Posted on CICU-stuck mitral valve-whole symptoms,sign ,diagnosis n management?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"prosthetic valve thrombosis" AND thrombolysis AND management
Reading File
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Stuck Mitral Valve (Prosthetic Mitral Valve Thrombosis) - CICU Overview
"Stuck mitral valve" refers to prosthetic mitral valve thrombosis (PMVT) - a life-threatening emergency in the CICU where thrombus formation or pannus obstructs leaflet/disc movement of a prosthetic mitral valve, causing acute hemodynamic compromise.
Incidence & Risk
- Mechanical valve thrombosis: 0.3-1.3% per patient-year in high-income countries; up to 6% per patient-year in low/middle-income settings
- Mitral and tricuspid positions are more prone than the aortic position
- Risk is similar (~2%/year) for mechanical and biologic valves when anticoagulation is adequate
Key risk factors:
- Sub-therapeutic anticoagulation (most common trigger) - low mean INR
- Atrial fibrillation
- Left atrial enlargement
- LV systolic dysfunction
- Hypercoagulable states
- Prior thromboembolism
- Valve type and design
Symptoms
Onset is typically subacute, with features of both stenosis and regurgitation:
| Category | Symptoms |
|---|---|
| Low cardiac output | Fatigue, weakness, dizziness, presyncope |
| Pulmonary congestion | Dyspnea (exertional or at rest), orthopnea, PND |
| Acute decompensation | Frank pulmonary edema, cardiogenic shock |
| Embolic | Stroke, TIA, peripheral arterial emboli (arm, leg, mesenteric, renal) |
| NYHA functional class | Ranges I-II (mild, subacute) to III-IV (severe, acute) |
Clinical suspicion must be raised whenever a patient with a mechanical mitral valve presents with new-onset heart failure, thromboembolism, or low cardiac output - especially if anticoagulation has been suboptimal.
Signs on Examination
| Sign | Significance |
|---|---|
| Decreased or absent valve closure click | Hallmark - reduced or fixed leaflet motion |
| New regurgitant murmur | Leaflet unable to close fully |
| Louder-than-expected stenotic murmur | Obstruction to inflow |
| Signs of pulmonary hypertension | Loud P2, right heart failure signs |
| Signs of low cardiac output | Cool peripheries, hypotension, tachycardia, oliguria |
| Cardiogenic shock | Hypotension + signs of organ hypoperfusion |
| Neurological deficits | From systemic embolization (85% CNS involvement) |
Diagnosis
1. Clinical Suspicion
- New symptoms + subtherapeutic INR
- Absent or muffled prosthetic valve sounds
2. Echocardiography (Primary Tool)
Transthoracic Echo (TTE):
- Elevated transvalvular gradients (mean mitral gradient >5 mmHg suggests obstruction)
- Restricted leaflet/disc motion
- Visible thrombus (not always seen)
- Reduced valve area
- Elevated PASP
Transesophageal Echo (TEE) - Gold Standard:
- Better visualization of thrombus size and location (anterior vs. posterior)
- Thrombus area measurement (critical for management: <0.8 cm² vs. ≥0.8 cm²)
- Assesses leaflet excursion directly
- Important: TEE may be negative if thrombi are small or if thrombus has embolized - an embolic event in a prosthetic valve patient is presumed related to the prosthesis even with negative TEE
Echocardiographic findings:
- For mechanical valves: directly visible immobile disc/leaflet
- For bioprosthetic/TAVR valves: increased transvalvular velocity, decline in proximal-to-valve velocity ratio, leaflet thickening (HALT - hypo-attenuating leaflet thickening)
3. Cinefluoroscopy (Fluoroscopy of the Valve)
- Non-invasive, rapid, widely available
- Directly visualizes leaflet/disc opening and closing angles over several cardiac cycles
- Valve imaged en face AND at 90° angle
- Compares measured angles to manufacturer-specified normal opening/closing angles
- Fixed or restricted leaflet = diagnostic of obstruction
Classic image below - cinefluoroscopy of a bileaflet mechanical valve:
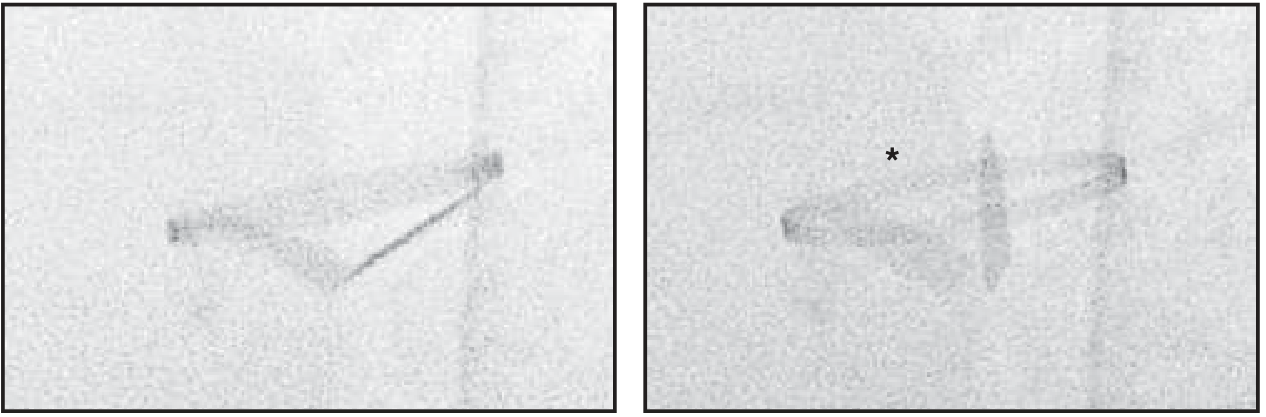
Left panel: normal diastolic opening (both leaflets open). Right panel: systole - one leaflet closes normally while the other (asterisk) remains immobile = thrombosis.
- Harrison's Principles of Internal Medicine 22E, Fig. 249-4, p. 1951
4. ECG-Gated Cardiac CT
- Excellent for visualizing thrombus vs. pannus
- Detects hypo-attenuating leaflet thickening (HALT) in bioprosthetic valves
- Used when echo is inconclusive
5. Laboratory
- INR - confirm sub-therapeutic anticoagulation
- CBC, renal and hepatic function
- BNP/NT-proBNP (severity of heart failure)
- Troponin (if ischemia suspected)
- Blood cultures if endocarditis considered
Thrombus vs. Pannus Differentiation
| Feature | Thrombus | Pannus |
|---|---|---|
| INR | Sub-therapeutic | May be therapeutic |
| Onset | Acute/subacute | Chronic, gradual |
| CT density | Low-attenuation | Higher density |
| Echo | Mobile, echo-dense mass | Fixed, hyperechoic |
| Fibrinolysis response | Good | Poor |
Management
Risk Stratification (Determines Treatment)
The two key parameters from TEE guide therapy:
- Thrombus size: <0.8 cm² (small) vs. ≥0.8 cm² (large)
- NYHA functional class / hemodynamic status
Algorithm
Suspected PMVT
|
┌────┴────┐
Shock/NYHA NYHA I-II
III-IV Stable
| |
Emergency TEE → measure
Surgery* thrombus size
┌────┴────┐
<0.8 cm² ≥0.8 cm²
Small Large
| |
Fibrinolysis Fibrinolysis
OR UFH (if surgery
not available)
or SURGERY
*Emergency Surgery is the first choice for:
- Left-sided PMVT + cardiogenic shock
- NYHA class III-IV symptoms
- Large thrombus burden ≥0.8 cm² on TEE
- Braunwald's Heart Disease, 15th Ed., p. 821
Fibrinolytic (Thrombolytic) Therapy
Indicated for:
- Recent onset (<2 weeks) + NYHA class I-II + small thrombus (<0.8 cm²)
- Sicker patients with larger thrombi when surgery is not available or is too high-risk
- Right-sided PMVT (first-line)
Regimens used:
- Slow infusion, low-dose fibrinolytic (e.g., tPA 10 mg IV bolus then 90 mg over 2 hrs; or streptokinase/urokinase regimens)
- Followed by continuous UFH infusion during transition to VKA
Contraindications to fibrinolysis:
- Recent stroke (<2 months)
- Active internal bleeding
- Large thrombus (high embolic risk)
- NYHA III-IV with available surgery
Monitoring fibrinolysis:
- Serial TTE/TEE to assess response
- Monitor INR, PTT
- If unsuccessful with UFH alone → convert to fibrinolytic therapy
Anticoagulation
- UFH infusion for small, asymptomatic or minimally symptomatic thrombi as initial therapy
- Transition to VKA (warfarin) - targeting higher INR range than baseline
- Add low-dose aspirin if not already prescribed
- Review for drug interactions and compliance
- Optimize INR to therapeutic range
Post-Treatment
- After any fibrinolytic course: continuous UFH then transition to VKA at higher target INR ± aspirin
- Serial TTE to assess treatment response
- Long-term: compliance counseling, regular INR monitoring, patient education
Key Points Summary for CICU
| Parameter | Detail |
|---|---|
| Commonest cause | Sub-therapeutic anticoagulation |
| Most specific sign | Absent/muffled prosthetic click |
| First investigation | TTE + urgent TEE |
| Gold standard imaging | TEE (thrombus size) + Cinefluoroscopy |
| Shock/NYHA III-IV | Emergency surgery |
| Small thrombus + stable | Fibrinolysis or UFH |
| Right-sided PVT | Fibrinolysis (preferred) |
| Post-therapy | Higher target INR + serial echo |
Recent evidence: A 2024 systematic review and meta-analysis in JAHA (PMID: 39291476) compared surgery vs. thrombolysis for left-sided PMVT without hemodynamic compromise - a key reference for management decisions in stable patients.
Sources:
- Braunwald's Heart Disease, 15th Ed. (Prosthetic Valve Thrombosis, p. 821)
- Harrison's Principles of Internal Medicine 22E (Cinefluoroscopy, p. 1951)
- Rosen's Emergency Medicine (Valve Thrombosis, p. 2065)
- Textbook of Clinical Echocardiography (Prosthetic Valve Thrombosis, p. 442)
This is a shared conversation. Sign in to Orris to start your own chat.