I now have comprehensive information. Let me compose the full HTN notes.
Hypertension (HTN) - Comprehensive Notes: Basics to Clinicals
Updated to 2025 AHA/ACC Guidelines (PMID: 40811516) and 2024 ESC Guidelines (PMID: 39210715)
1. DEFINITION & CLASSIFICATION
BP Classification (2017/2025 AHA/ACC - Adults)
| Category | SBP | | DBP |
|---|
| Normal | <120 mmHg | and | <80 mmHg |
| Elevated | 120-129 mmHg | and | <80 mmHg |
| Stage I HTN | 130-139 mmHg | or | 80-89 mmHg |
| Stage II HTN | ≥140 mmHg | or | ≥90 mmHg |
Children ≥13 years: same as adults. Children 1-12 years: percentile-based (Stage I = ≥95th percentile; Stage II = ≥95th + 12 mmHg or ≥140/90).
2024 ESC maintains the older threshold: ≥140/90 mmHg = hypertension (with "elevated normal" = 130-139/85-89 mmHg).
Key BP Phenotypes
- White coat HTN: elevated office BP but normal out-of-office readings (ambulatory/home BP)
- Masked HTN: normal office BP but elevated out-of-office readings - carries increased CVD risk
- Resistant HTN: uncontrolled BP despite ≥3 antihypertensives at optimal doses (one being a diuretic)
- Refractory HTN: uncontrolled on ≥5 agents
- Pseudoresistant HTN: apparent resistance due to poor adherence, white coat effect, or incorrect measurement
Hypertensive Crisis
- Emergency: severely elevated BP (usually >180/120) WITH acute target organ damage (TOD) - requires immediate IV treatment
- Urgency: severely elevated BP WITHOUT TOD - can be managed orally, gradual reduction over 24-48h
2. EPIDEMIOLOGY
- HTN affects ~1.28 billion adults worldwide; a leading cause of premature cardiovascular death
- Lifetime risk approaches 90% for individuals living to age 80-85
- Race/ethnicity: higher prevalence and severity in Black populations (earlier onset, greater TOD)
- HTN is present in ~85% of adults with diabetes; the two conditions are highly colinear
- Only ~50% of hypertensive patients have controlled BP globally
3. PATHOPHYSIOLOGY
Key Equation
BP = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
In chronic established HTN:
- CO is typically normal
- TPR is elevated (autoregulatory response to maintain tissue perfusion)
- Increased TPR is often a consequence - not the primary cause - of elevated BP
Renal-Body Fluid Feedback (Guyton's Concept)
The kidney is central to long-term BP regulation via pressure natriuresis - as BP rises, sodium and water excretion increases, reducing volume and resetting BP. HTN occurs when this pressure-natriuresis curve is shifted rightward, requiring a higher BP to maintain sodium balance.
Causes of impaired renal pressure natriuresis:
- Nephron loss (reduced filtration surface area)
- Increased preglomerular resistance (patchy = salt-sensitive; generalized = salt-insensitive)
- Reduced glomerular filtration coefficient (Kf)
- Increased renal tubular reabsorption (mineralocorticoid excess, Ang II excess)
RAAS (Renin-Angiotensin-Aldosterone System)
- A key function of RAAS is to allow wide variations in sodium intake without large BP fluctuations
- Reduced RAAS responsiveness (e.g., mineralocorticoid excess, Liddle syndrome) impairs suppression of renin during high sodium intake → salt-sensitive HTN
- Focal nephrosclerosis → patchy preglomerular vasoconstriction → ischemic nephrons hypersecrete renin
Neurohormonal Mechanisms
| System | Role in HTN |
|---|
| RAAS (Ang II) | Vasoconstriction, sodium retention, aldosterone release, sympathetic activation |
| Sympathetic NS | Increases CO, promotes renal sodium retention via α1-receptors, vasoconstriction |
| Endothelin-1 (ET-1) | Potent vasoconstrictor; ET-1 especially mediates salt-sensitive HTN |
| Nitric Oxide (NO) deficiency | Impairs renal pressure natriuresis; oxidative stress inactivates NO |
| Atrial Natriuretic Peptide (ANP) | Counter-regulatory; reduces preload, promotes natriuresis |
| Aldosterone | Increases distal tubule Na+ reabsorption → volume expansion → HTN |
Autoregulation Shift in Chronic HTN
In chronic HTN, the autoregulation curve shifts to higher BPs - hypertensive patients tolerate higher BP before organ damage. This is why rapid BP lowering can cause ischemia in chronically hypertensive patients (brain, kidney).
Obesity-Related HTN Mechanisms
- Renal sympathetic nerve activation → sodium retention
- RAAS activation (adipose-derived renin, angiotensinogen)
- Hyperinsulinemia → renal tubular sodium reabsorption
- ~78% of male primary HTN and ~65% of female primary HTN attributed to excess weight (Framingham)
Salt Sensitivity
- More common in older patients and in Black patients
- Characterized by rightward shift in pressure-natriuresis curve, low renin
- Caused by: aldosterone excess, high Ang II, Liddle syndrome, nephron loss
4. ETIOLOGY
Primary (Essential) HTN (~90-95%)
- No identifiable single cause
- Polygenic; influenced by lifestyle, diet (sodium, potassium), obesity, age, stress
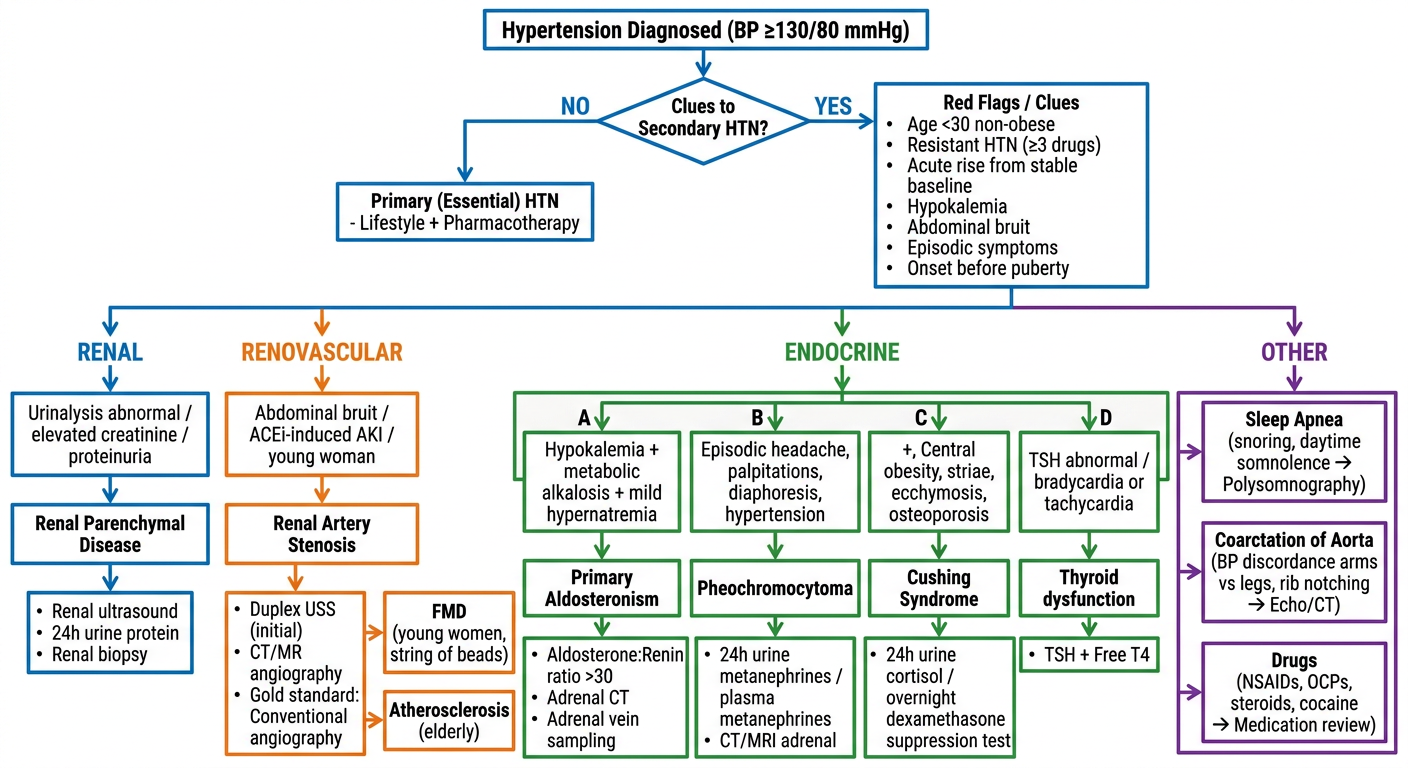
Secondary HTN (<10%)
When to suspect: severe/resistant HTN, onset before age 30 in non-obese patient, acute rise from a previously stable baseline, onset before puberty, HTN with associated electrolyte abnormalities
| Category | Condition | Key Clue |
|---|
| Renal parenchymal | CKD, glomerulonephritis, polycystic kidney disease, diabetic nephropathy | Elevated Cr, proteinuria, abnormal UA |
| Renovascular | Renal artery stenosis (FMD in young; atherosclerosis in elderly) | Abdominal bruit (diastolic), acute ↑Cr after ACEI/ARB |
| Renal artery stenosis | Fibromuscular dysplasia - "string of beads" on angiography | Young women; up to 20% of resistant HTN |
| Coarctation of aorta | Congenital narrowing of aorta | BP discordance upper vs. lower limbs; rib notching on CXR |
| Primary aldosteronism | Bilateral hyperplasia or adrenal adenoma (Conn's) | HTN + hypokalemia + metabolic alkalosis; aldosterone:renin ratio >30 (~10% of hypertensive patients) |
| Pheochromocytoma | Catecholamine-secreting tumor | Episodic headache, palpitations, diaphoresis, flushing ("5 P's") |
| Cushing's syndrome | Cortisol excess | Central obesity, thin skin, ecchymoses, osteoporosis, striae |
| Hypothyroidism | ↓Thyroid function | Raised DBP; cold intolerance, constipation; ~20% of hypothyroid patients; resolves with T4 replacement |
| Hyperthyroidism | ↑Thyroid function | Isolated ↑SBP (wide pulse pressure); treat underlying + beta-blockers |
| Acromegaly | GH excess | Arthralgias, macroglossia, jaw enlargement, headache |
| Hypercalcemia | Any cause | Direct Ca-mediated ↑SVR; avoid thiazides |
| Sleep apnea | OSA | Nondipping pattern; snoring, daytime somnolence |
| Drugs/toxins | NSAIDs, OCP, glucocorticoids, sympathomimetics, cocaine, amphetamines, cyclosporine, licorice (apparent mineralocorticoid excess) | Medication history |
| Vasculitis | PAN, Takayasu arteritis, GCA, Kawasaki | Systemic features |
5. DIAGNOSIS & EVALUATION
BP Measurement (Proper Technique)
- Patient seated, back supported, feet flat, arm at heart level, 5-min rest before measurement
- Use correct cuff size (bladder encircling 80% of arm circumference)
- Average ≥2 readings on ≥2 separate occasions
- Check both arms initially (>10 mmHg difference suggests peripheral artery disease)
- In elderly: check orthostatic BP
Out-of-Office BP Monitoring
- Ambulatory BP Monitoring (ABPM): gold standard; identifies white coat HTN, masked HTN, nondipping
- Home BP Monitoring (HBPM): average of AM + PM readings over 5-7 days
Nondipping BP
- Normal: nocturnal BP dips ≥10% from daytime
- Nondippers have increased CVD/CKD risk
- Associated with: OSA, CKD, autonomic dysfunction, diabetes
Initial Workup (All Hypertensive Patients)
History: duration, prior readings, family history, medications, lifestyle, symptoms of secondary causes
Physical exam: fundoscopy (hypertensive retinopathy), cardiovascular exam, bruits, BMI, waist circumference
Basic labs: BMP (electrolytes, BUN, Cr), fasting glucose, lipid panel, urinalysis + microalbumin, CBC
ECG: LV hypertrophy, arrhythmias
Echocardiogram: if suspected LVH or cardiac dysfunction
Target Organ Damage (TOD) Assessment
| Organ | Finding |
|---|
| Heart | LVH, CAD, HF |
| Brain | Stroke, TIA, lacunar infarcts |
| Kidney | CKD, microalbuminuria, proteinuria |
| Eyes | Hypertensive retinopathy (grades I-IV) |
| Peripheral vessels | PAD |
Keith-Wagener-Barker Retinopathy Grading
- Grade I: arteriovenous (AV) nipping, silver wiring
- Grade II: definite AV nipping
- Grade III: flame hemorrhages, soft exudates (cotton-wool spots)
- Grade IV: papilledema → hypertensive emergency
6. LIFESTYLE MODIFICATIONS (Non-Pharmacological Treatment)
Every hypertensive patient should be counseled on lifestyle modification - these alone can reduce BP significantly:
| Intervention | Expected SBP Reduction |
|---|
| Weight loss (to ideal BMI <25) | ~1 mmHg per kg lost |
| DASH diet (fruits, vegetables, whole grains, low-fat dairy, low sodium) | ~8-14 mmHg |
| Sodium restriction (<2.3 g/day, ideally <1.5 g/day) | ~5-6 mmHg |
| DASH + low sodium combined | Up to ~20.8 mmHg in SBP ≥150 mmHg |
| Aerobic exercise (150 min/week moderate intensity) | ~5-8 mmHg |
| Potassium supplementation or high-potassium diet | ~3-5 mmHg |
| Limit alcohol (<2 drinks/day men, <1 drink/day women) | ~3-4 mmHg |
| Smoking cessation | Reduces overall CV risk (acute pressor effect) |
Physical activity dose-dependently reduces HTN risk by ~6% per 10 MET-hours/week of leisure activity.
7. PHARMACOLOGICAL TREATMENT
When to Start Medications
| BP Stage | No TOD/Risk Factors | With TOD or high CVD risk |
|---|
| Elevated BP (120-129/<80) | Lifestyle only | Lifestyle only |
| Stage I (130-139/80-89) | Lifestyle ± medication (if 10-yr CVD risk ≥10%) | Start medication |
| Stage II (≥140/90) | Start medication + lifestyle | Start medication + lifestyle |
| ≥160/100 | Two-drug combination | Two-drug combination |
First-Line Drug Classes
| Class | Examples | Mechanism | Preferred In |
|---|
| ACE Inhibitors | Lisinopril, ramipril, enalapril | Block Ang I→Ang II conversion | DM, CKD with proteinuria, HFrEF, post-MI |
| ARBs | Losartan, valsartan, irbesartan | Block AT1 receptor | Same as ACEI; better tolerated (no cough) |
| Thiazide/Thiazide-like diuretics | HCTZ, chlorthalidone, indapamide | Block NCC in DCT → natriuresis | Elderly, Black patients, isolated systolic HTN; chlorthalidone preferred |
| Calcium Channel Blockers (CCB) | Amlodipine (DHP); diltiazem, verapamil (non-DHP) | Block L-type Ca channels → vasodilation (DHP) or rate/conduction (non-DHP) | Elderly, Black patients, angina, isolated systolic HTN |
| Beta-blockers | Metoprolol, carvedilol, bisoprolol | Block β-adrenergic receptors → ↓CO, ↓renin | Post-MI, HF, angina, tachyarrhythmia; NOT first-line for uncomplicated HTN per 2025 AHA/ACC |
| Aldosterone antagonists (MRA) | Spironolactone, eplerenone | Block aldosterone receptor | Primary aldosteronism, resistant HTN, HFrEF |
| Alpha-1 blockers | Doxazosin, prazosin | Block α1 receptors → vasodilation | BPH + HTN; not first-line |
| Central agonists | Clonidine, methyldopa | ↓Sympathetic outflow (α2 agonist) | Resistant HTN; methyldopa = drug of choice in pregnancy (with labetalol/nifedipine) |
| Vasodilators | Hydralazine, minoxidil | Direct arterial vasodilation | Refractory HTN; minoxidil for severe cases |
| ARNi | Sacubitril/valsartan | Block neprilysin + AT1 receptor | HFrEF with HTN |
Compelling Indications (Drug of Choice)
| Condition | Preferred Agent(s) | Avoid |
|---|
| Diabetes | ACEI or ARB | |
| CKD with proteinuria | ACEI or ARB | |
| Heart failure (HFrEF) | ACEI/ARB + beta-blocker + MRA | Non-DHP CCB (verapamil, diltiazem) |
| Post-MI | Beta-blocker + ACEI | |
| Atrial fibrillation (rate control) | Beta-blocker or non-DHP CCB | |
| Angina | Beta-blocker or CCB | |
| Isolated systolic HTN (elderly) | Diuretic or DHP-CCB | |
| Primary aldosteronism | MRA (spironolactone) | |
| Pregnancy | Labetalol, methyldopa, nifedipine | ACEI, ARB (teratogenic) |
| Black patients | Thiazide + CCB (ACEI less effective as monotherapy) | |
| Renovascular HTN (bilateral RAS) | CCB, diuretic | ACEI/ARB (risk of acute kidney injury) |
BP Targets
| Population | Target |
|---|
| General adults | <130/80 mmHg (AHA/ACC 2025) |
| Adults ≥65 years | <130/80 mmHg if tolerated (individualize) |
| CKD with proteinuria | <130/80 mmHg |
| Diabetes | <130/80 mmHg |
| Stroke prevention | <130/80 mmHg |
| Pregnancy | <140/90 (severe HTN: <160/110) |
ESC 2024 target: SBP 120-129 mmHg if tolerated for most adults; elderly target 130-139 mmHg SBP.
8. RESISTANT HYPERTENSION
Definition: BP ≥130/80 (or uncontrolled) despite ≥3 drugs at optimal doses (including a diuretic)
Steps in management:
- Confirm true resistance (exclude pseudoresistance - poor adherence, white coat effect, incorrect measurement)
- Optimize current regimen (especially add/up-titrate diuretic - chlorthalidone preferred over HCTZ)
- Screen for secondary causes (especially primary aldosteronism - most common reversible cause)
- Add MRA (spironolactone) as 4th agent - evidence from PATHWAY-2 trial
- Consider direct vasodilators (hydralazine, minoxidil)
- 42% of treatment-resistant hypertensives are physically inactive
- Device-based therapies: renal denervation (investigational but promising)
9. HYPERTENSIVE EMERGENCIES
Definition
BP usually >180/120 mmHg with acute TOD:
- Hypertensive encephalopathy: headache, confusion, vomiting, altered consciousness, papilledema
- Hypertensive ICHD / Hemorrhagic stroke
- Acute coronary syndrome (ACS)
- Acute aortic dissection
- Acute pulmonary edema
- Acute kidney injury
- HELLP syndrome / Eclampsia
- Thrombotic microangiopathy (TMA)
Management Principles
- Do NOT lower BP too rapidly - risk of ischemia due to shifted autoregulation
- Target: reduce MAP by not more than 25% in the first hour, then to 160/100-110 mmHg over 2-6h, then normalize over 24-48h
- Exception - Aortic dissection: target SBP 100-120 mmHg within minutes
IV Agents for Hypertensive Emergencies
| Drug | Mechanism | Best For | Avoid |
|---|
| Nicardipine | DHP-CCB | Most emergencies; ACS, stroke, encephalopathy | |
| Labetalol | α+β blocker | ACS, aortic dissection, perioperative | Acute HF, bronchospasm |
| Esmolol | Ultra-short β1-blocker | Aortic dissection, perioperative | |
| Clevidipine | Ultra-short DHP-CCB | Perioperative, wide applications | |
| Nitroprusside | NO donor → arterial + venous dilation | Most emergencies | Caution: cyanide toxicity, ↑ICP |
| Nitroglycerin | Venous dilation > arterial | ACS, pulmonary edema | |
| Hydralazine | Direct vasodilator | Eclampsia/pregnancy | Unpredictable response |
| Phentolamine | Alpha blocker | Pheochromocytoma, MAOI crisis | |
| Fenoldopam | D1 agonist | CKD (renal protective) | |
10. SPECIAL POPULATIONS
HTN in Pregnancy
- Gestational HTN: onset ≥20 weeks without proteinuria
- Preeclampsia: ≥20 weeks + proteinuria (>300 mg/24h) ± severe features (headache, visual changes, epigastric pain, thrombocytopenia, elevated LFTs)
- Eclampsia: preeclampsia + seizures
- HELLP: Hemolysis, Elevated Liver enzymes, Low Platelets
- Treatment: labetalol IV, hydralazine IV, oral nifedipine; magnesium sulfate for seizure prophylaxis/treatment
- ACEI and ARBs are absolutely contraindicated (fetal renal agenesis, oligohydramnios, death)
HTN in Elderly
- Predominantly isolated systolic HTN (ISH) due to large artery stiffness
- Pulse pressure increases with age as a marker of arteriosclerosis
- Start with low doses, titrate slowly
- Orthostatic hypotension is common - check standing BP
- Target: SBP <130-139 mmHg; individualize based on frailty
HTN in CKD
- CKD is both a cause and consequence of HTN
- Proteinuric CKD: ACEI/ARB preferred (reduce intraglomerular pressure)
- Monitor potassium and creatinine after starting ACEI/ARB (acceptable ≤30% creatinine rise)
HTN in Diabetes
- Most patients with T2DM have HTN (~85%)
- ACEI/ARB preferred (nephroprotective, reduce microalbuminuria)
- Target: <130/80 mmHg
11. TARGET ORGAN DAMAGE & COMPLICATIONS
| Organ | Complication | Mechanism |
|---|
| Heart | LVH, CAD, HF, AF | Pressure overload → concentric hypertrophy → diastolic dysfunction → HF |
| Brain | Ischemic stroke, hemorrhagic stroke, TIA, vascular dementia | Large artery atherosclerosis + small vessel lipohyalinosis |
| Kidneys | Nephrosclerosis, CKD, ESRD | Preglomerular vasoconstriction → ischemic nephropathy |
| Eyes | Hypertensive retinopathy, BRVO/CRVO | Arterial wall thickening, AV nipping |
| Aorta | Dissection, aneurysm | Wall stress ∝ BP × radius |
| Peripheral arteries | PAD | Accelerated atherosclerosis; 2.5x risk in men, 3.9x in women (Framingham) |
12. MONITORING & FOLLOW-UP
- After initiating therapy: recheck BP in 1-4 weeks
- Once controlled: every 3-6 months
- Annual labs: BMP (potassium monitoring on diuretics/ACEI/ARB), fasting glucose, lipids, urinalysis
- Adherence assessment at every visit
- Reassess for new secondary causes if BP deteriorates after stability
KEY MNEMONICS
ABCD for antihypertensive selection:
- A = ACE inhibitor / ARB
- B = Beta-blocker (if compelling indication)
- C = Calcium channel blocker
- D = Diuretic (thiazide)
Secondary HTN causes - "PHEO CRASH":
- Primary aldosteronism
- Hypo/hyperthyroidism
- Endocrine (Cushing, acromegaly, hyperCa)
- OSA (obstructive sleep apnea)
- Coarctation of aorta
- Renovascular disease (RAS)
- Acute/chronic kidney disease (renal parenchymal)
- Sleek (i.e., drugs - Sympathomimetics, NSAIDs, OCPs, Steroids)
- Hypercalcemia / pheocHromocytoma
RECENT GUIDELINES UPDATE (2025)
2025 AHA/ACC Guideline (PMID: 40811516 - published October 2025):
- Replaces the 2017 ACC/AHA guideline
- Maintained definition of HTN as ≥130/80 mmHg
- Emphasizes living document approach with ongoing updates
- Reaffirms universal BP target of <130/80 for most adults
- Strengthened evidence for lifestyle intervention combinations
2024 ESC Guideline (PMID: 39210715 - published October 2024):
- Maintains definition of HTN as ≥140/90 mmHg
- Introduces "elevated BP" category: 130-139/85-89 mmHg
- Recommends treatment initiation target SBP 120-129 mmHg in most adults
Sources: Fuster and Hurst's The Heart, 15th Edition; Frameworks for Internal Medicine; Textbook of Family Medicine 9e; 2025 AHA/ACC Hypertension Guideline (PMID: 40811516); 2024 ESC Guidelines (PMID: 39210715)