scc in epidrmal nevus
"epidermal nevus" AND "squamous cell carcinoma"
"epidermal nevus" AND "malignant transformation"
Squamous Cell Carcinoma (SCC) Arising in Epidermal Nevus
Background: What is an Epidermal Nevus?
- Keratinocytic (verrucous) epidermal nevus - most common; verrucous papules coalescing into linear/whorled plaques
- ILVEN (Inflammatory Linear Verrucous Epidermal Nevus) - inflammatory, treatment-resistant, pruritic
- Nevus comedonicus, nevus sebaceous (technically adnexal), and others
SCC Arising in Epidermal Nevus
Frequency and Clinical Significance
"Rarely, cutaneous malignancies such as BCC or SCC have been reported to arise within keratinocytic epidermal nevi during adulthood."
- Fitzpatrick's Dermatology, Vol 1-2 (Course and Complications section)
Why Does Malignant Transformation Occur?
Clinical Warning Signs of SCC within an Epidermal Nevus
| Feature | Significance |
|---|---|
| Rapid growth or expansion of a previously stable lesion | Most common alarm sign |
| Ulceration within the nevus | Suggests invasive SCC |
| Bleeding, crusting, or induration | Malignant change |
| New nodule or erythematous plaque within nevus | Warrants excision biopsy |
Differential Diagnosis
- Hypertrophic lichen planus
- Verruca vulgaris
- Seborrheic keratosis (SK)
- Prurigo nodularis / lichen simplex chronicus
- Kaposi sarcoma (in intertriginous or late-stage ILVEN variants)
Course, Complications, and Special Considerations
- Congenital lesions tend to remain stable; lesions appearing post-birth may enlarge before stabilizing around puberty.
- Intertriginous lesions are prone to maceration and secondary infection.
- The epidermolytic hyperkeratosis histologic variant carries a genetic counseling implication: if the underlying K1 or K10 mutation is present in gonadal tissue, there is risk of epidermolytic ichthyosis in offspring.
Management
- Biopsy any suspicious change within an epidermal nevus - punch or excisional biopsy depending on size and location.
- Confirmed SCC: wide local excision with appropriate margins (standard SCC management principles apply).
- For the underlying nevus: full-thickness surgical excision is the most definitive treatment and has the lowest recurrence rate.
- Destructive modalities (laser ablation, cryotherapy, electrofulguration, medium- to full-depth chemical peels) may partially clear the nevus but do not remove the deep dermal component and have higher recurrence.
- ILVEN may be tried with topical steroids, retinoids, or calcipotriene, but response is typically poor.
- Fitzpatrick's Dermatology, 9th ed., "Keratinocytic Epidermal Nevus" - Course and Complications (p. 1838)
- Andrews' Diseases of the Skin, "Keratinocytic Epidermal Nevi" (p. 736); Yarak S, et al citation (An Bras Dermatol 2016; 91: 166)
- Hafner C, et al: Mosaic RAS mutations in keratinocytic epidermal nevi. J Med Genet 2012; 49: 249
Find images of histopathologic features of SCC within epidermal nevus words)
histopathology SCC squamous cell carcinoma arising epidermal nevus microscopy images
https://pmc.ncbi.nlm.nih.gov/articles/PMC5325030
Histopathologic Features of SCC Arising in Epidermal Nevus
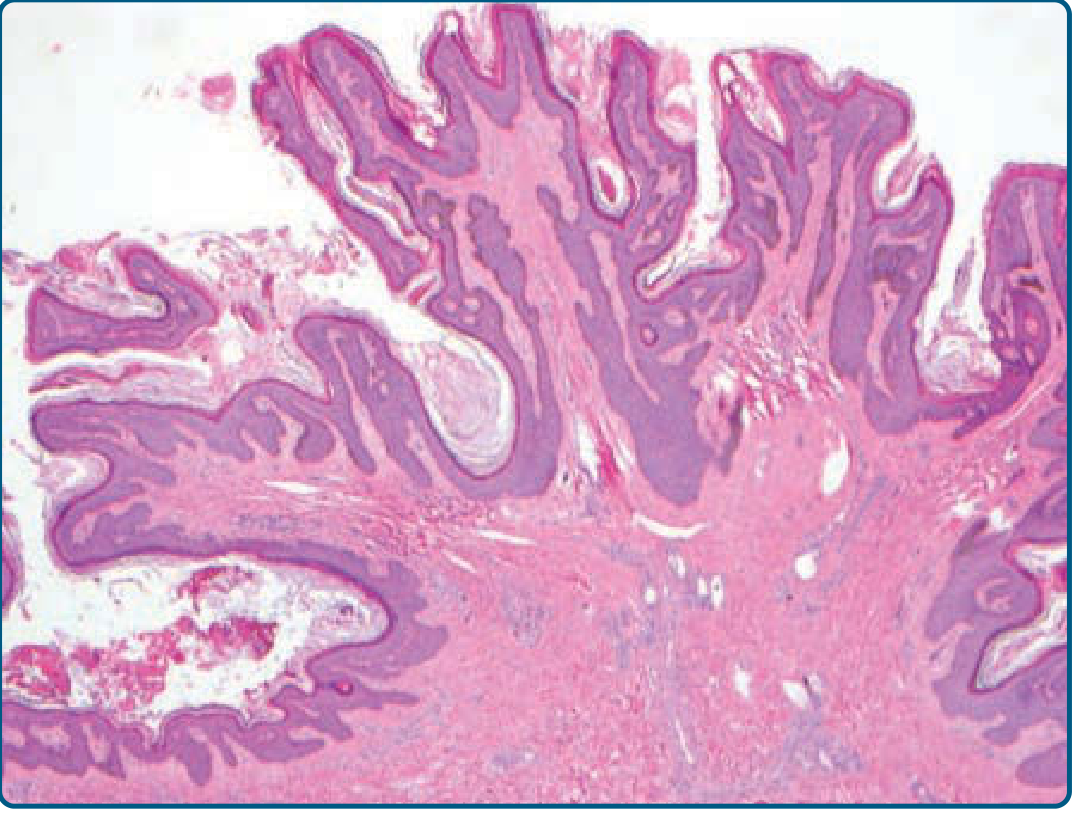
1. The Background Lesion: Epidermal Nevus Histology
- Acanthosis - irregular thickening of the epidermis
- Papillomatosis - finger-like projections of the dermal papillae
- Hyperkeratosis - thickened stratum corneum (orthokeratotic)
- Sharp lateral demarcation from adjacent normal epidermis
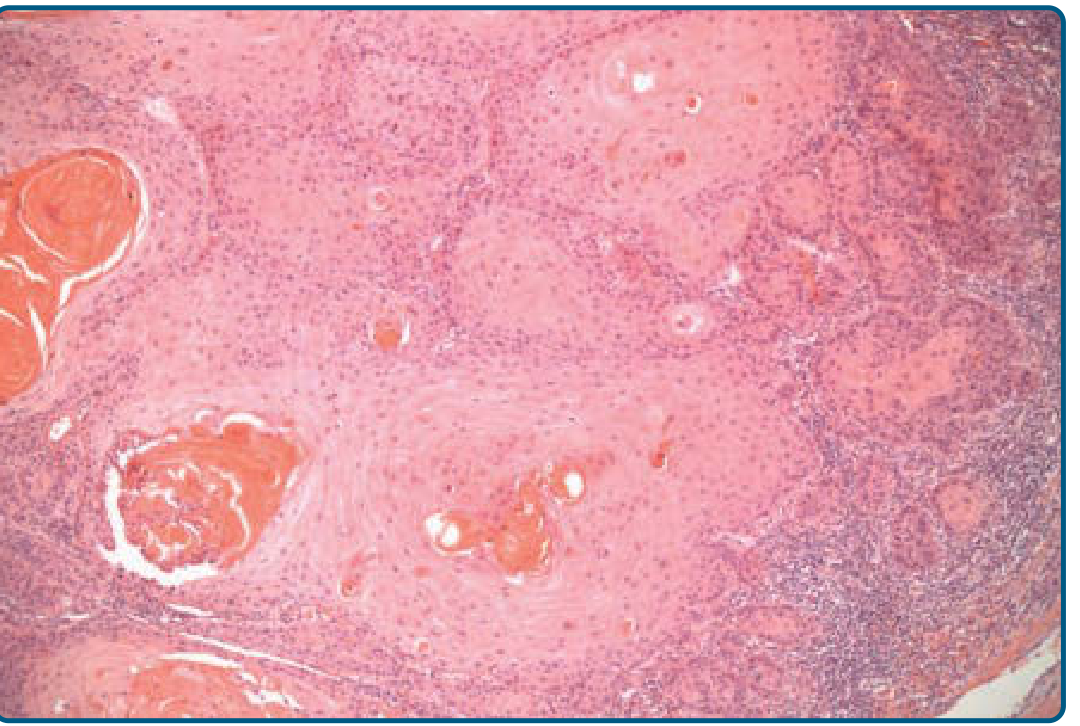
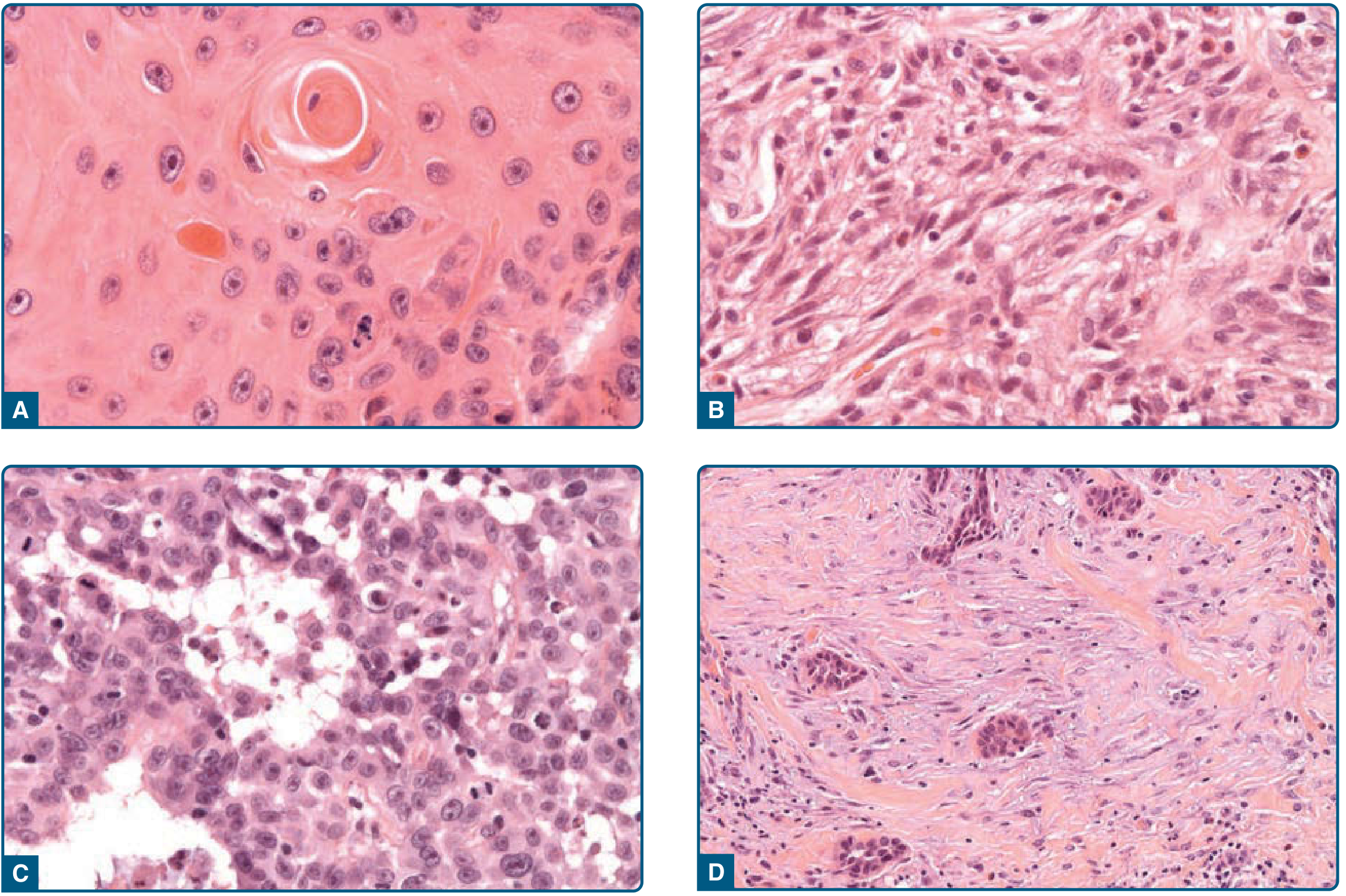
2. SCC Arising Within: Key Histopathologic Features
| Feature | Description |
|---|---|
| Keratinocyte atypia | Enlarged, pleomorphic nuclei with prominent nucleoli, increased mitoses |
| Horn pearl formation | Concentric whorls of keratin (keratin pearls) - hallmark of well-differentiated SCC |
| Individual cell dyskeratosis | Premature keratinization of single cells within the nest |
| Dermal invasion | Irregular nests and cords of atypical keratinocytes breaking through the basement membrane |
| Desmoplastic stroma | Reactive fibrotic stroma surrounding invasive nests (in desmoplastic variant) |
| Inflammatory infiltrate | Peritumoral lymphocytic infiltrate, often prominent |
| Eccrine gland involvement | Reported in published cases - SCC spreading to secretory portion of eccrine glands |
| Perineural/vascular invasion | Bad prognostic features - should be specifically reported |
3. Histopathologic Variants (All May Occur Within Epidermal Nevus)
| Variant | Key Feature | Risk Level |
|---|---|---|
| Well-differentiated | Horn pearls, minimal pleomorphism | Standard |
| Verrucous | Broad pushing borders, monomorphic cells, no invasion | Low metastatic potential |
| Acantholytic (adenoid) | Pseudoglandular spaces due to acantholysis | Higher metastatic risk (~19%) |
| Spindle-cell | Spindled atypical keratinocytes, no keratinization | High - needs IHC (cytokeratins) |
| Desmoplastic | Infiltrative narrow cords, prominent fibrous stroma | High recurrence |
4. Grading in the Histopathology Report
- Grade I (well-differentiated): Most cells differentiated; prominent keratinization and horn pearls; minimal pleomorphism
- Grade II (moderately differentiated): Intermediate features
- Grade III/IV (poorly/undifferentiated): Pleomorphic nuclei, high mitotic rate, rare keratinization; may require IHC with cytokeratins to confirm squamous lineage
- Fitzpatrick's Dermatology, 9th ed., "Basic Histopathologic Features of Squamous Cell Carcinoma" (Figs 112-6 and 112-7, p. 1938-1939)
- Fitzpatrick's Dermatology, "Keratinocytic Epidermal Nevus" (Fig 108-14, p. 1838)
- Yarak S, et al. Squamous cell carcinoma arising in a multiple verrucous epidermal nevus. An Bras Dermatol 2016; 91: 166 - biopsy findings: well-differentiated invasive SCC below VEN area, HE 40x




prepare a case report abstarct submission for up pathcon 2026 using the case of scc epidermal nevus in infraaxillary region. the case details are in the attached images. the word limit is 300. use these headings Introduction ▸ Case Details ▸ Discussion ▸ Conclusion
Abstract: Case Report Submission — UP PathCon 2026
Search pubmed for arcticles on this topic and then create the abstract under the headings i told before, keep the word limit to 300. also inc;lude the patient was ihc for hpv p16 negetive
"epidermal nevus" AND "squamous cell carcinoma"
"verrucous epidermal nevus" AND malignant transformation
PMID: 41979430
PMID: 24403890
PMID: 28300931
Abstract — UP PathCon 2026
- Riad H, et al. Case Rep Dermatol. 2013 (PMID: 24403890) - fatal metastatic SCC from VEN
- Yarak S, et al. An Bras Dermatol. 2016 (PMID: 28300931) - well-differentiated invasive SCC in multiple VEN
- Homsi HA, et al. J Cutan Pathol. 2026 (PMID: 41979430) - rare secondary neoplasms in epidermal nevus, case series + literature review