Antiparkinson drugs Fir 2nd yr mbbs pharmacy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the content needed for a thorough 2nd year MBBS pharmacy-level response. Let me now compile the complete notes.
Antiparkinson Drugs
2nd Year MBBS Pharmacology
Parkinson's Disease - Quick Overview
Parkinson's disease (paralysis agitans) is a progressive neurodegenerative disorder characterized by the classical tetrad:
- Tremor (resting, "pill-rolling")
- Rigidity (cogwheel/leadpipe)
- Akinesia / Bradykinesia
- Postural instability
TRAP = the mnemonic
Pathophysiology - The Key to Understanding All Drugs
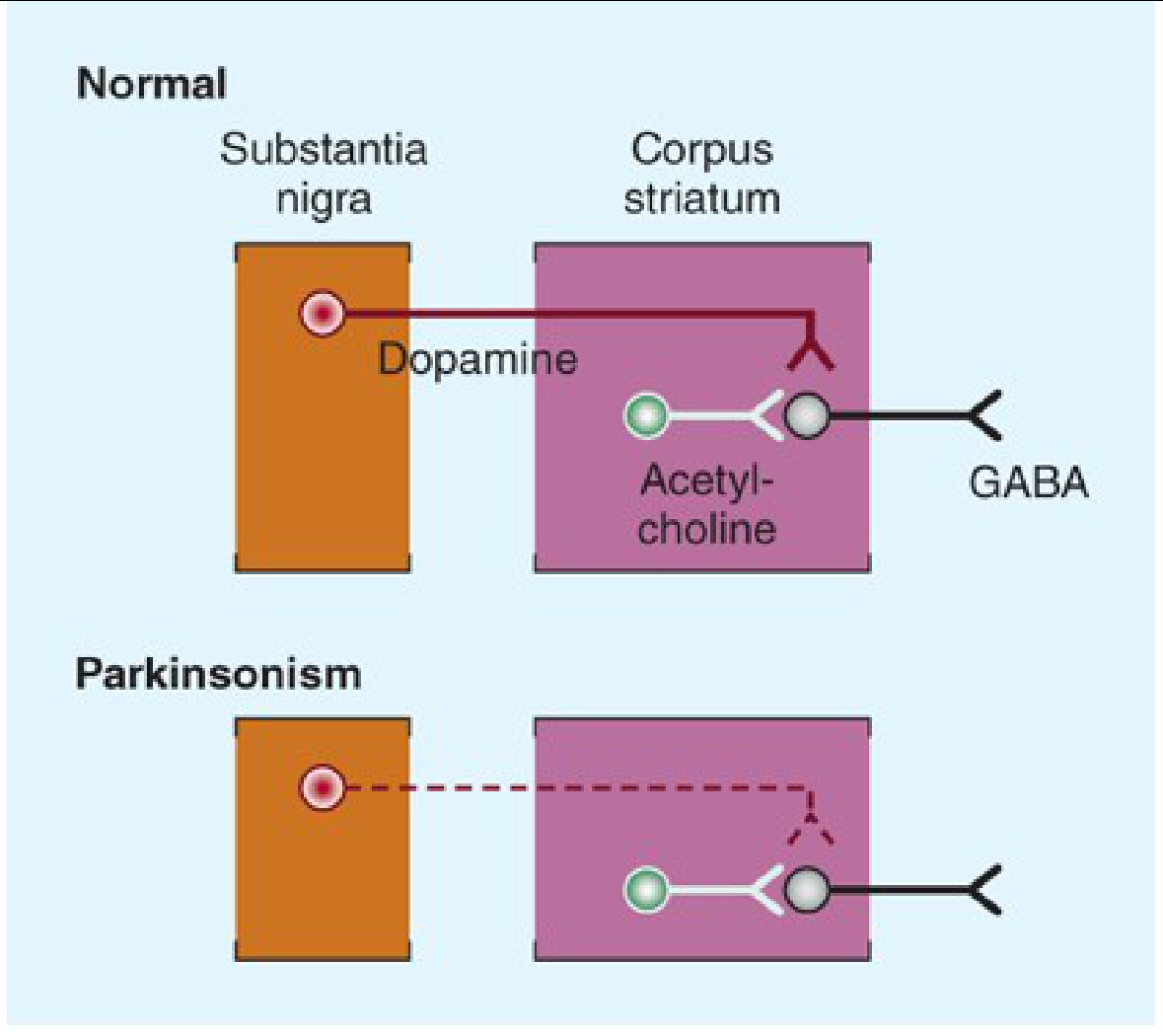
The core problem is a selective loss of dopaminergic neurons in the substantia nigra pars compacta, leading to:
- Reduced dopamine in the corpus striatum (basal ganglia)
- Unopposed cholinergic (ACh) activity in the striatum
Normal state: Dopamine (inhibitory) balances Acetylcholine (excitatory) in the striatum.
In Parkinsonism: Dopamine falls → ACh dominates → rigidity, tremor, bradykinesia.
Katzung's Basic & Clinical Pharmacology, 16th Ed.
Two therapeutic strategies follow directly from this:
- Increase dopamine activity (most drugs)
- Decrease cholinergic activity (anticholinergics)
Classification of Antiparkinson Drugs
A. Drugs that increase dopaminergic activity
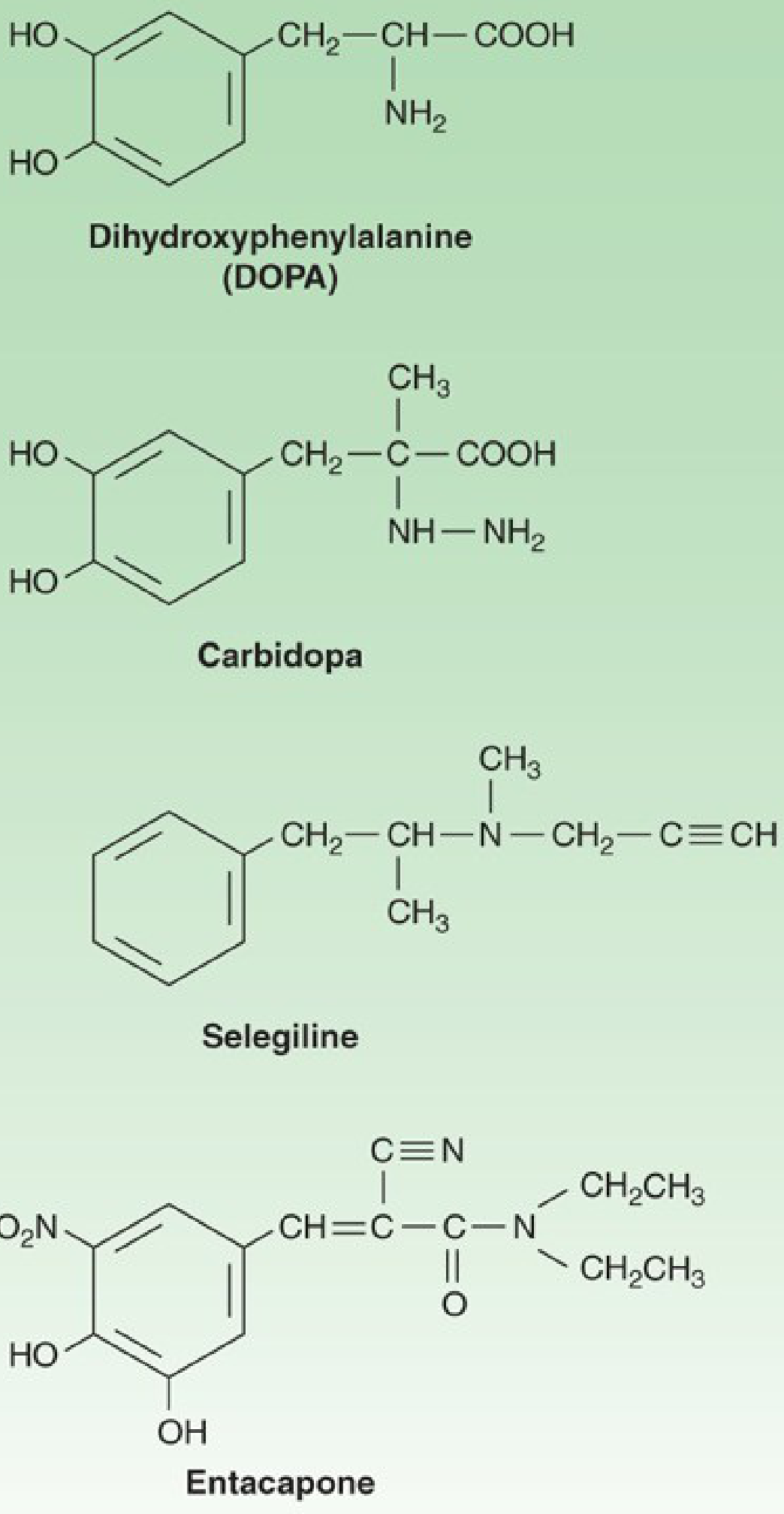
- Dopamine precursor - Levodopa (+ Carbidopa)
- Dopamine agonists - Bromocriptine, Pramipexole, Ropinirole, Rotigotine, Apomorphine
- MAO-B inhibitors (prevent dopamine breakdown) - Selegiline, Rasagiline, Safinamide
- COMT inhibitors (prevent levodopa/dopamine breakdown) - Entacapone, Tolcapone
- Dopamine releaser - Amantadine
B. Drugs that decrease cholinergic activity
- Anticholinergics - Trihexyphenidyl (Benzhexol), Benztropine, Procyclidine, Biperiden
DRUG 1: Levodopa (L-DOPA) ★★★ Most Important
Why not give dopamine directly?
Dopamine cannot cross the blood-brain barrier (BBB). Levodopa enters the brain via L-amino acid transporter (LAT) and is then converted to dopamine by DOPA decarboxylase inside the brain.
Katzung's Basic & Clinical Pharmacology, 16th Ed.
Pharmacokinetics
- Given orally; absorbed from small intestine (competition with dietary amino acids - hence best taken on empty stomach)
- ~95-99% of levodopa is decarboxylated peripherally to dopamine if given alone - this peripheral dopamine causes side effects (nausea, vomiting, cardiac arrhythmias)
- Therefore always combined with Carbidopa (a peripheral DOPA decarboxylase inhibitor that cannot cross BBB)
Levodopa + Carbidopa combination (Sinemet)
- Carbidopa blocks peripheral decarboxylation
- More levodopa reaches the brain
- Peripheral side effects reduced
- Dose of levodopa can be reduced by ~75%
- Carbidopa does NOT reduce central side effects (dyskinesias, psychosis)
Therapeutic effects
- Best drug for bradykinesia and rigidity
- Less effective for tremor
- Most effective overall symptomatic treatment of Parkinson's disease
Adverse effects
Peripheral:
- Nausea, vomiting (most common early)
- Postural hypotension
- Cardiac arrhythmias (rare)
Central (cannot be prevented by carbidopa):
- Dyskinesias (involuntary movements - most troublesome long-term effect)
- Psychiatric effects: hallucinations, confusion, psychosis
- On-off phenomenon (sudden unpredictable fluctuations between mobile "on" and immobile "off" states)
- Wearing-off effect (end-of-dose deterioration as drug duration shortens over time)
Contraindications
- Psychotic illness
- Angle-closure glaucoma
- Use with non-selective MAO inhibitors (risk of hypertensive crisis) - wait 2 weeks
- Active peptic ulcer
Important drug interactions
- Pyridoxine (Vitamin B6): Increases peripheral decarboxylation of levodopa, reducing CNS levels - this interaction is abolished when carbidopa is also given
- Antipsychotics (D2 blockers): Antagonize the effects of levodopa - avoid
- Non-selective MAO inhibitors: Hypertensive crisis
DRUG 2: Dopamine Receptor Agonists
These drugs directly stimulate dopamine receptors in the striatum - they do NOT require conversion and are not dependent on surviving neurons.
| Drug | Receptor | Route | Notes |
|---|---|---|---|
| Bromocriptine | D2 agonist (ergot) | Oral | Oldest; also used in hyperprolactinemia |
| Pramipexole | D2/D3 (non-ergot) | Oral | Preferred; may help depression |
| Ropinirole | D2 (non-ergot) | Oral | Metabolized by CYP1A2 |
| Rotigotine | D2/D3 | Transdermal patch | Continuous delivery |
| Apomorphine | D1 + D2 | Subcutaneous injection | Rescue therapy for off episodes |
Advantages over levodopa:
- Longer duration of action → less wearing-off
- No conversion needed (not dependent on surviving neurons)
- Less dyskinesia
Adverse effects (class effects):
- Nausea, vomiting
- Postural hypotension
- Psychiatric effects (hallucinations, impulse control disorders - gambling, hypersexuality)
- Ergot-specific: fibrosis (pulmonary, retroperitoneal, cardiac valvular) - reason pergolide was withdrawn
DRUG 3: MAO-B Inhibitors
Selegiline (Deprenyl) and Rasagiline selectively and irreversibly inhibit MAO-B, which is responsible for dopamine metabolism in the brain.
Result: More dopamine available in the synapse.
- Used as adjunct with levodopa to reduce wearing-off
- Selegiline dose: 5 mg with breakfast + 5 mg with lunch (avoid evening - causes insomnia via amphetamine metabolite)
- Rasagiline: 1 mg once daily; more potent; used as monotherapy in early disease too
- Possible neuroprotective effect (still debated)
Key interaction: Do NOT combine with:
- Meperidine/pethidine (risk of serotonin syndrome, hyperpyrexia)
- SSRIs or TCAs (theoretical serotonin syndrome risk)
- Sympathomimetics
- Dextromethorphan
At normal doses (selective MAO-B), the "cheese reaction" (tyramine hypertensive crisis) does NOT occur - only if MAO-A is also inhibited (higher, non-selective doses).
DRUG 4: COMT Inhibitors
Catechol-O-Methyl Transferase (COMT) breaks down both levodopa and dopamine peripherally.
- Entacapone: Peripheral COMT inhibitor; must be given with each dose of levodopa (short half-life). Does NOT cross BBB. Increases levodopa bioavailability by ~35%.
- Tolcapone: Central + peripheral COMT inhibitor; given 3x/day. More effective but causes hepatotoxicity (liver monitoring required, less commonly used now).
Use: Adjunct to levodopa to reduce wearing-off fluctuations. Never given alone.
DRUG 5: Amantadine
- Originally an antiviral drug (influenza A)
- Mechanism: Multiple - releases dopamine from nerve terminals, blocks dopamine reuptake, has mild NMDA antagonist (glutamate blocking) effect, mild anticholinergic effect
- Use: Mild early Parkinson's disease, or as adjunct; also used to treat levodopa-induced dyskinesias
- Quick onset of action but tachyphylaxis develops (loses effect within weeks to months)
- Side effects: Livedo reticularis (mottled skin discoloration), ankle edema, confusion, hallucinations
DRUG 6: Anticholinergics
By blocking muscarinic receptors in the striatum, these drugs restore the dopamine-ACh balance.
Drugs: Trihexyphenidyl (Benzhexol), Benztropine, Procyclidine
Best for: Tremor and rigidity (less effective for bradykinesia)
Side effects (antimuscarinic): Dry mouth, constipation, urinary retention, blurred vision, tachycardia, confusion (especially elderly - avoid)
Contraindications: Glaucoma, prostate hypertrophy, elderly patients (significant cognitive impairment risk)
Also used for: Drug-induced parkinsonism (from antipsychotics)
Summary Comparison Table
| Drug Class | Mechanism | Best for | Key Side Effect |
|---|---|---|---|
| Levodopa + Carbidopa | Dopamine precursor | Bradykinesia, rigidity | Dyskinesias, on-off |
| Dopamine agonists | Direct D2 stimulation | Early/adjunct | Impulse control disorder |
| MAO-B inhibitors | Prevent DA breakdown | Adjunct, early mild | Serotonin syndrome with pethidine |
| COMT inhibitors | Extend levodopa action | Wearing-off | Tolcapone hepatotoxicity |
| Amantadine | DA release + NMDA block | Mild disease, dyskinesias | Livedo reticularis |
| Anticholinergics | Block ACh in striatum | Tremor, drug-induced parkinsonism | Confusion in elderly |
Important Exam Points
- Levodopa is always combined with carbidopa (peripheral dopa decarboxylase inhibitor) to reduce peripheral side effects and increase CNS availability.
- Pyridoxine (B6) reduces levodopa efficacy ONLY when carbidopa is NOT co-administered.
- Selegiline + pethidine (meperidine) = dangerous serotonin syndrome / hyperpyrexia.
- Non-selective MAO inhibitors + levodopa = hypertensive crisis.
- Bromocriptine is an ergot dopamine agonist - also used for hyperprolactinemia, acromegaly, and neuroleptic malignant syndrome.
- Anticholinergics are preferred for drug-induced parkinsonism (from antipsychotics).
- Apomorphine is a subcutaneous dopamine agonist used as rescue therapy for severe off episodes.
- Tolcapone requires liver function monitoring (hepatotoxic); Entacapone does not.
- The on-off phenomenon and wearing-off effect are long-term complications of levodopa therapy.
- Amantadine is unique: it causes livedo reticularis and also helps treat levodopa-induced dyskinesias.
Sources: Katzung's Basic & Clinical Pharmacology, 16th Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.