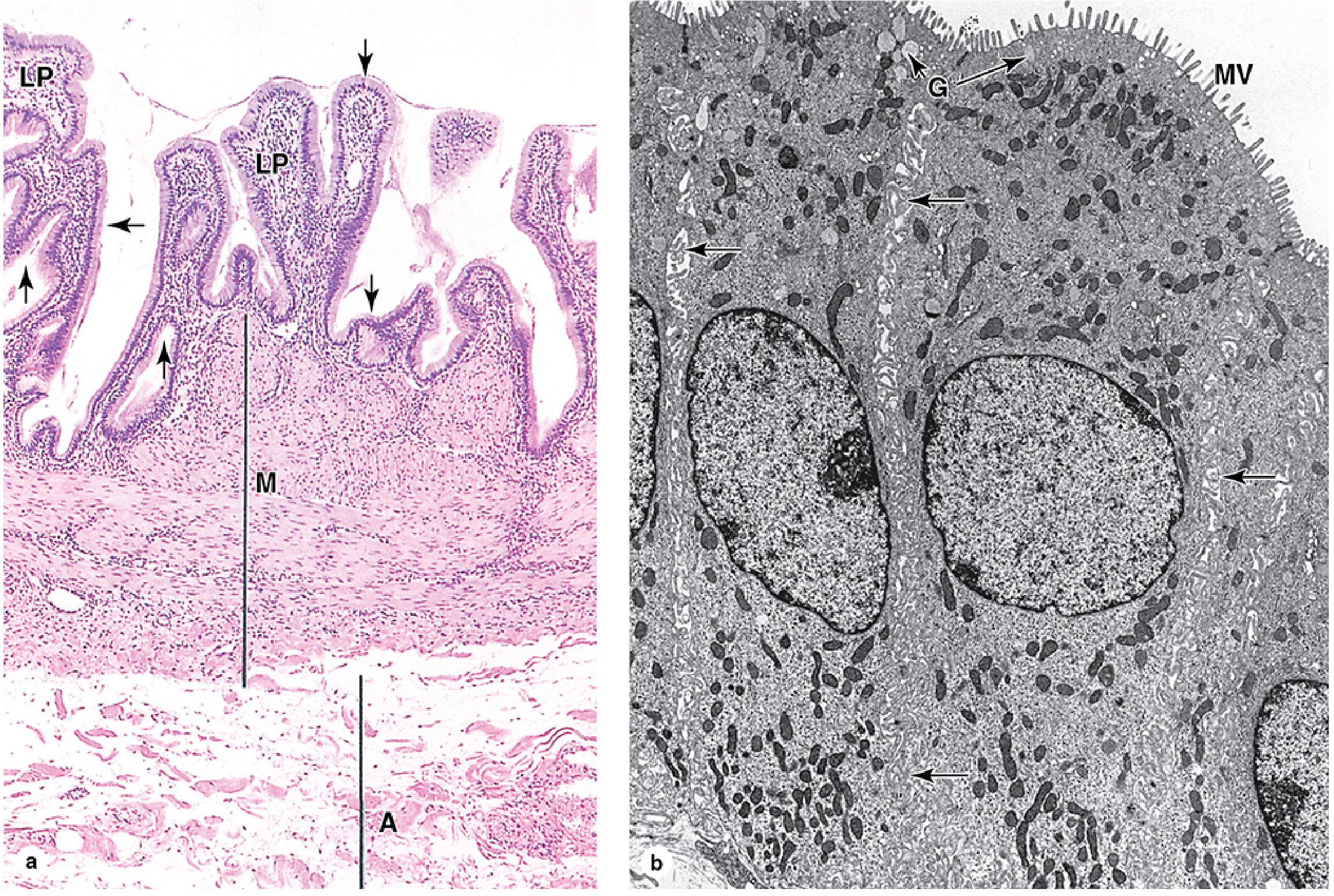
4. GALLBLADDER
General Organization
The gallbladder is a hollow, pear-shaped organ attached to the inferior surface of the liver, capable of storing 30-50 mL of bile that it concentrates 5- to 10-fold during storage. It develops from the cystic duct as an outgrowth of the bile duct system.
Layers of the Gallbladder Wall
The gallbladder wall, from inside out, consists of:
1. Mucosa
- Epithelium: simple tall columnar epithelium (cholangiocytes)
- Cells have prominent microvilli on their apical surface (for water absorption)
- Abundant mitochondria (energy for active transport)
- Distinct lateral intercellular spaces (indicative of active water transport)
- Scattered apical secretory granules containing mucus (for protection)
- No goblet cells in the main mucosa
- Lamina propria: thin layer of loose connective tissue with capillaries
- The mucosa forms prominent folds/rugae when the gallbladder is empty; these folds flatten when the organ is distended with bile
- No muscularis mucosae
2. Muscularis (Smooth Muscle Layer)
- Bundles of smooth muscle oriented in multiple directions (longitudinal, circular, oblique) - unlike the typical two-layer arrangement of the gut
- Functions to contract and expel bile into the cystic duct
- Relatively thin, not a clearly organized smooth muscle coat
3. Perimuscular Connective Tissue (Subserosal Layer)
- Loose connective tissue with vessels and nerves
- Contains Rokitansky-Aschoff sinuses: invaginations of the surface epithelium penetrating into the muscularis - these are considered features of chronic inflammation/cholecystitis but may be normal variants
4. Serosa/Adventitia
- The gallbladder has a serosa (visceral peritoneum) where it is exposed to the peritoneal cavity
- An adventitia where it contacts the liver
Bile Concentration Mechanism
The gallbladder epithelium actively concentrates bile by removing water:
- Na⁺/K⁺-ATPase in basolateral membranes pumps Na⁺ into intercellular spaces
- Cl⁻ and HCO₃⁻ follow (electroneutrality)
- Water follows osmotically via transcellular and paracellular routes
- Water is rapidly removed by subepithelial capillaries in the lamina propria
- Bile becomes concentrated 5-10x, with cholesterol, bilirubin, bile acids, and other solutes retained
Bile Flow
The bile produced by hepatocytes flows:
Bile canaliculi → Canal of Hering → Interlobular bile ducts → Right and Left hepatic ducts → Common hepatic duct → (branches as cystic duct to gallbladder) → Common bile duct → Ampulla of Vater → Duodenum
- The biliary ducts are lined by cholangiocytes - cuboidal to low columnar cells - similar to gallbladder epithelium but without the prominent water-transporting specializations
- The sphincter of Oddi at the ampulla of Vater regulates bile flow into the duodenum
- CCK (from duodenal I cells, triggered by ingested fats) → contracts gallbladder muscularis + relaxes sphincter of Oddi → bile enters duodenum
No Submucosal Layer
Unlike the rest of the GI tract, the gallbladder lacks a submucosa. The lamina propria transitions directly to the muscularis.
Clinical Correlates: Gallbladder
Cholelithiasis (Gallstones)
The most common gallbladder disease. Concentration of bile in the gallbladder is the main predisposing factor.
Types of gallstones:
-
Cholesterol stones (~80% in Western countries)
- Supersaturation of cholesterol in bile (insufficient bile salts to keep it in solution) → nucleation and crystallization
- Pure: white/yellow, often solitary, radiolucent
- Mixed: contain bile pigment as well; more common
- Risk factors: "5 Fs" - Female, Fat, Fertile (multiparous), Forty, Fair (Northern European)
-
Pigment stones (black and brown)
- Black: chronic hemolysis (e.g., sickle cell disease, hereditary spherocytosis, thalassemia) → excess unconjugated bilirubin → calcium bilirubinate crystals; usually in gallbladder; radio-opaque
- Brown: biliary infection/stasis → bacterial β-glucuronidase deconjugates bilirubin; often found in bile ducts (choledocholithiasis)
Cholecystitis
- Acute cholecystitis: gallstone impaction in the cystic duct → bile stasis → chemical/bacterial inflammation; histology: edema, neutrophilic infiltration, mucosal necrosis
- Chronic cholecystitis: repeated mild episodes → mucosal atrophy, fibrosis of muscularis, lymphocytic infiltration, Rokitansky-Aschoff sinuses (glandular herniations through the muscle wall - a hallmark feature)
Cholangitis (Primary Sclerosing / Primary Biliary)
- Primary sclerosing cholangitis (PSC): inflammation and fibrosis of bile ducts, often associated with ulcerative colitis; "onion skin" periductal fibrosis on histology; → biliary cirrhosis
- Primary biliary cholangitis (PBC): autoimmune destruction of small interlobular bile ducts; florid duct lesion - lymphocytic infiltration destroying bile duct epithelium; positive anti-mitochondrial antibodies (AMA)
Carcinoma of the Gallbladder
- Rare; most are adenocarcinomas arising from the columnar epithelium
- Strongly associated with chronic cholelithiasis and cholecystitis
- Carries a very poor prognosis (usually detected late)
Biliary Obstruction
- Causes: gallstones (choledocholithiasis), strictures, pancreatic carcinoma, cholangiocarcinoma
- Result: obstructive jaundice (conjugated hyperbilirubinemia), bile duct dilation (choledochectasis), biliary cirrhosis if chronic
- Bile duct proliferation (ductular reaction) is a histologic feature of biliary obstruction
Quick Comparison Summary
| Feature | Salivary Glands | Pancreas (Exocrine) | Liver | Gallbladder |
|---|---|---|---|---|
| Type | Exocrine (compound tubuloacinar) | Exocrine (compound acinar) + Endocrine | Both exocrine and endocrine + metabolic | Hollow sac (storage/concentration) |
| Acini type | Serous, mucous, or mixed | Serous only | N/A | N/A |
| Myoepithelial cells | Yes | No | No | No |
| Centroacinar cells | No | Yes | No | No |
| Striated ducts | Yes (key feature) | No | No | No |
| Capsule | Dense CT (major glands) | Thin, sparse CT | Glisson's capsule + visceral peritoneum | Serosa/adventitia |
| Key secretory product | Saliva (amylase, mucins, IgA) | Digestive enzymes + HCO₃⁻ fluid | Bile, plasma proteins, glucose | Concentrates bile |
| Regulation | Autonomic (parasympathetic = secretion) | CCK, Secretin, Vagal | Hormonal, portal blood | CCK (contracts) |
| Key clinical condition | Sjögren, parotitis, pleomorphic adenoma | Pancreatitis, diabetes, adenocarcinoma | Cirrhosis, hepatitis, HCC | Cholelithiasis, cholecystitis |
Sources: Junqueira's Basic Histology - Text and Atlas, 17e (ISBN 9781264930395); Ross & Pawlina's Histology: A Text and Atlas with Correlated Cell and Molecular Biology (ISBN 9781975181512)
This is a shared conversation. Sign in to Orris to start your own chat.