A 65 years old male attends the surgical OP with complaints of passing blood and mucous per rectum for the past 3 weeks. Rectal examination shows an ulcer on the posterior wall of rectum. Answer the following, ·What is most probable diagnosis .What are the investigations to be done .What is the management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile the complete response.
Most Probable Diagnosis
Carcinoma of the Rectum (Rectal Adenocarcinoma)
This is the most probable diagnosis in a 65-year-old male presenting with:
- Blood and mucus per rectum for 3 weeks
- Rectal ulcer on the posterior wall detected on digital rectal examination (DRE)
The clinical picture is classic. As described in S. Das's Manual on Clinical Surgery: "In ulcerative carcinoma of the rectum, the patient often passes a considerable quantity of blood-stained, purulent and offensive discharge at the time of defaecation. Excessive mucus is also discharged." Carcinoma of the rectum is painless early on - pain only appearing when the growth spreads into the pelvic cellular tissue or sacral plexus.
Differential diagnoses to consider:
- Rectal polyp (adenomatous/villous)
- Ulcerative colitis / Crohn's disease
- Solitary rectal ulcer syndrome
- Rectal tuberculosis
- Amoebiasis of the rectum
Investigations
I. To Establish the Diagnosis
| Investigation | Purpose |
|---|---|
| Proctoscopy / Rigid sigmoidoscopy | Direct visualization of ulcer; guided biopsy |
| Biopsy + Histopathology | Confirms adenocarcinoma; grades differentiation |
| Colonoscopy | Evaluates the entire colon; detects synchronous tumors (present in ~5% of cases) |
| CEA (Carcinoembryonic antigen) | Baseline tumor marker; useful for postoperative surveillance |
II. For Staging (Locoregional)
| Investigation | Purpose |
|---|---|
| MRI of pelvis | Gold standard for local staging - assesses tumor depth (T stage), nodal involvement (N stage), circumferential resection margin (CRM), and mesorectal fascia involvement |
| Endorectal ultrasound (ERUS) | Highly accurate for assessing depth of wall invasion (T staging); complements MRI |
| CT chest/abdomen/pelvis | Detects distant metastases (lung, liver, peritoneum) - Stage IV workup |
III. For Systemic/Preoperative Assessment
| Investigation | Purpose |
|---|---|
| FBC (Full blood count) | Assess anaemia from chronic blood loss |
| Liver function tests | Liver metastases, surgical fitness |
| Renal function tests + electrolytes | Pre-op workup |
| Coagulation profile (PT/INR) | Pre-op |
| ECG + Chest X-ray | Cardiorespiratory fitness for surgery |
| PET scan | Optional - reserved for ambiguous CT findings or high-morbidity operations (e.g. pelvic exenteration) |
As per Schwartz's Principles of Surgery: "For rectal cancers, digital rectal examination and rigid or flexible proctoscopy with biopsy should be performed to assess tumor size, location, morphology, histology, and fixation. Endorectal ultrasound or MRI can be invaluable in staging rectal cancer... A chest/abdominal/pelvic CT scan should be obtained to evaluate for distant metastases."
Management
Management depends on the TNM stage, tumor location, and patient fitness. The staging algorithm below guides treatment decisions:
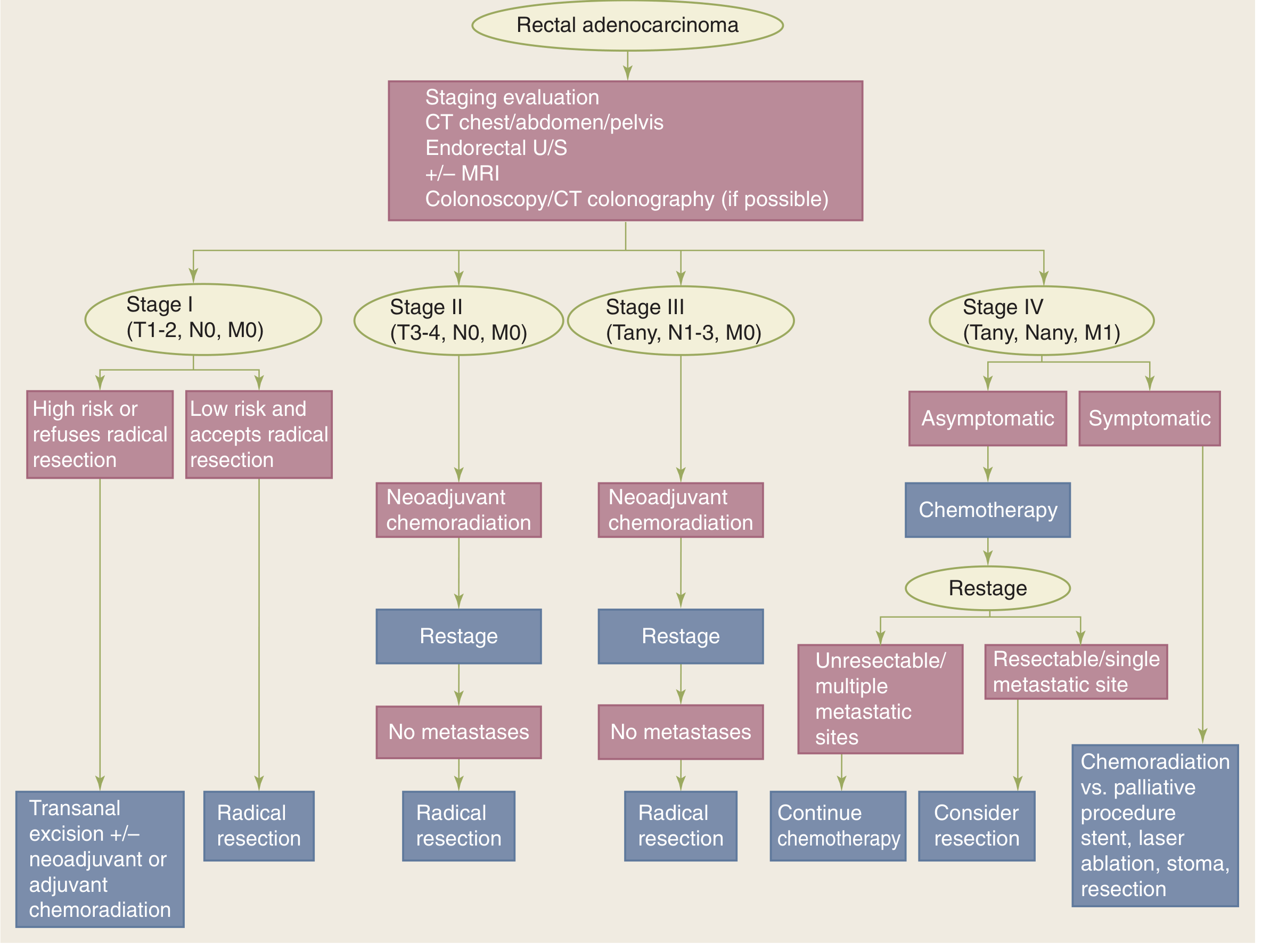
Stage I (T1-2, N0, M0) - Localized, early
- Radical resection is preferred in all fit patients.
- Local excision (transanal excision / TEM / TAMIS): limited to small (<3 cm), well-differentiated, low-risk T1N0 lesions, or patients unfit for major surgery.
- Adjuvant/neoadjuvant chemoradiation may be added for high-risk features.
Stage II & III (T3-4 or N+) - Locally advanced
- Neoadjuvant long-course chemoradiotherapy (CRT) followed by reassessment and radical resection. This downstages the tumor and improves the chance of sphincter preservation and R0 resection.
- Total Mesorectal Excision (TME) is the surgical standard - sharp dissection along embryological planes, ensuring complete excision of the mesorectal envelope to reduce local recurrence.
Surgical Options (Radical Resection)
| Procedure | Indication |
|---|---|
| Anterior Resection (AR) | Tumor ≥2 cm above the anorectal junction; sphincter-saving |
| Low Anterior Resection (LAR) + stapled anastomosis | Lower rectal tumors; preserves continence |
| Abdominoperineal Resection (APR) | Distal rectal tumors within 2 cm of anorectal junction, or poor sphincter function; results in permanent end colostomy |
Bailey & Love: "A sphincter-saving operation (anterior resection) is usually possible for tumours whose lower margin is ≥2 cm above the anorectal junction... The introduction of the stapled anastomosis and chemoradiotherapy downstaging has enabled many more patients to be treated by a sphincter-saving procedure."
Stage IV (Distant metastases)
- Chemotherapy (FOLFOX, FOLFIRI, CAPOX + targeted agents such as bevacizumab or cetuximab depending on RAS/BRAF mutation status).
- In resectable isolated liver/lung metastases: consider metastatectomy after neoadjuvant chemotherapy.
- Palliation: stenting, laser ablation, defunctioning stoma for obstruction.
Postoperative Adjuvant Therapy
- Adjuvant chemotherapy (5-FU based, or CAPECITABINE) is typically given for Stage III disease after surgery.
- For Stage II with high-risk features (T4, poor differentiation, perineural invasion, vascular invasion) - adjuvant chemotherapy is considered.
- Regular CEA monitoring and surveillance colonoscopy.
Key Summary Table
| Aspect | Detail |
|---|---|
| Diagnosis | Carcinoma rectum (adenocarcinoma) - ulcerative type |
| Essential investigations | DRE, proctoscopy + biopsy, colonoscopy, MRI pelvis, CT chest/abdomen/pelvis, CEA |
| Definitive surgery | TME (Anterior resection or APR depending on tumor level) |
| Neoadjuvant therapy | Chemoradiotherapy for Stage II/III to downstage and improve resectability |
| Adjuvant therapy | Chemotherapy for Stage III; consider for high-risk Stage II |
Sources: S. Das Manual on Clinical Surgery 13th Ed. | Schwartz's Principles of Surgery 11th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.