How to understand cns who classification in pathology pg residency
Reading File
Finding Sources
Finding Sources
Searching the Web
WHO CNS tumor classification 2021 pathology PG residency simplified guide
Reading File
Reading Web Page
https://www.pathologyoutlines.com/topic/cnstumorwhoclassific…
Reading File
Reading File
I now have excellent material from Robbins to craft a comprehensive, well-structured answer. Let me compile everything into a study guide format.
Here is a complete, PG residency-oriented breakdown of the WHO CNS Tumor Classification (5th edition, 2021) - what it means, how it changed, and how to remember it for exams and clinical practice.
WHO CNS Tumor Classification - A PG Pathology Study Guide
Why the 2021 (5th Edition) Matters
The 2021 WHO CNS5 is a major conceptual shift - not just a list update. The core idea: tumor type (defined by molecular markers) now drives classification, and grading happens within each type, not across all tumors. This aligns CNS tumors with how the rest of oncology works.
Key changes from 2016 (4th ed.) to 2021 (5th ed.):
| Old (2016) | New (2021) |
|---|---|
| Roman numerals (Grade I-IV) | Arabic numerals (Grade 1-4) |
| Grading across all tumors | Grading within tumor type |
| IDH used loosely | IDH status is a defining criterion |
| "Glioblastoma" used for IDH-mutant grade 4 | "Glioblastoma" = IDH-wildtype only |
| "Diffuse astrocytoma," "Anaplastic astrocytoma" as separate terms | Both replaced by "Astrocytoma, IDH-mutant, grade 2/3/4" |
| WHO grade | CNS WHO grade - a distinct concept |
The 3 Big Families You Must Know
1. GLIOMAS (most common primary intraparenchymal brain tumors)
A. Adult-type Diffuse Gliomas (3 types - the most tested group)
Rule of thumb: First ask IDH status, then 1p/19q codeletion
| Tumor | IDH | 1p/19q | ATRX | TERT | Grade | Key fact |
|---|---|---|---|---|---|---|
| Astrocytoma, IDH-mutant | Mutant | Intact | Lost | WT | 2, 3, or 4 | TP53 mutation also present; grade 4 if CDKN2A biallelic deletion |
| Oligodendroglioma, IDH-mutant & 1p/19q codeleted | Mutant | Codeleted | Retained | Mutant | 2 or 3 | 1p/19q codeletion is the defining molecular feature |
| Glioblastoma, IDH-wildtype | Wildtype | - | - | Mutant | 4 only | EGFR amplification, +7/-10, TERT mutation; most common CNS malignancy |
Memory tip: "IDH-mutant = younger patients, better prognosis. IDH-wildtype = older patients (>55 yr), worse prognosis."
- Glioblastoma grossly: butterfly lesion crossing corpus callosum; histology - pseudopalisading necrosis + microvascular proliferation are the two hallmarks
- Glioblastoma = ~14% of all primary CNS tumors, >50% of CNS malignancies
- Even without necrosis/microvascular proliferation, an IDH-wildtype diffuse astrocytoma qualifies as GBM if it has: TERT promoter mutation OR EGFR amplification OR +7/-10
B. Pediatric-type Diffuse Gliomas
Separate category from adult because biology is fundamentally different. Driven by MAPK pathway alterations, H3 mutations. Examples:
- Diffuse midline glioma, H3 K27-altered (e.g., DIPG - diffuse intrinsic pontine glioma) - Grade 4
- Diffuse hemispheric glioma, H3 G34-mutant - Grade 4
- Diffuse low-grade glioma, MAPK pathway-altered - Grade 1/2
C. Circumscribed Astrocytic Gliomas
- Pilocytic astrocytoma (Grade 1): Most common in children; KIAA1549::BRAF fusion; cerebellar, cystic with mural nodule; biphasic pattern, Rosenthal fibers, eosinophilic granular bodies; microvascular proliferation/necrosis do NOT upgrade it
- Pleomorphic xanthoastrocytoma (Grade 2-3): BRAF V600E mutation
2. EPENDYMOMAS
Now classified by location + molecular alteration (not just histology):
| Location | Molecular marker | Grade | Prognosis |
|---|---|---|---|
| Supratentorial | ZFTA::RELA fusion | 2-3 | Poor |
| Supratentorial | YAP1 fusion | 2-3 | Better |
| Posterior fossa | PFA group (H3K27me3 loss) | 2-3 | Poor |
| Posterior fossa | PFB group | 2-3 | Better |
| Spinal cord | NF2 mutation | 2 | Better |
| Spinal cord | MYCN amplification | 3 | Poor |
Memory tip: PFA = Poor; PFB = Better. IHC: H3K27me3 loss = PFA (loss of trimethylation).
3. EMBRYONAL TUMORS
| Tumor | Key feature | Grade |
|---|---|---|
| Medulloblastoma | Most common malignant pediatric brain tumor; posterior fossa | 4 |
| CNS PNET | Diagnosis eliminated in 2016 - no longer used | - |
| ETMR (Embryonal Tumor with Multilayered Rosettes) | C19MC amplification | 4 |
| AT/RT (Atypical Teratoid/Rhabdoid Tumor) | SMARCB1/INI1 loss | 4 |
Medulloblastoma - 4 molecular groups (must know):
- WNT-activated - best prognosis, monosomy 6, nuclear beta-catenin
- SHH-activated - intermediate, TP53 wild-type or mutant (important distinction)
- Group 3 - worst prognosis; MYC amplification, metastatic
- Group 4 - most common; isochromosome 17q
Other Important Tumor Categories
Meningiomas (most common primary brain tumor overall)
- Grade 1 (benign, most), Grade 2 (atypical), Grade 3 (malignant/rhabdoid/papillary)
- Key IHC: EMA+, S100-
- NF2 mutation common; brain invasion alone now = Grade 2
Nerve Sheath Tumors
- Schwannoma: S100+; bilateral acoustic = NF2; Antoni A and B areas; Verocay bodies
- Neurofibroma: S100 partially+; NF1 associated
Lymphomas
- Primary CNS DLBCL: most common primary CNS lymphoma; periventricular, CD20+, EBV-negative in immunocompetent; "angel wing" enhancement on MRI
Metastases
- Most common tumors involving the CNS overall (not primary)
- Common sources: lung (most common), breast, melanoma, GI, renal
The 5-Step Framework to Answer Any WHO CNS Classification MCQ
-
Is it diffuse or circumscribed?
- Diffuse → think adult (IDH/1p19q) or pediatric (H3/MAPK)
- Circumscribed → pilocytic, ependymoma, etc.
-
What is the IDH status?
- IDH mutant → astrocytoma OR oligodendroglioma
- IDH wildtype → GBM (grade 4)
-
If IDH mutant, check 1p/19q:
- Codeleted → Oligodendroglioma
- Not codeleted → Astrocytoma, IDH-mutant
-
Grade within the type:
- Astrocytoma IDH-mutant: CDKN2A biallelic deletion = automatic grade 4
- GBM IDH-wildtype: always grade 4
-
Key IHC panels:
- GFAP = glial tumors
- IDH1 R132H antibody = 90% of IDH mutations
- ATRX loss = astrocytoma (not oligodendroglioma)
- p53 overexpression = IDH-mutant astrocytoma
- OLIG2 = oligodendroglial lineage
- Synaptophysin, NeuN = neuronal tumors
- INI1/SMARCB1 loss = AT/RT
- SSTR2 = meningioma (useful for PET)
High-Yield Points for MCQs / DNB / USMLE
- "Pseudopalisading necrosis" = GBM, IDH-wildtype
- "Fried egg" cells with perinuclear halo + chicken-wire vasculature = Oligodendroglioma
- "Biphasic + Rosenthal fibers + Eosinophilic granular bodies + mural nodule in cyst" = Pilocytic astrocytoma
- "Rosettes (Homer-Wright)" = Medulloblastoma / neuroblastoma
- "Flexner-Wintersteiner rosettes" = Retinoblastoma
- "True ependymal rosettes + perivascular pseudorosettes" = Ependymoma
- "SMARCB1/INI1 loss in a child <3 years" = AT/RT
- "IDH-mutant grade 4 astrocytoma" ≠ GBM (GBM is reserved for IDH-wildtype only)
- Glioblastoma crosses corpus callosum = "butterfly glioma"
- BRAF V600E = pleomorphic xanthoastrocytoma (also papillary craniopharyngioma)
- BRAF-KIAA1549 fusion = pilocytic astrocytoma
Sources
- Robbins and Cotran Pathologic Basis of Disease (10th ed.), Chapter 28 - CNS Tumors, pp. 1193-1230
- Pathology Outlines - WHO CNS Classification
- Louis DN et al., The 2021 WHO Classification of CNS Tumors - Acta Neuropathol 2021
Explain the basic cell cytology of brain and origin of these tumors
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
brain cell types cytology neuron astrocyte oligodendrocyte microglia ependymal cell morphology function pathology
Loading Image
Reading File
I now have all the material needed for a thorough, well-illustrated answer. Let me compose it.
Basic Cell Cytology of the Brain and the Origin of CNS Tumors
This is the foundation everything else in CNS pathology builds on. If you understand what each cell normally is and does, you understand what it looks like when it goes wrong - and what tumor it gives rise to.
The Two Major Cell Populations of the CNS
The brain has two functional cell families:
- Neurons - the functional unit; signal processing
- Glia (Neuroglia) - support cells; ~10x more numerous than neurons in some regions
1. NEURONS
Cytology
- Large cells with a prominent round nucleus and a large, conspicuous nucleolus ("owl-eye nucleus" in context)
- Abundant Nissl substance (rough ER + free ribosomes) = basophilic granules in cytoplasm - reflects high protein synthesis demand
- Cytoplasmic processes: dendrites (receive input) and a single axon (transmit output)
- Completely postmitotic - cannot divide once mature; destroyed neurons are not replaced
Key IHC markers: Synaptophysin, NeuN, Neurofilament protein, Chromogranin
Response to injury
- Red neuron (acute ischemia): cell body shrinks, nucleus becomes pyknotic, cytoplasm intensely eosinophilic, Nissl substance disappears - visible by 6-12 hours
- Central chromatolysis (axonal injury/regeneration): cell body swells and rounds, nucleus pushed to periphery, Nissl substance disperses from center
- Neuronophagia: microglia surround and engulf dying neurons
Tumor origin
Neurons themselves rarely give rise to tumors (being postmitotic). Neuronal and glioneuronal tumors arise from neuronal progenitor cells or immature neurons:
- Ganglioglioma / Gangliocytoma - mature ganglion cells + neoplastic glial component
- Dysembryoplastic neuroepithelial tumor (DNET) - young patients, temporal lobe, seizures
- Medulloblastoma - embryonal tumor from cerebellar granule cell progenitors
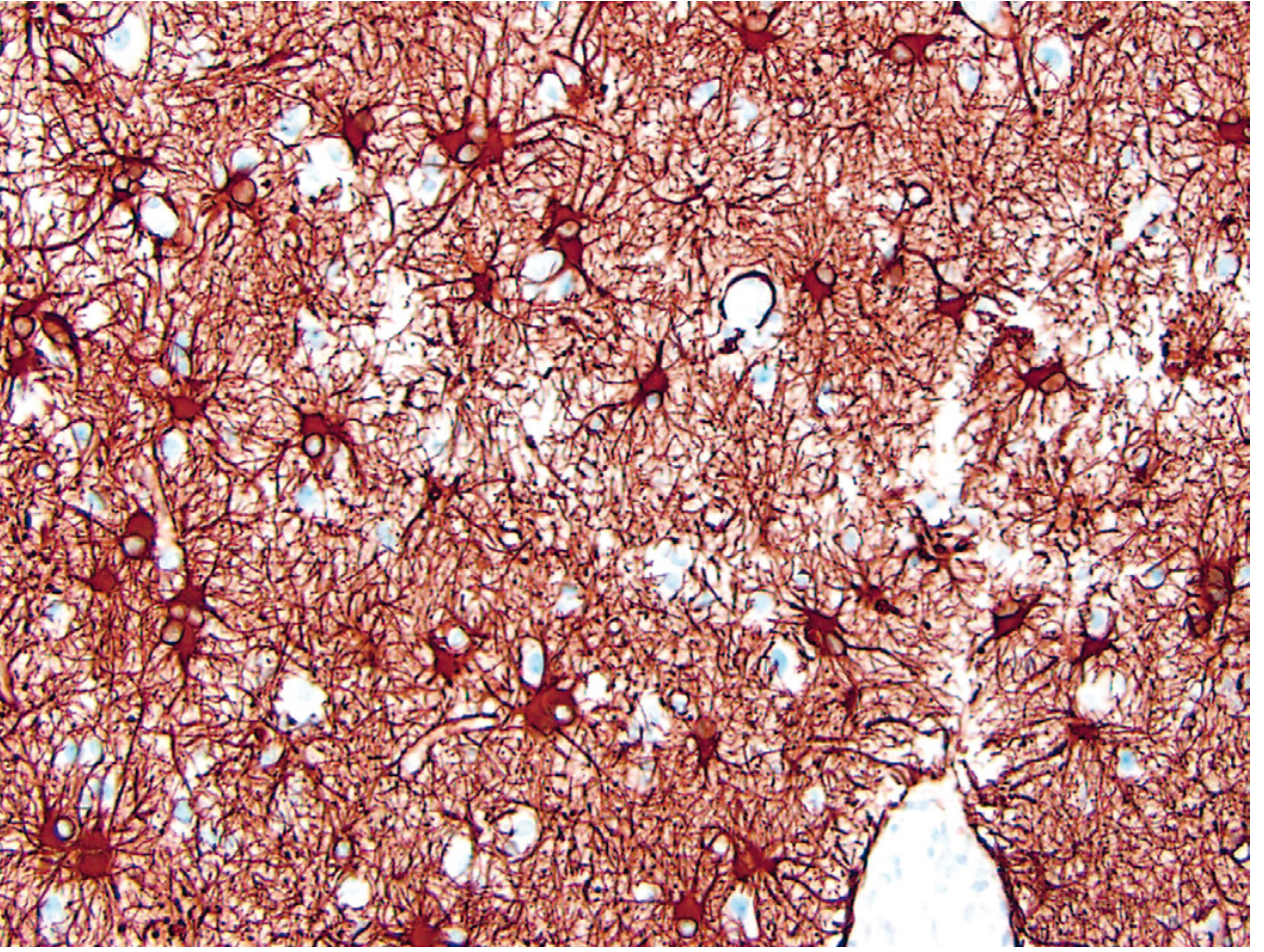
2. ASTROCYTES
Cytology
- Star-shaped (Greek: astron = star) with multiple radiating cytoplasmic processes
- Nucleus: oval, pale chromatin, inconspicuous nucleolus
- Cytoplasm typically indistinct on H&E; identified by IHC
- Two subtypes: fibrous astrocytes (white matter - long slender processes) and protoplasmic astrocytes (gray matter - short bushy processes)
- Hallmark intermediate filament: GFAP (Glial Fibrillary Acidic Protein)
Key IHC marker: GFAP+, S100+, Vimentin+
Functions
- Metabolic buffering: regulate K+, neurotransmitter reuptake (glutamate)
- Blood-brain barrier: astrocyte foot processes envelop capillary endothelium
- Structural scaffold and repair via gliosis
- Radial glia during development = a specialized astrocyte that acts as a scaffold for neuronal migration
Response to injury - GLIOSIS
- Most important CNS injury marker regardless of etiology
- Astrocytes undergo hypertrophy + hyperplasia → gemistocytic (reactive) astrocytes: plump, bright pink cytoplasm, eccentric nucleus, stout processes (GFAP overexpressed)
- Alzheimer type II astrocytes: seen in hyperammonemia (liver disease/urea cycle defects) - enlarged vesicular nucleus, glycogen droplet
- Rosenthal fibers: thick eosinophilic corkscrew inclusions in astrocyte processes; contain αB-crystallin, HSP27, ubiquitin; seen in long-standing gliosis and pilocytic astrocytoma
- Corpora amylacea: PAS-positive, basophilic, lamellated round bodies at subpial/perivascular astrocyte end-feet; increase with age (degenerative)
Tumor origin from astrocytes
Astrocytes (or their progenitors) give rise to astrocytic tumors:
| Tumor | Grade | Key molecular |
|---|---|---|
| Astrocytoma, IDH-mutant | 2, 3, or 4 | IDH mutation + TP53 + ATRX loss |
| Glioblastoma, IDH-wildtype | 4 | TERT + EGFR + +7/-10 |
| Pilocytic astrocytoma | 1 | KIAA1549::BRAF fusion |
| Pleomorphic xanthoastrocytoma | 2-3 | BRAF V600E |
3. OLIGODENDROCYTES
Cytology
- Small, round nucleus with densely packed chromatin (dark, "raisin-like")
- Scanty cytoplasm - barely visible on H&E
- Located in rows between nerve fibers in white matter (interfascicular oligodendrocytes) or scattered in gray matter (satellite oligodendrocytes)
- Each oligodendrocyte wraps around multiple internodes on multiple axons (contrast: Schwann cells in PNS wrap only one internode on one axon)
Key IHC markers: OLIG2+ (most sensitive), MBP (myelin basic protein), MOG
Function
- Myelination of CNS axons → enables saltatory conduction
- Satellite oligodendrocytes may play a metabolic support role for neurons
Response to injury
- Injury → demyelination (as in MS, PML, leukodystrophies)
- In PML (JC virus infection): viral inclusions appear within oligodendroglial nuclei
- In MSA (Multiple System Atrophy): glial cytoplasmic inclusions (GCIs) composed of α-synuclein accumulate in oligodendrocytes
Tumor origin
- Oligodendroglioma, IDH-mutant and 1p/19q codeleted (Grade 2 or 3)
- Classic histology: "fried egg" cells (perinuclear halo artifact) + "chicken-wire" vasculature + microcalcifications
- The "fried egg" perinuclear halo is a fixation artifact - not seen in frozen sections
- OLIG2 is positive in both oligodendrogliomas and astrocytomas, so it alone does not distinguish them - molecular testing is essential
4. MICROGLIA
Cytology
- Smallest glial cells
- Elongated, bean-shaped / irregular nucleus with dense chromatin
- Thin, ramified (branching) cytoplasmic processes with spine-like appendages
- Appear inconspicuous on H&E; identified by IHC
Key IHC markers: CD68+, IBA-1+, CD163+ (shared with macrophages)
Origin - UNIQUE among CNS cells
- NOT from neuroectoderm - derived from yolk sac (or fetal liver) early in embryonic development - mesodermal origin
- They are the resident macrophages of the CNS
- Share surface markers with peripheral monocytes/macrophages
Functions
- Immune surveillance - patrol CNS for pathogens and cell debris
- Synaptic pruning during development (complement-dependent) - elimination of weak synapses
- Phagocytosis of dead cells, debris, pathogens
Response to injury
Microglia show four characteristic responses:
- Proliferation
- Nuclear elongation → "rod cells"
- Microglial nodules - aggregates around small foci of necrosis (seen in viral encephalitis)
- Neuronophagia - microglia surround dying neurons
When activated, microglia transform into "amoeboid" phagocytes resembling macrophages. Aberrant activation of complement-mediated synaptic pruning by microglia is implicated in schizophrenia, Alzheimer disease, and frontotemporal dementia.
Tumor origin
Microglia are the cell of origin for primary CNS lymphoma in some contexts, but notably do not directly give rise to a major defined tumor type. However, the tumor microenvironment is heavily populated by tumor-associated microglia/macrophages (TAMs), especially in glioblastoma.
5. EPENDYMAL CELLS
Cytology
- Ciliated, columnar epithelial-like cells lining the ventricular system and central canal of spinal cord
- Cilia beat to circulate CSF
- Cuboidal to columnar in cross-section; form a single layer
- Specialized subtype: tanycytes (in floor of 3rd ventricle); choroid plexus epithelium (produces CSF)
Key IHC markers: GFAP+ (variable), EMA+, Vimentin+, S100+
Function
- Line and protect ventricular walls
- CSF circulation (ciliary movement)
- Contribute to blood-CSF barrier
Response to injury
- Ependymal granulations: when ependymal lining disrupted by inflammation or ventricular dilation, subependymal astrocytes proliferate, forming small nodular irregularities on ventricular surface
- CMV can infect ependymal cells → nuclear inclusions
Tumor origin
- Ependymomas arise from ependymal cells or their radial glial precursors
- Location + molecular alteration now defines them (WHO 2021):
- Supratentorial: ZFTA::RELA fusion (poor prognosis) or YAP1 fusion (better)
- Posterior fossa: PFA (H3K27me3 loss, poor) vs PFB (better)
- Spinal: NF2 mutation (most common spinal)
- Histology: perivascular pseudorosettes (most common - tumor cells around vessel with anuclear zone) + true ependymal rosettes (cells around a central lumen)
6. SUMMARY TABLE: Cell → Tumor
| CNS Cell | Origin | Key IHC | Tumor | Molecular |
|---|---|---|---|---|
| Neuron | Neuroectoderm | Synaptophysin, NeuN | Ganglioglioma, Medulloblastoma | WNT, SHH, H3 |
| Astrocyte | Neuroectoderm | GFAP+, OLIG2+ | Astrocytoma, GBM, Pilocytic | IDH, TERT, BRAF |
| Oligodendrocyte | Neuroectoderm | OLIG2+, MBP | Oligodendroglioma | IDH + 1p/19q codeletion |
| Microglia | Yolk sac (mesoderm) | CD68+, IBA-1+ | (No major primary tumor; role in TME) | - |
| Ependymal cell | Neuroectoderm | GFAP variable, EMA+ | Ependymoma | ZFTA::RELA, NF2, MYCN |
| Meningothelial cell | Mesodermal/neural crest | EMA+, S100- | Meningioma | NF2, TRAF7, AKT1 |
| Schwann cell (PNS) | Neural crest | S100+, SOX10+ | Schwannoma, Neurofibroma | NF2, NF1 |
The Key Concept: Tumors from Progenitor Cells, Not Mature Cells
This is the modern understanding as stated in Robbins:
"It appears these tumors are mostly derived from multipotent progenitor cells that preferentially differentiate down a particular cellular lineage."
This explains why:
- A "glioblastoma" expresses GFAP (astrocytic) but also has oligodendroglial features in some areas
- Medulloblastoma (embryonal tumor) can express neuronal AND glial markers
- The "cell of origin" and the "differentiation lineage" are not always the same thing
Neural stem cells (found in the subventricular zone and hippocampal dentate gyrus in adults) are increasingly thought to be the cell of origin for many adult gliomas - particularly in IDH-mutant tumors, where the IDH mutation is the earliest oncogenic hit that likely occurs in a progenitor cell.
Quick Memory Aid for PG Exams
- Neurons → postmitotic; red neuron = ischemia; Nissl = RER
- Astrocytes → GFAP is the marker; gliosis = injury marker; gemistocytes = reactive
- Oligodendrocytes → myelinate CNS; OLIG2; "fried egg" = oligodendroglioma
- Microglia → yolk sac origin; CD68; rod cells + microglial nodules = viral encephalitis
- Ependymal → ciliated, ventricular lining; perivascular pseudorosettes = ependymoma
- Rosenthal fibers = astrocyte inclusions in pilocytic astrocytoma + long-standing gliosis
- Corpora amylacea = aging astrocytes; PAS+, basophilic, perivascular
Sources: Robbins and Cotran Pathologic Basis of Disease, 10th ed., Chapter 28 (Cellular Pathology of the CNS, pp. 1146-1149; Tumors, pp. 1193-1220)
A great video covering all glial cell types with excellent visuals:
This is a shared conversation. Sign in to Orris to start your own chat.