What are characteristics of synovial joints b) Explain pump handle and bucket handle movement of thorax (2.5+2.5) c) Classify the muscle based on the function d) Explain motor strategies of motor control e). Explain pronation and supination. Muscle responsible, plane in which movement takes place. (3+1+1)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Here is the complete, well-structured answer to all five questions.
a) Characteristics of Synovial Joints
Synovial joints are also called true joints (diarthroses). Unlike false joints (synarthroses) where surfaces are connected, synovial joints have articulating surfaces separated by a cavity. The joint capsule produces synovial fluid, giving this joint type its name.
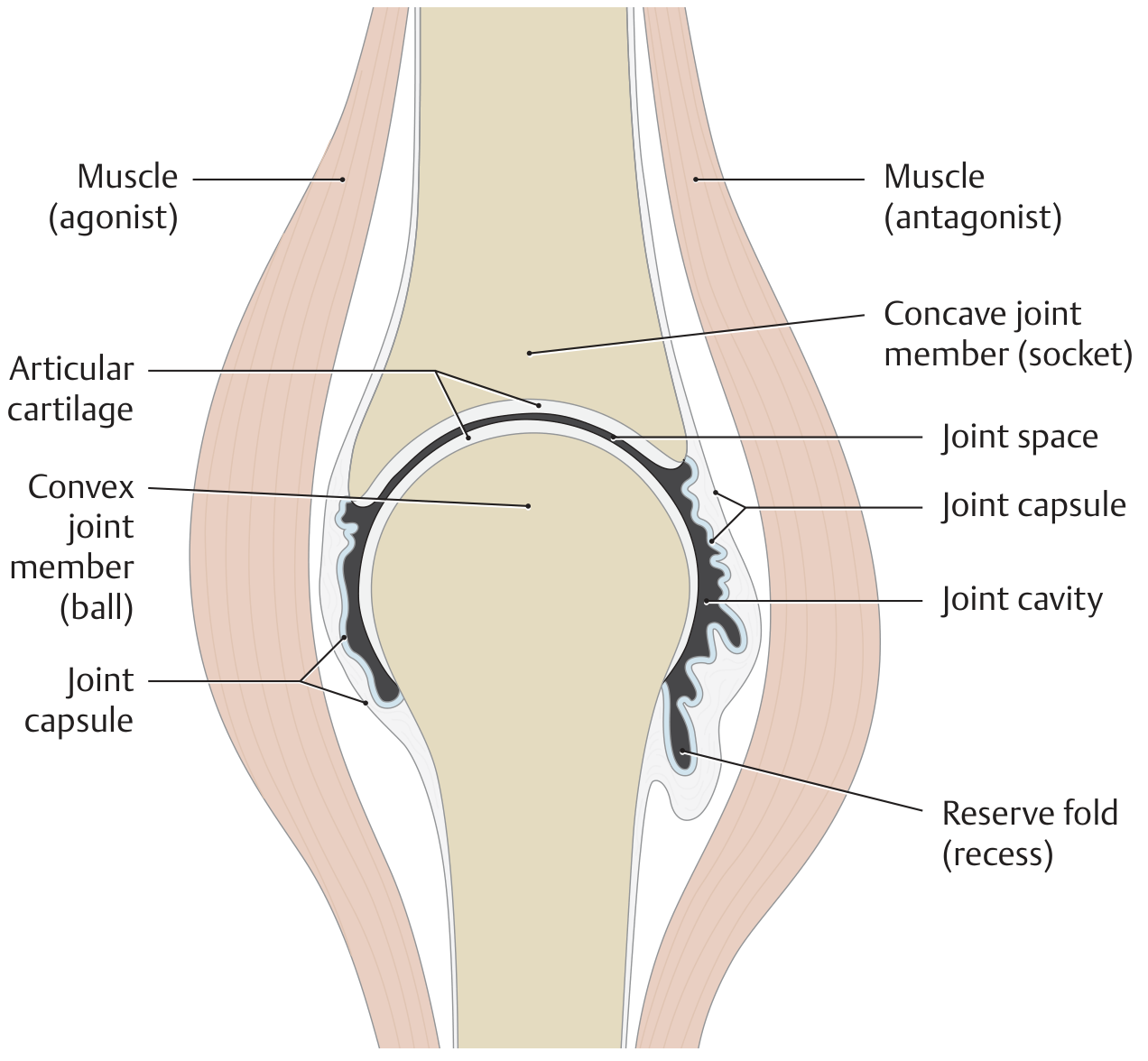
Characteristics:
-
Articular cartilage - Variously shaped articular surfaces covered by hyaline cartilage, which reduces friction and distributes compressive forces.
-
Joint cavity - A potential space between the articulating bones, with articular recesses that vary in width.
-
Joint capsule - An all-around closed fibrous capsule, which is reinforced by alar folds, synovial folds, and synovial villi. It has two layers:
- Outer fibrous layer (stratum fibrosum)
- Inner synovial layer (stratum synoviale) - produces synovial fluid
-
Synovial fluid - Highly viscous fluid produced by the joint capsule. It lubricates the joint, nourishes articular cartilage, and provides shock absorption.
-
Intra-articular structures - Present in some joints to improve congruency and increase force-absorbing surface area:
- Menisci (e.g., knee) - crescent-shaped, wedge in cross section
- Articular discs (e.g., sternoclavicular, temporomandibular joints) - divide the joint into two chambers
- Labra (e.g., hip, shoulder) - wedge-shaped fibrocartilaginous rims that deepen the socket
-
Ligaments - Intra- and extracapsular ligaments act as primary joint stabilizers.
-
Muscles - The joint is crossed by muscles moving it in opposite directions (agonist/antagonist pair).
-
Synovial bursae - Fluid-filled sacs often located near the joint, sometimes communicating with the joint cavity, reducing friction between structures.
Note: Not all of the above are present in every synovial joint.
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
b) Pump Handle and Bucket Handle Movements of the Thorax
During breathing, the dimensions of the thorax change in the vertical, lateral, and anteroposterior directions. Two named rib movements account for the anteroposterior and lateral changes.
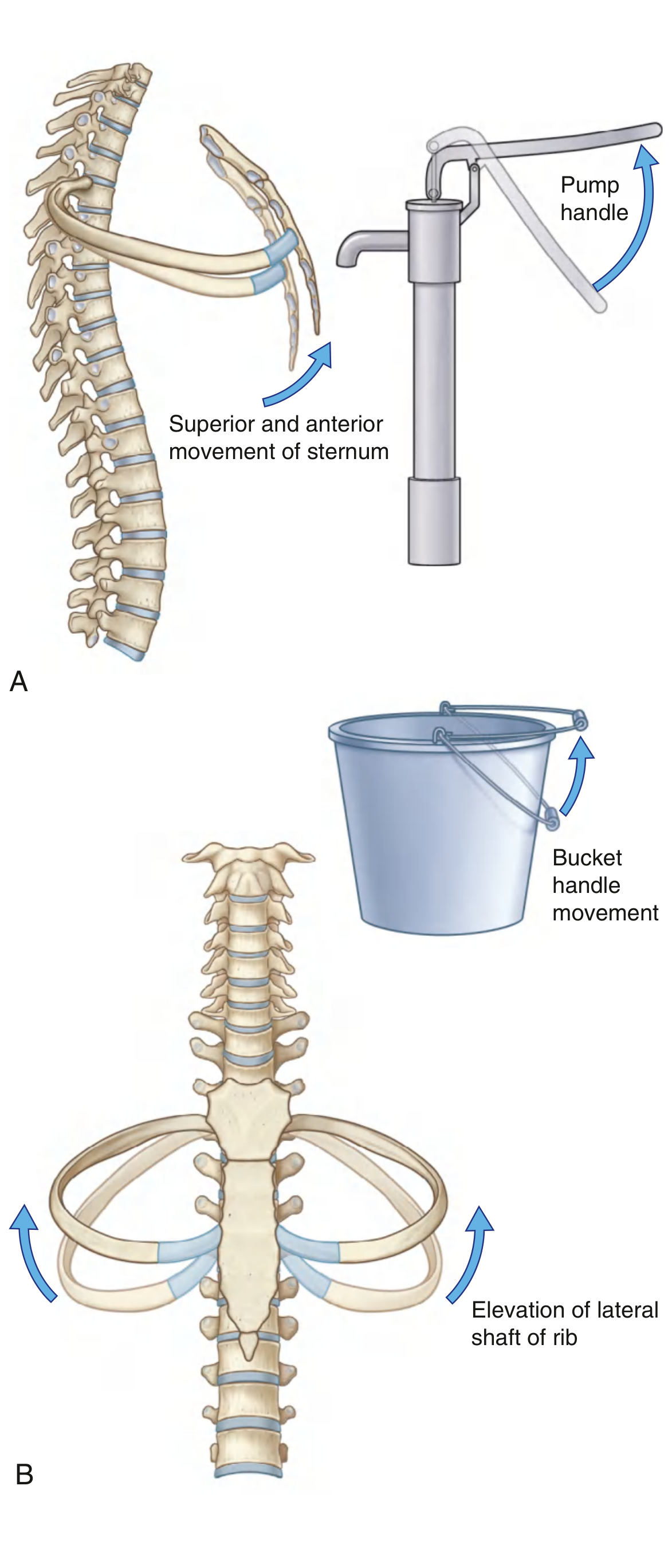
Pump Handle Movement (Anteroposterior diameter)
- The posterior ends of ribs articulate with the vertebral column; the anterior ends are lower than the posterior ends.
- When the ribs are elevated during inspiration, this geometry causes the anterior end (and attached sternum) to move upward and forward - like the handle of an old-fashioned water pump being raised.
- This increases the anteroposterior (AP) diameter of the thorax.
- Predominantly involves the upper ribs (ribs 1-6), especially ribs 2-6.
- On depression (expiration), the sternum moves downward and backward.
Axis of rotation: The axis runs roughly in the coronal plane through the costovertebral joint.
Bucket Handle Movement (Transverse/lateral diameter)
- In addition to the anterior ends being lower than the posterior ends, the middles of the rib shafts are lower than both ends - like a bucket handle lying flat.
- When the rib shafts are elevated during inspiration, the middles of the shafts swing upward and outward laterally - like a bucket handle being lifted.
- This increases the transverse (lateral) diameter of the thorax.
- Predominantly involves the lower ribs (ribs 7-10), which have more lateral flare.
Axis of rotation: The axis runs roughly in the sagittal (AP) plane through the costovertebral and sternocostal joints.
Both movements occur simultaneously during normal breathing, with pump handle predominating in the upper thorax and bucket handle in the lower thorax.
- Gray's Anatomy for Students
c) Classification of Muscles Based on Function
Muscles can be classified based on their functional role during a given movement:
| Functional Class | Description | Example |
|---|---|---|
| Prime Mover (Agonist) | The muscle primarily responsible for producing a movement | Biceps brachii in elbow flexion |
| Antagonist | A muscle that opposes or reverses the action of the agonist; relaxes as agonist contracts | Triceps brachii during elbow flexion |
| Synergist | Assists the agonist in producing movement; helps fine-tune or refine the action | Brachialis assisting biceps in elbow flexion |
| Fixator (Stabilizer) | Fixes or stabilizes the proximal joint/origin so the agonist has a firm base to act from | Rotator cuff muscles stabilizing the shoulder while the biceps flexes the elbow |
| Neutralizer | Cancels out an unwanted secondary action of the agonist | Wrist extensors neutralizing the wrist flexion tendency of finger flexors |
Additional functional categories:
- Postural muscles (tonic) - Continuously active to maintain body posture against gravity (e.g., soleus, erector spinae). Rich in slow-twitch (Type I) fibers.
- Phasic muscles - Activated for rapid, forceful movements. Rich in fast-twitch (Type II) fibers (e.g., gastrocnemius, rectus femoris).
- Multi-articular muscles - Cross more than one joint and act on multiple joints (e.g., rectus femoris, hamstrings).
- Shunt muscles - Oriented to produce compression/stabilization across a joint rather than angular motion (e.g., brachioradialis).
- Spurt muscles - Produce primarily angular movement at a joint (e.g., brachialis).
Classification criteria also used in anatomy: origin, topography, and innervation.
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
d) Motor Strategies of Motor Control
Motor strategies are the organized, stereotyped responses the nervous system uses to maintain balance and control movement following perturbations. Research from Kandel's Principles of Neural Science describes these in detail:
Three Core Postural Motor Strategies
1. Ankle Strategy
- Used when: Small, slow perturbations on a firm, wide surface
- Mechanism: The body sways as a single inverted pendulum, rotating about the ankle joints. Muscles contract around the ankle (gastrocnemius/tibialis anterior) to restore the center of mass (CoM) over the base of support without moving the feet.
- Base of support: Remains fixed
- Key feature: The feet stay in place; correction occurs from the ground up (distal to proximal muscle activation sequence)
2. Hip Strategy
- Used when: Larger, faster perturbations or on narrow/compliant surfaces
- Mechanism: Rapid flexion or extension at the hip joints shifts the CoM. Trunk and hip muscles are activated first (proximal to distal sequence), which is the reverse of the ankle strategy.
- Base of support: Remains fixed, but hip motion shifts the CoM rapidly
- Key feature: Produces a countermovement of the trunk and legs in opposite directions
3. Stepping (Change-in-Support) Strategy
- Used when: The perturbation is so large that the CoM cannot be recovered with the ankle or hip strategy
- Mechanism: A rapid step or multiple steps are taken to move the base of support under the displaced CoM. Similarly, the hand may grab a support to enlarge the base.
- Base of support: Changed/enlarged
- Key feature: Longest latency, allowing cortical input (choice of which foot, direction, avoiding obstacles)
Key Features of Automatic Postural Responses
-
They are not simple stretch reflexes but synergistic activation of muscle groups in a characteristic sequence.
-
Latency in humans: 90-120 ms in ankle muscles (longer than stretch reflex, shorter than voluntary reaction time).
-
The nervous system selects the appropriate strategy based on the size and speed of perturbation, the surface conditions, and prior experience/anticipation.
-
Anticipatory postural adjustments (APAs) also occur - the CNS pre-activates postural muscles before a voluntary limb movement to counteract the expected postural disturbance.
-
Eric Kandel, Principles of Neural Science, 6th Edition; Scott-Brown's Otorhinolaryngology
e) Pronation and Supination
Definition
- Supination - Rotation of the forearm so the palm faces anteriorly/upward (anatomical position). The radius and ulna are parallel.
- Pronation - Rotation of the forearm so the palm faces posteriorly/downward. The distal end of the radius crosses over the ulna.
The hand articulates predominantly with the radius; thus when the distal radius moves medially over the ulna, the hand pronates. When it returns, the hand supinates.
Plane of Movement
Pronation and supination occur in the transverse (horizontal) plane about a longitudinal axis running from the radial head proximally to the head of the ulna distally. The range of motion is approximately 80-90° of pronation and 80-90° of supination from neutral (mid-position).
Muscles Responsible
Supination
| Muscle | Details |
|---|---|
| Biceps brachii | The largest and most powerful supinator; most effective when the elbow is flexed to 90°. The tendon wraps around the radius when pronated; contraction unwraps it, producing supination. |
| Supinator | Located in the posterior compartment of the forearm; originates from the supinator crest of ulna and lateral epicondyle of humerus. Works at all elbow positions including full extension (when biceps is less effective). |
Pronation
| Muscle | Details |
|---|---|
| Pronator teres | From the medial epicondyle of humerus to the lateral surface of the radius (midshaft). A faster, more forceful pronator. Also assists in elbow flexion. |
| Pronator quadratus | A flat, square muscle between the anterior surfaces of distal radius and ulna. The primary pronator; active in all pronation movements. |
Accessory
- Anconeus - Causes slight abduction of the distal ulna during pronation to maintain the palm over the central axis.
Summary table:
| Movement | Muscles | Plane | Axis |
|---|---|---|---|
| Supination | Biceps brachii, Supinator | Transverse | Longitudinal (radial head to ulnar head) |
| Pronation | Pronator teres, Pronator quadratus | Transverse | Longitudinal (radial head to ulnar head) |
- Gray's Anatomy for Students; General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.