Ccb overdose emergency handling case treatmwnt
Reading File
Finding Sources
Finding Sources
Searching PubMed
"calcium channel blocker" AND "overdose" AND "treatment"
Reading File
Reading File
Reading File
Loading Image
Reading File
I have comprehensive information. Let me now compile a thorough, well-organized clinical answer.
Calcium Channel Blocker (CCB) Overdose — Emergency Management
Pathophysiology
CCBs block L-type slow calcium channels in myocardium and vascular smooth muscle, producing four toxicity domains in overdose:
- Negative chronotropy — SA node suppression → bradycardia
- Negative dromotropy — AV conduction delay → AV block
- Negative inotropy — reduced contractility → cardiogenic shock
- Vasodilation — peripheral vasoplegia → distributive shock
Verapamil is the most lethal in overdose (combines myocardial depression + vasodilation). Diltiazem is similarly cardiotoxic. Dihydropyridines (amlodipine, nifedipine) primarily cause vasodilation with reflex tachycardia at low doses, but all selectivity is lost in severe overdose.
Uniquely, CCBs also block calcium-mediated insulin secretion from pancreatic β-cells → hyperglycemia, which is a poor prognostic marker.
High protein binding and large Vd (>1–2 L/kg) make hemodialysis and hemoperfusion ineffective. — Rosen's Emergency Medicine, p. 2940
Clinical Features
| Feature | Verapamil/Diltiazem | Dihydropyridines |
|---|---|---|
| Hemodynamics | Hypotension + bradycardia | Hypotension + reflex tachycardia (early) |
| ECG | AV block (all degrees), junctional rhythm, sinus arrest, asystole | Sinus tachycardia; AV block only in severe overdose |
| Glucose | Hyperglycemia (common) | Variable |
| QRS widening | Uncommon early | Uncommon early |
Timing: IR preparations → toxicity within 1–6 hours. Extended-release (ER) preparations → toxicity may be delayed 6–16 hours. Assume ER if formulation is unknown and observe conservatively.
Pediatric note: Deaths have been reported after a single-tablet ingestion. All pediatric CCB ingestions require emergency evaluation.
Diagnosis
- ECG (obtain immediately, repeat with any hemodynamic change): look for sinus bradycardia, PR prolongation, AV block, junctional/ventricular escape rhythms
- Glucose (hyperglycemia correlates with severity, indicates HDI)
- Electrolytes — hypokalemia seen in severe overdose; serum Ca usually normal
- Lactate/ABG — lactic acidosis indicates systemic hypoperfusion
- Toxicology screen — CCB levels not routinely available or clinically useful; screen for co-ingestions (especially β-blockers, digoxin)
Differential: Hypothermia, acute coronary syndrome, hyperkalemia, hypothyroidism, cardiac glycoside toxicity, β-blocker toxicity, antidysrhythmic toxicity
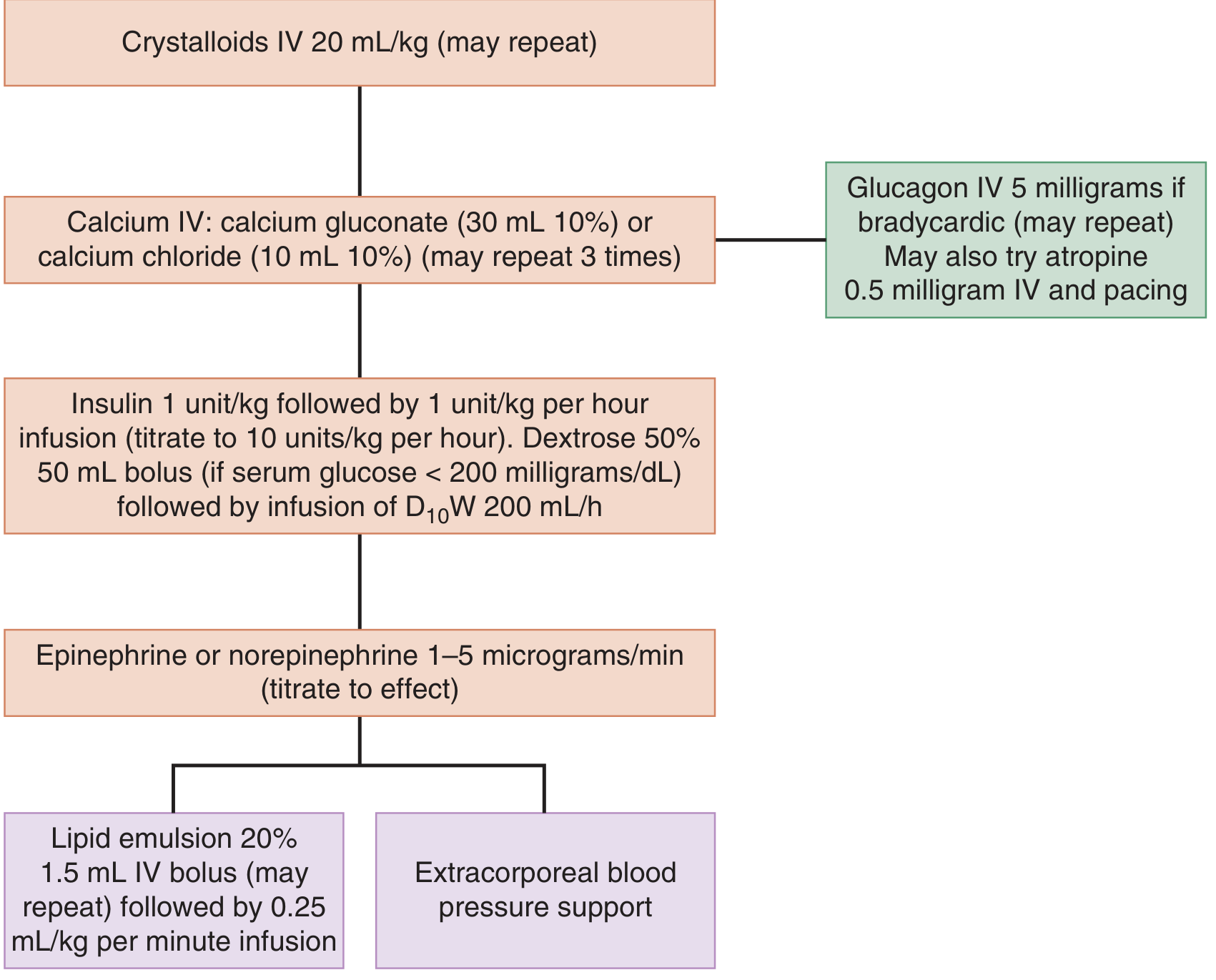
Treatment Algorithm
Step-by-Step Emergency Management
1. Immediate Stabilization
- IV access (large bore), cardiac monitoring, continuous pulse oximetry
- 12-lead ECG, frequent BP measurement
- Secure airway if GCS impaired or hemodynamic collapse imminent
2. GI Decontamination
- Activated charcoal (1 g/kg PO/NG, up to 50 g) if patient presents within 1–2 hours with a protected airway
- Whole bowel irrigation with polyethylene glycol solution should be considered for ER preparations — continue until rectal effluent is clear
3. IV Fluid Resuscitation
- Crystalloids 20 mL/kg IV bolus, may repeat
- Caution: avoid fluid overload (risk of pulmonary edema), especially in elderly or those with cardiac disease
4. Calcium Salts (First-Line Antidote)
- Calcium gluconate 10%: 30 mL IV (3 g) — preferred for peripheral IV access
- Calcium chloride 10%: 10 mL IV (1 g) — more bioavailable calcium, requires central line (risk of tissue necrosis if extravasation)
- May repeat up to 3 times; repeat every 15–20 minutes if needed
- Mechanism: increases extracellular calcium to overcome the blocked channels; transiently reverses hypotension and bradycardia
- Monitor ionized calcium levels if giving repeated doses
5. Atropine (For Bradycardia)
- 0.5 mg IV, up to 3 mg total
- Rarely fully effective; consider a temporizing measure only
- Indicated for HR <50 bpm with hypotension/symptoms
6. Glucagon
- 5 mg IV (may repeat); used mainly for co-ingested β-blocker overdose
- Not routinely recommended in pure CCB overdose — no mechanistic advantage over epinephrine, and no good clinical evidence — Rosen's, p. 2941
- Tintinalli's includes it in the algorithm as a bridging agent if bradycardia persists after calcium
7. High-Dose Insulin (HDI) — Cornerstone of Severe Overdose
This is the most important treatment for hemodynamically significant CCB poisoning. Mechanism: improves cardiac inotropy by shifting myocardial energy substrate use from fatty acids to glucose, and may improve intracellular calcium handling.
HDI Protocol (Tintinalli's Emergency Medicine, Table 195-4):
| Step | Action |
|---|---|
| Check glucose | If <200 mg/dL → give 50 mL of D50W IV (peds: 1 mL/kg of D25W) |
| Insulin bolus | Regular insulin 1 unit/kg IV |
| Insulin infusion | Start at 1 unit/kg/hour, titrate up to 10 units/kg/hour |
| Dextrose infusion | D10W at 200 mL/hour (peds: 5 mL/kg/hour) |
| Glucose target | 100–200 mg/dL |
| Glucose monitoring | Every 15–20 minutes initially; hourly once stable |
| Hemodynamic goal | HR >50 bpm, SBP >100 mmHg |
| Potassium monitoring | Replace K⁺ if <2.8 mEq/L; keep K⁺ 2.8–3.2 mEq/L |
HDI response takes 15–30 minutes — bridge with vasopressors while waiting.
8. Vasopressors
- Norepinephrine or epinephrine 1–5 mcg/min IV, titrate to effect
- Start concurrently with HDI (don't wait for HDI to kick in)
- Wean vasopressors first once hemodynamic response is seen
9. Transcutaneous / Transvenous Cardiac Pacing
- For hemodynamically significant bradycardia refractory to medications
- Note: CCB-induced bradycardia often responds poorly to pacing (unlike primary conduction disease)
10. Methylene Blue (Emerging — Vasoplegia)
- 1–2 mg/kg IV as slow infusion
- Inhibits guanylyl cyclase → reduces cGMP → increases SVR
- Particularly useful for vasoplegia unresponsive to maximum doses of norepinephrine and vasopressin
- A reasonable option when conventional vasopressors are maxed — Rosen's, p. 2941
11. Intravenous Lipid Emulsion (ILE / Intralipid)
- 20% lipid emulsion: 1.5 mL/kg IV bolus, may repeat; then 0.25 mL/kg/min infusion
- Proposed mechanism: "lipid sink" sequesters lipophilic CCB molecules
- Reserve for refractory cardiogenic shock not responding to IV fluids, calcium, HDI, and ≥3 vasopressors at max doses, AND when ECMO is not immediately available
- Evidence is limited; large follow-up studies showed poor outcomes in humans
12. ECMO (Extracorporeal Membrane Oxygenation)
- Preferred salvage therapy over lipid emulsion when available
- Indicated for patients in refractory cardiogenic arrest or shock despite all above measures
- A 2024 systematic review (PMID 38165982) confirms a role for ECMO in severe CCB overdose
- If at a non-ECMO facility, arrange urgent transfer; consider ILE as bridge
Summary — Escalation Ladder
IV Fluids + Calcium salts
↓ (if inadequate)
HDI + Vasopressors (concurrent)
↓ (if refractory)
Atropine ± Pacing | Glucagon (β-blocker co-ingestion)
↓ (if refractory)
Methylene blue (vasoplegia)
↓ (if cardiogenic shock persists)
ILE (if no ECMO) OR ECMO (preferred)
Special Considerations
| Situation | Action |
|---|---|
| ER/SR preparation ingested | Observe ≥24 hours; aggressive WBI |
| Pediatric ingestion | Any ingestion → immediate ER referral |
| Co-ingested β-blocker | Add glucagon; HDI even more critical |
| Co-ingested digoxin | Check digoxin level; Fab fragments if indicated |
| Hyperglycemia present | Start HDI regardless of vasopressor response |
| Pulmonary edema develops | Aggressive diuresis; caution with fluids |
Sources: — Tintinalli's Emergency Medicine: A Comprehensive Study, Ch. 195 | — Rosen's Emergency Medicine: Concepts and Clinical Practice, Ch. 142 | Recent ECMO evidence: Finn et al., ASAIO J 2024 (PMID 38165982)
This is a shared conversation. Sign in to Orris to start your own chat.