Hydrocephalus pathophysiology,types and management
Reading File
Finding Sources
Searching PubMed
"hydrocephalus"[MeSH Terms] AND management
Searching the Web
hydrocephalus pathophysiology types management 2024 clinical review
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, authoritative content to write a complete answer. Let me compile everything.
Hydrocephalus: Pathophysiology, Types, and Management
Normal CSF Physiology (Foundation)
CSF is produced by the choroid plexus within the ventricles at approximately 500 mL/day (with a total CSF volume of ~150 mL, meaning full turnover occurs ~3x daily). It circulates from the lateral ventricles → third ventricle → cerebral aqueduct (of Sylvius) → fourth ventricle → exits via the foramina of Luschka (lateral, paired) and foramen of Magendie (midline) → subarachnoid space → absorbed primarily through arachnoid granulations into the dural venous sinuses, with additional absorption along the brain parenchyma and spinal cord. Cerebrovascular pulsations also drive net CSF flow. The balance between production and resorption regulates CSF volume precisely.
Definition
Hydrocephalus is an increase in the volume of CSF within the ventricular system due to impaired flow or decreased resorption. It is a pressure-dependent enlargement of the cerebral ventricles. The term literally means "water on the brain" but is clinically a nonspecific term that must be distinguished from ventriculomegaly due to cerebral atrophy (hydrocephalus ex vacuo), which carries different implications entirely.
- Robbins & Kumar Basic Pathology, p. 821
- Bradley and Daroff's Neurology in Clinical Practice, p. 1853
Pathophysiology
The Imbalance Mechanism
Hydrocephalus results from any disturbance in the formation, flow, or absorption of CSF:
- Obstruction to flow - either within the ventricular system (intraventricular) or within the subarachnoid space/arachnoid granulations
- Decreased resorption - impaired arachnoid granulation function (post-hemorrhage, post-infection, venous hypertension)
- Overproduction - rare; can occur with choroid plexus papilloma
Sequence of Events in Acute Hydrocephalus
- Obstruction occurs → CSF continues to be produced despite rising pressure
- 80% of maximal ventricular enlargement occurs within the first 6 hours of onset (acute phase)
- A slower phase of further enlargement follows
- CSF accumulates in the periventricular white matter interstitial space → transependymal edema (periventricular lucency on CT/MRI)
- In the chronic phase, ventricular pressure may normalize due to compensatory drainage, even though structural damage persists
- Long-standing hydrocephalus → white matter atrophy, axonal damage, subependymal gliosis
The image below (CT) shows transependymal flow - contrast diffusing from the ventricle into surrounding periventricular white matter:
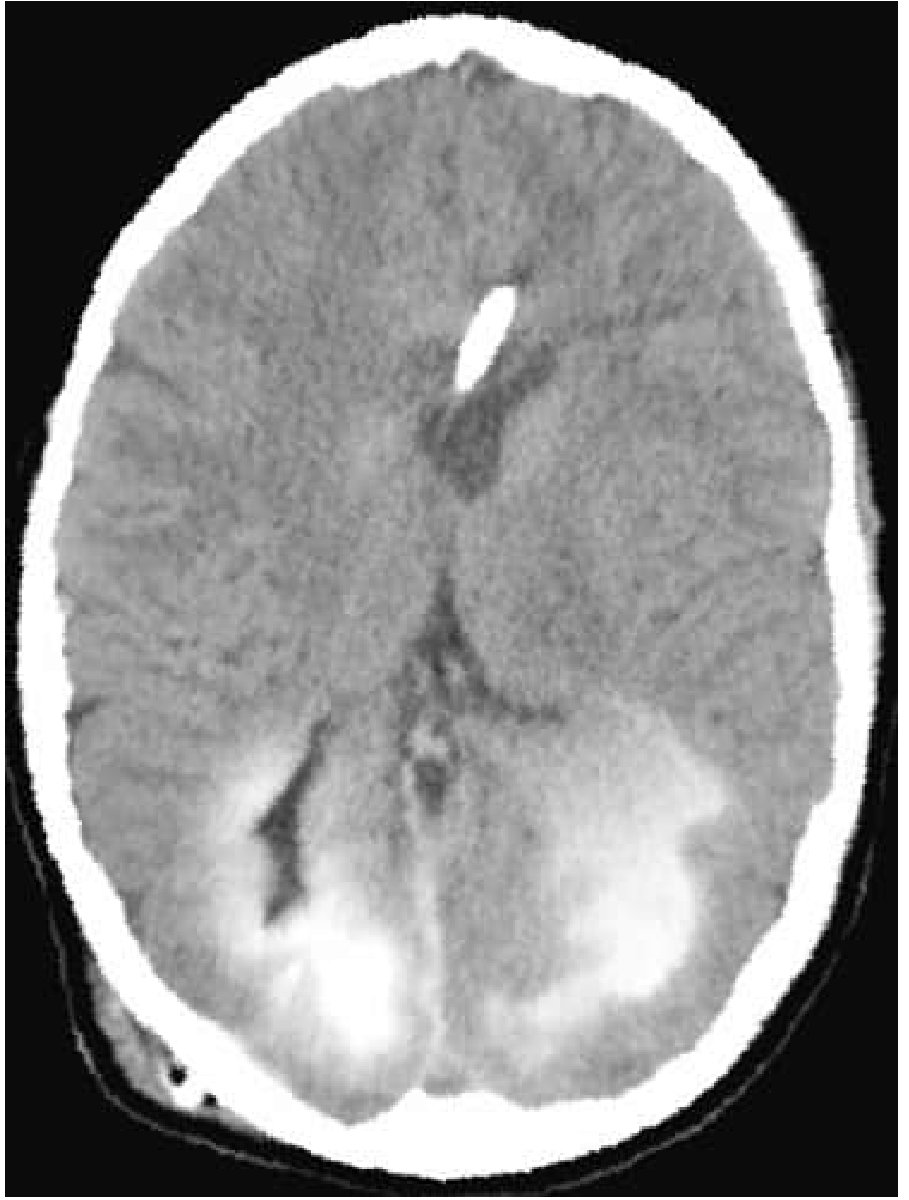
Fig. Transependymal Flow - CT showing contrast infused through a ventricular shunt diffusing into surrounding brain through the ependyma. - Bradley and Daroff's Neurology, p. 1854
And the gross pathology of dilated lateral ventricles:
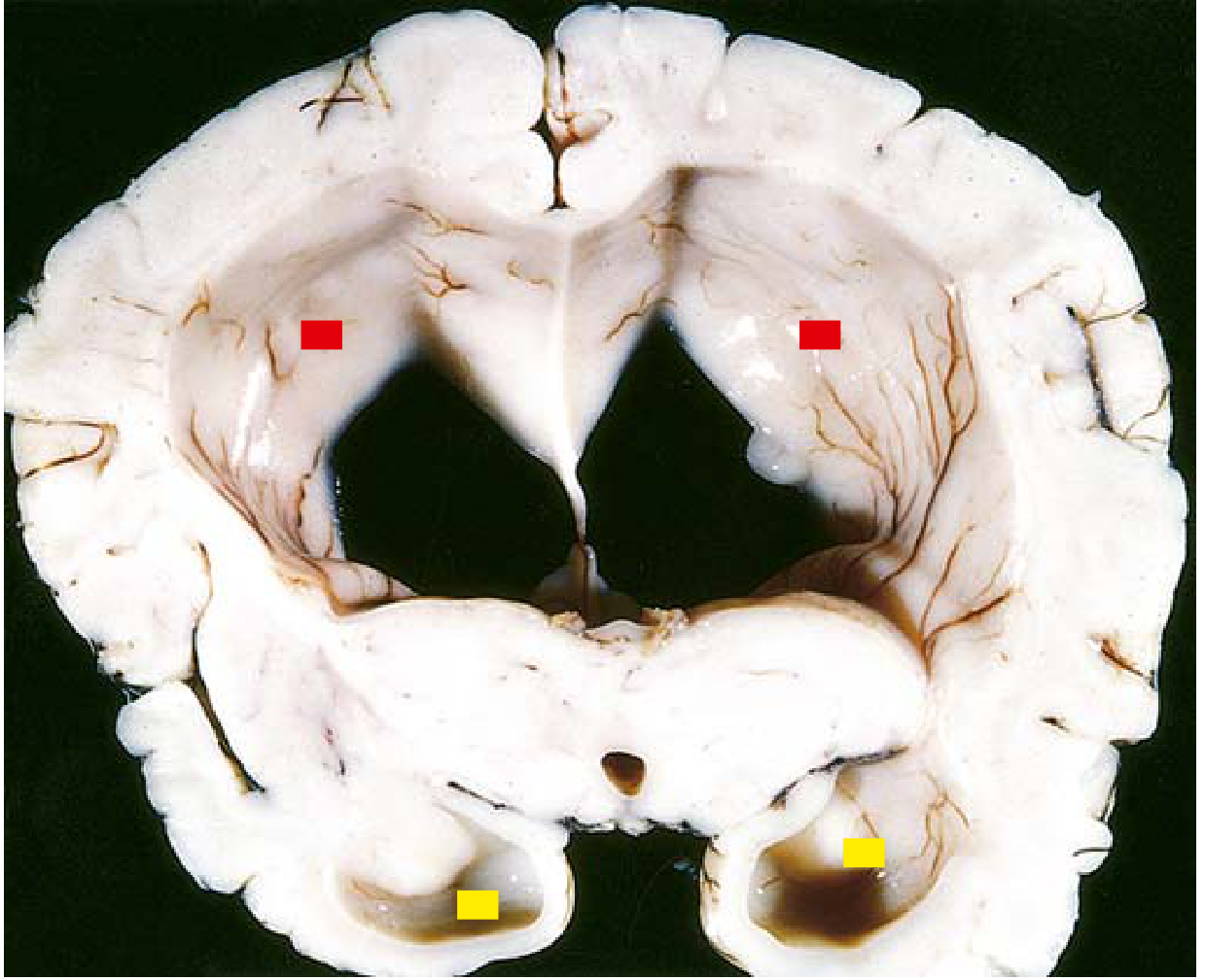
Fig. Hydrocephalus - coronal section at mid-thalamus showing grossly dilated lateral ventricles. - Robbins & Kumar Basic Pathology, p. 821
Classification / Types
1. Non-communicating Hydrocephalus (Obstructive/Intraventricular)
CSF flow is blocked within the ventricular system before reaching the subarachnoid space. Only a portion of the ventricular system dilates (upstream from the obstruction).
Vulnerable narrow points (sites of obstruction):
- Foramen of Monro - colloid cysts, suprasellar tumors, subependymal giant cell astrocytomas (in tuberous sclerosis)
- Cerebral aqueduct (of Sylvius) - most common site; aqueductal stenosis (congenital or post-infectious gliosis), tectal plate gliomas, pineal region tumors, brainstem diffuse astrocytomas
- Fourth ventricular outflow (foramina of Luschka and Magendie) - Dandy-Walker malformation, Chiari II malformation, posterior fossa tumors (medulloblastoma, ependymoma), cerebellar hemorrhage/infarction
Key imaging features:
- Temporal horn dilatation disproportionate to lateral ventricle size
- Anterior and posterior recess enlargement of the third ventricle
- Inferior convexity of the third ventricular floor
- Transependymal edema (periventricular hyperintensity)
- Sulcal spaces, basal cisterns effaced/obliterated
2. Communicating Hydrocephalus (Extraventricular Obstructive)
The entire ventricular system is enlarged; CSF flows freely through the ventricular system but cannot be absorbed adequately. Obstruction is outside the ventricles, at the level of the subarachnoid space or arachnoid granulations.
Causes:
- Post-subarachnoid hemorrhage (blood products impair arachnoid granulation absorption)
- Post-meningitis (infectious scarring - bacterial, TB, fungal, syphilis)
- Leptomeningeal carcinomatosis
- Raised intracranial venous pressure (venous sinus thrombosis, dural AVMs, vein of Galen malformations, craniosynostosis with jugular foramen stenosis)
- Idiopathic (especially in elderly - NPH)
Imaging: Full ventricular dilatation including fourth ventricle; may show variable sulcal effacement or even normal-appearing cortical surfaces.
3. Normal Pressure Hydrocephalus (NPH)
A special form of chronic communicating hydrocephalus, predominantly in the elderly. Represents approximately one-third of adult hydrocephalus presentations.
Classic Triad (Hakim-Adams triad):
- Gait disturbance - apraxic ("magnetic") gait; feet appear stuck to the floor; broad-based; frontal lobe pattern
- Urinary incontinence
- Dementia - subcortical type; psychomotor slowing, apathy, preserved language and spatial function
Pathophysiology of NPH: LP reveals normal or minimally elevated pressure, but long-term ICP monitoring reveals intermittent nocturnal pressure spikes. The "normal pressure" designation refers only to the moment of measurement. Ventricular enlargement compresses periventricular white matter tracts, especially the corticospinal fibers descending around the ventricles (explaining gait disturbance and lower limb predominance) and frontal connections (explaining the apraxia and incontinence).
Secondary NPH occurs after head trauma, SAH, meningitis, or surgery; idiopathic NPH has no identifiable cause.
Diagnosis:
- CT/MRI: enlarged ventricles out of proportion to sulcal atrophy; transependymal edema
- LP tap test (large-volume removal of 30-50 mL CSF): temporary improvement in gait confirms likely shunt responsiveness; a 2025 systematic review (PMID 40045804) highlighted the need to standardize this test
- Continuous ICP monitoring (gold standard)
- Isotope cisternography (reflux of isotope into ventricles, delayed cortical clearance)
4. Hydrocephalus Ex Vacuo
Not true hydrocephalus - ventricular enlargement is compensatory and secondary to loss of brain parenchyma from infarction, neurodegenerative disease, or other causes. ICP is normal; no treatment indicated. CSF volume simply fills the space left by shrinking brain tissue.
5. Congenital / Pediatric Hydrocephalus
Specific causes:
- Aqueductal stenosis - most common cause; can be developmental or acquired (post-IVH, post-infection)
- Chiari II malformation - associated with lumbosacral myelomeningocele; hindbrain herniation kinks the aqueduct
- Dandy-Walker malformation - cystic dilatation of the fourth ventricle, absent or hypoplastic vermis, obstructed foramina
- Post-hemorrhagic (germinal matrix IVH in premature infants <1500 g; ~25% develop progressive ventricular enlargement)
- Post-infective (TORCH infections, neonatal bacterial meningitis)
- Vein of Galen malformation - venous hypertension mechanism
Clinical Features by Age Group
Infants (sutures open, <2 years)
- Progressive macrocephaly (most reliable sign) - head circumference crossing centiles upward
- Frontal bossing, calvarial thinning
- Tense, bulging anterior fontanelle
- Sutural diastasis
- Enlarged scalp veins
- "Sunsetting" eyes - downward deviation of gaze from tectal compression (Parinaud's phenomenon)
- Lateral rectus palsy (CN VI false localizing sign)
- Lower limb spasticity (corticospinal tract stretching)
- Irritability, poor feeding, lethargy
Older Children (sutures fused)
- Early morning headache, nausea, vomiting
- Papilledema
- Diplopia (CN VI palsy)
- Ataxia (posterior fossa mass effect)
- Altered consciousness
- "Cracked pot" sound on skull percussion (McEwen sign)
- Endocrine dysfunction if third ventricle involved (growth failure, DI, amenorrhea)
Adults
- Acute: severe headache, papilledema, diplopia, mental status changes, sudden death (from severe ICP elevation)
- Subacute: progressive symptoms depending on site
- Colloid cyst of third ventricle: positional headaches with drop attacks (ball-valve effect - intermittent acute obstruction of foramen of Monro)
- Cerebellar hemorrhage/infarction: headache, ataxia, progressive drowsiness → acute obstructive hydrocephalus requiring emergency intervention
Imaging
| Modality | Role |
|---|---|
| CT | First-line in acute setting; shows ventricular size, transependymal edema, hemorrhage, calcifications; scout view assesses shunt tubing |
| MRI | Superior for cause identification; aqueduct stenosis (sagittal), flow voids (normal CSF flow), periventricular changes, posterior fossa masses, cerebellar infarction |
| Cranial ultrasound | Neonates; through open fontanelle; bedside monitoring of ventricular size |
| MRI flow studies | Assess ETV patency (large T2 hypointense flow void at surgical defect = patent) |
| Isotope cisternography | Communicating vs. non-communicating; NPH evaluation |
Management
1. Emergency / Acute Measures
- External Ventricular Drain (EVD): First-line for acute hydrocephalus (post-SAH, cerebellar hemorrhage, meningitis); removes CSF and monitors ICP continuously. Many patients requiring EVD will eventually need a permanent shunt.
- Posterior fossa craniectomy: For cerebellar hemorrhage with brainstem compression - decompress mass + restore CSF flow; preceded by EVD catheter placement.
- Medical: Acetazolamide (carbonic anhydrase inhibitor, reduces CSF production) and furosemide used as temporizing measures in premature infants with post-hemorrhagic hydrocephalus; not curative.
2. Ventriculoperitoneal Shunt (VP Shunt) - Most Common Definitive Treatment
A catheter drains CSF from a lateral ventricle to the peritoneal cavity via a one-way pressure-sensitive valve system. Also used:
- Ventriculoatrial (VA) shunt - drains to right atrium; used when peritoneal placement is impossible
- Ventriculopleural shunt - less common; drains to pleural space
VP Shunt Complications:
| Complication | Details |
|---|---|
| Obstruction/malfunction | Most common; ventricular catheter blocked by choroid plexus or glial tissue; presents with recurrence of hydrocephalus symptoms |
| Infection | 1-5% incidence; higher in infants; causes ventriculitis; can lead to devastating parenchymal damage |
| Over-drainage / Slit ventricle syndrome | Overdrainage → collapsed ventricles → raised ICP despite shunt patency; poorly compliant stiff ventricles |
| Shunt fracture/disconnection | Identified on plain X-ray (shunt series); calcification at fracture ends |
| Abdominal complications | Ascites, pseudocyst, peritoneal perforation |
| Shunt revisions | Required as children grow; multiple revisions over lifetime common |
3. Endoscopic Third Ventriculostomy (ETV)
A surgical opening is created in the floor of the third ventricle, allowing CSF to bypass the obstruction and drain into the suprasellar cistern - effectively creating an alternative CSF pathway.
Indications: Non-communicating hydrocephalus (aqueductal stenosis is the ideal indication); also used in posterior fossa tumor-associated hydrocephalus.
Advantages over shunt: No hardware left behind, no ongoing infection risk, no valve maintenance.
ETV patency on MRI: Large T2 hypointense flow void at the stoma site confirms patency.
ETV vs. VP shunt in tuberculosis meningitis hydrocephalus: A 2025 meta-analysis (PMID 40479834) evaluated ETV vs. VP shunt for pediatric TB meningitis hydrocephalus, with findings informing treatment selection in infectious etiologies.
4. NPH-Specific Management
- Large-volume LP tap test (30-50 mL): if gait improves within 24-72 hours, VP shunt placement is likely to benefit the patient. Gait improvement predicts better prognosis than improvement in dementia alone.
- VP shunt is the primary treatment; patients with gait as the dominant presenting feature respond best.
- Optimal CSF pressure setting on the shunt valve requires careful titration to avoid over-drainage.
- A 2025 systematic review on cerebral blood flow and autoregulation in NPH (PMID 41402911) highlights impaired vascular reactivity as part of the NPH mechanism, informing future therapeutic targets.
5. Treatment of Underlying Cause
- Remove obstructing tumor/mass
- Treat meningitis (antibiotics/antifungals)
- Drain hematoma
- Repair vascular malformation
Summary Table
| Feature | Non-Communicating | Communicating | NPH | Ex Vacuo |
|---|---|---|---|---|
| Obstruction site | Within ventricles | Subarachnoid/granulations | Arachnoid granulations | None (brain atrophy) |
| Ventricular involvement | Partial (upstream) | All ventricles | All ventricles | Diffuse |
| ICP | Elevated | Elevated/variable | Normal (transiently elevated) | Normal |
| Treatment | ETV or shunt | Shunt | LP tap test + VP shunt | None |
| Common causes | Aqueductal stenosis, tumors, Chiari | Post-SAH, meningitis, venous HTN | Idiopathic, post-SAH, post-trauma | Alzheimer's, infarction |
Sources: Bradley and Daroff's Neurology in Clinical Practice, pp. 1853-1857 | Robbins & Kumar Basic Pathology, p. 820-821 | Grainger & Allison's Diagnostic Radiology, pp. 2027-2029 | Recent PubMed systematic reviews (PMIDs 41402911, 40045804, 40479834, 40542903)
Anti edema measure for hydrocephalus
Finding Sources
Finding Sources
Searching PubMed
"intracranial pressure" AND "hydrocephalus" AND "medical management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive, authoritative answer. Let me compile it.
Anti-Edema Measures in Hydrocephalus
Conceptual Framework
The intracranial compartment is rigid (Monroe-Kellie doctrine). Total intracranial volume = brain parenchyma + blood + CSF = constant. Reducing any one compartment lowers ICP. In hydrocephalus, the primary excess is CSF, but the resulting raised ICP also generates periventricular (transependymal) interstitial edema and secondary cerebral vasodilatation. Anti-edema treatment targets all three compartments:
- Reduce CSF volume (drainage, reduce production)
- Reduce brain water/edema (osmotherapy, corticosteroids)
- Reduce cerebral blood volume (positioning, hyperventilation - temporary)
Anti-edema measures are temporizing/bridging interventions. Definitive treatment remains surgical (VP shunt or ETV).
1. General / Supportive Measures (First-Line - Immediate)
These should be optimized before any pharmacological agent:
| Measure | Rationale |
|---|---|
| Head elevation 30° | Facilitates jugular venous drainage; reduces intracranial venous pressure and CBV |
| Avoid neck flexion/rotation | Compressing jugular veins raises ICP |
| Avoid hypoxia (SpO₂ >94%) | Hypoxia causes cerebral vasodilation → ↑CBV → ↑ICP |
| Avoid hypercarbia | CO₂ is the most potent cerebral vasodilator |
| Avoid hyperthermia | Fever dramatically raises cerebral metabolic demand and CBF |
| Avoid hyponatremia and hypo-osmolar fluids | Water enters brain down osmotic gradient; use isotonic (normal saline) or hypertonic fluids only; avoid 5% dextrose, 0.45% NaCl, and lactated Ringer in cerebral edema |
| Pain and agitation control | Coughing, straining, dyssynchrony with ventilator all spike ICP; titrated fentanyl (25-50 mcg boluses) is preferred |
- Adams and Victor's Principles of Neurology, 12th Ed., p. 913
2. Osmotic Therapy (Cornerstone of Medical Management)
Mechanism: Creates an osmotic gradient across an intact blood-brain barrier (BBB), drawing water from brain interstitium into the bloodstream, reducing brain volume and ICP. Additionally improves blood rheology and cerebral microcirculation by reducing blood viscosity.
A. Mannitol
- Dose: 0.25–1.0 g/kg IV as a 20% solution, every 3–6 hours
- Target: Serum osmolality 290–315 mOsm/L; serum sodium >142 mEq/L
- Ceiling: Do NOT exceed serum osmolality of 320 mOsm/kg (above this, efficacy falls and renal failure risk rises)
- Mechanism: Multiple actions - osmotic dehydration of brain, reduces CSF production, improves CBF by reducing blood viscosity
- Onset: Rapid; also has an immediate rheologic effect on blood viscosity before the osmotic effect is established
- Duration: 2-6 hours per dose
- Side effects:
- Diuresis → hypovolemia, hypokalemia, hypernatremia
- Renal failure (rare; mainly with >200 g/day; almost always reversible)
- Rebound edema if discontinued abruptly (small-molecule diuretics like urea cause rebound; mannitol causes less, but still possible)
- Hyperglycemic hyperosmolar state in diabetics
- Preferred when: Patient is fluid-overloaded or euvolemic; large-molecule, does not expand vascular volume
B. Hypertonic Saline (HTS)
- Formulations and doses:
- 3% NaCl: bolus 150 mL, or continuous infusion 30–50 mL/hr
- 7.5% NaCl: 75 mL boluses
- 23.4% NaCl: 30 mL boluses (requires central venous access for all concentrations >3%)
- Target: Serum sodium up to 160 mEq/L (upper limit)
- Mechanism: Directly raises serum sodium and osmolality; expands intravascular volume (unlike mannitol, which diureses)
- Advantages over mannitol: No diuresis; can be used as a resuscitation fluid simultaneously; avoids hypovolemia; at least as effective as mannitol
- Disadvantages: Can cause volume overload/pulmonary edema in poor cardiac function; risk of osmotic demyelination if sodium correction too rapid; requires central line for concentrated formulations
- Preferred when: Patient is hypovolemic, hypotensive, or requires fluid resuscitation; also when mannitol has caused excessive diuresis
"Several small series comparing the agents have shown too little difference to allow a choice between the two agents. Local experience and an overall assessment of side effects typically dominate practice." - Adams and Victor's Principles of Neurology, p. 913-914
3. Reduction of CSF Production
Acetazolamide (Carbonic Anhydrase Inhibitor)
- Mechanism: Inhibits carbonic anhydrase in the choroid plexus → reduces Na⁺/H⁺ exchange → reduces CSF secretion by ~50%
- Use: Primary medical treatment for slowly progressive hydrocephalus and as a bridge to surgery; also used in idiopathic intracranial hypertension (pseudotumor cerebri)
- Dose (adults): 250 mg–1 g orally 2–4 times daily (typically up to 2 g/day)
- Dose (pediatric/neonates): Used combined with furosemide for post-hemorrhagic hydrocephalus in premature infants
- Limitations: "Of marginal benefit" as a standalone agent; does not address the obstruction; not suitable for acute presentations
- Side effects: Metabolic acidosis, hypokalemia, paresthesias, nephrolithiasis, sulfa allergy cross-reactivity
Furosemide (Loop Diuretic)
- Mechanism: Inhibits Na-K-2Cl cotransporter in choroid plexus; also independent systemic diuresis reduces brain interstitial water
- Use: Used in combination with acetazolamide (synergistic); especially in neonatal/pediatric progressive hydrocephalus as a temporizing measure
- Limitation: Not definitive; primarily a bridge to surgical management
"Acetazolamide and furosemide may provide temporary relief by decreasing the rate of CSF production [in slowly progressive hydrocephalus]." - The Harriet Lane Handbook, 23rd Ed., p. 731
4. Reduction of Cerebral Blood Volume
Controlled Hyperventilation
-
Mechanism: Lowering PaCO₂ → CSF alkalosis → cerebral vasoconstriction → ↓cerebral blood volume → ↓ICP
-
Target: PaCO₂ 30–35 mmHg (mild hyperventilation); avoid <25 mmHg
-
Onset: Rapid (minutes); effect lasts only 20–40 minutes - pH equilibrates as choroid plexus generates ammonium buffers
-
Use: Emergency bridge only - acute herniation, acute ICP spike, while surgical intervention is being prepared
-
Caution: Excessive hyperventilation can cause cerebral ischemia (vasoconstriction reduces perfusion); particularly dangerous in children - even modest hypocarbia (PCO₂ <25 mmHg) shows ischemic changes in 75% of pediatric patients
-
NOT for chronic use - loss of effect, risk of ischemia
-
Adams and Victor's Principles of Neurology, p. 914
-
Bradley and Daroff's Neurology in Clinical Practice, p. 1851
5. Corticosteroids
- Mechanism: Reduce vasogenic edema by stabilizing and restoring the blood-brain barrier permeability; reduce release of vasogenic cytokines
- Dexamethasone is the agent of choice (best CNS penetration, minimal mineralocorticoid effect)
- Standard dose: 4–10 mg IV loading, then 4 mg every 6 hours
- High-dose: up to 100 mg/day in severe cases
When corticosteroids ARE indicated in hydrocephalus context:
- Peritumoral vasogenic edema (brain tumors, metastases) - dramatic and rapid response; reduces edema around tumor causing the obstruction
- Inflammatory/demyelinating causes (MS lesions blocking CSF pathways) - high-dose methylprednisolone 1 g/day x 3–5 days
- Bacterial meningitis - dexamethasone reduces neuroinflammation and risk of post-meningitic communicating hydrocephalus (adjunct to antibiotics)
- Spinal cord edema post-surgically
When corticosteroids are NOT indicated / contraindicated:
- Traumatic brain injury - the CRASH trial (>10,000 patients) showed methylprednisolone significantly increased mortality vs. placebo; absolutely contraindicated
- Cytotoxic edema (ischemic stroke, intracerebral hemorrhage) - no benefit; systemic complications worsen outcome
- Pure obstructive hydrocephalus without vasogenic edema - no direct benefit; may mask signs of infection
"Corticosteroids lower ICP primarily in vasogenic edema... they have been less effective in cytotoxic edema, and are contraindicated in the treatment of edema secondary to stroke or hemorrhage." - Bradley and Daroff's Neurology in Clinical Practice, p. 1852
6. Sedation and Analgesia for ICP Control
-
Propofol: First-choice IV sedative in ICU; decreases cerebral metabolic rate, oxygen demand, and CBF; rapidly clears for neurologic assessment; watch for hypotension
-
Dexmedetomidine: Alternative; preserves neurologic exam; risk of hypotension and bradycardia; does not suppress respiratory drive
-
Barbiturate coma (pentobarbital):
- Loading dose: 10 mg/kg IV over 30 minutes
- Maintenance: 1–4 mg/kg/hour, titrated to EEG burst suppression
- Reserved for refractory ICP (>40 mmHg) unresponsive to all other measures
- Major drawback: hypotension requiring vasopressors; significantly reduces cerebral perfusion pressure
- Evidence shows no overall outcome benefit; used only as last resort before decompressive craniectomy
-
Rosen's Emergency Medicine, p. 70
7. Hypothermia
- Mechanism: Reduces cerebral metabolic demand and CBF
- Target temperature: 32–34°C
- Current evidence: Multiple RCTs (DECRA, RESCUEicp, Clifton, Andrews) have failed to show improved outcomes. Major problem: rebound ICP surge on rewarming. Not routinely recommended; may be used in very selected cases with refractory ICP.
8. Decompressive Craniectomy
- The surgical last resort for medically refractory intracranial hypertension
- Removes a large bone flap to allow brain to expand without herniation
- ICP monitoring is required to trigger this decision (persistent ICP >25 mmHg despite all medical measures)
- Evidence from RESCUEicp trial: reduces mortality but increases survivors with severe disability
Step-Wise Protocol Summary
STEP 1 (Immediate - all patients)
→ Head 30° elevation, correct hypoxia, hypercarbia, fever
→ Isotonic/hypertonic fluids ONLY; avoid hypotonic solutions
→ Adequate analgesia/sedation (propofol + fentanyl)
STEP 2 (Pharmacological)
→ Acute/symptomatic: Mannitol 0.25-1 g/kg IV or HTS bolus
→ Subacute/progressive: Acetazolamide ± furosemide (reduces CSF production)
→ Vasogenic edema (tumor/inflammation): Dexamethasone 4-10 mg IV
→ Emergency bridge: Controlled hyperventilation PaCO₂ 30-35 mmHg
STEP 3 (Refractory ICP)
→ Barbiturate coma (pentobarbital)
→ Therapeutic hypothermia (selected cases)
STEP 4 (Definitive)
→ CSF drainage: EVD, VP shunt, or ETV
→ Decompressive craniectomy (last resort)
Key Distinctions by Edema Type
| Edema Type | Mechanism | Best Treatment |
|---|---|---|
| Interstitial (transependymal) | CSF forcing through ependyma into white matter | Relieve obstruction (EVD/shunt); osmotherapy |
| Vasogenic (peritumoral/inflammatory) | Disrupted BBB, protein-rich fluid | Dexamethasone; mannitol |
| Cytotoxic (ischemia) | Na-K-ATPase failure, cellular swelling | HTS/mannitol (limited); NO steroids |
| Osmotic | Hyponatremia/rapid correction | Hypertonic saline; correct sodium carefully |
Sources: Adams and Victor's Principles of Neurology, 12th Ed., pp. 912-917 | Bradley and Daroff's Neurology in Clinical Practice, pp. 1851-1852 | Rosen's Emergency Medicine, pp. 70-71 | The Harriet Lane Handbook, 23rd Ed., p. 731
This is a shared conversation. Sign in to Orris to start your own chat.