Acute pyelonephritis
Reading File
Finding Sources
Searching PubMed
"pyelonephritis" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a thorough, textbook-grounded overview of acute pyelonephritis.
Acute Pyelonephritis
Definition
Acute pyelonephritis is suppurative (purulent) inflammation of the kidney and renal pelvis caused by bacterial infection. It is an upper urinary tract infection (UTI), distinct from lower tract infections (cystitis, urethritis, prostatitis), though it commonly arises as a complication of them.
- Robbins & Kumar Basic Pathology
Pathogenesis & Routes of Infection
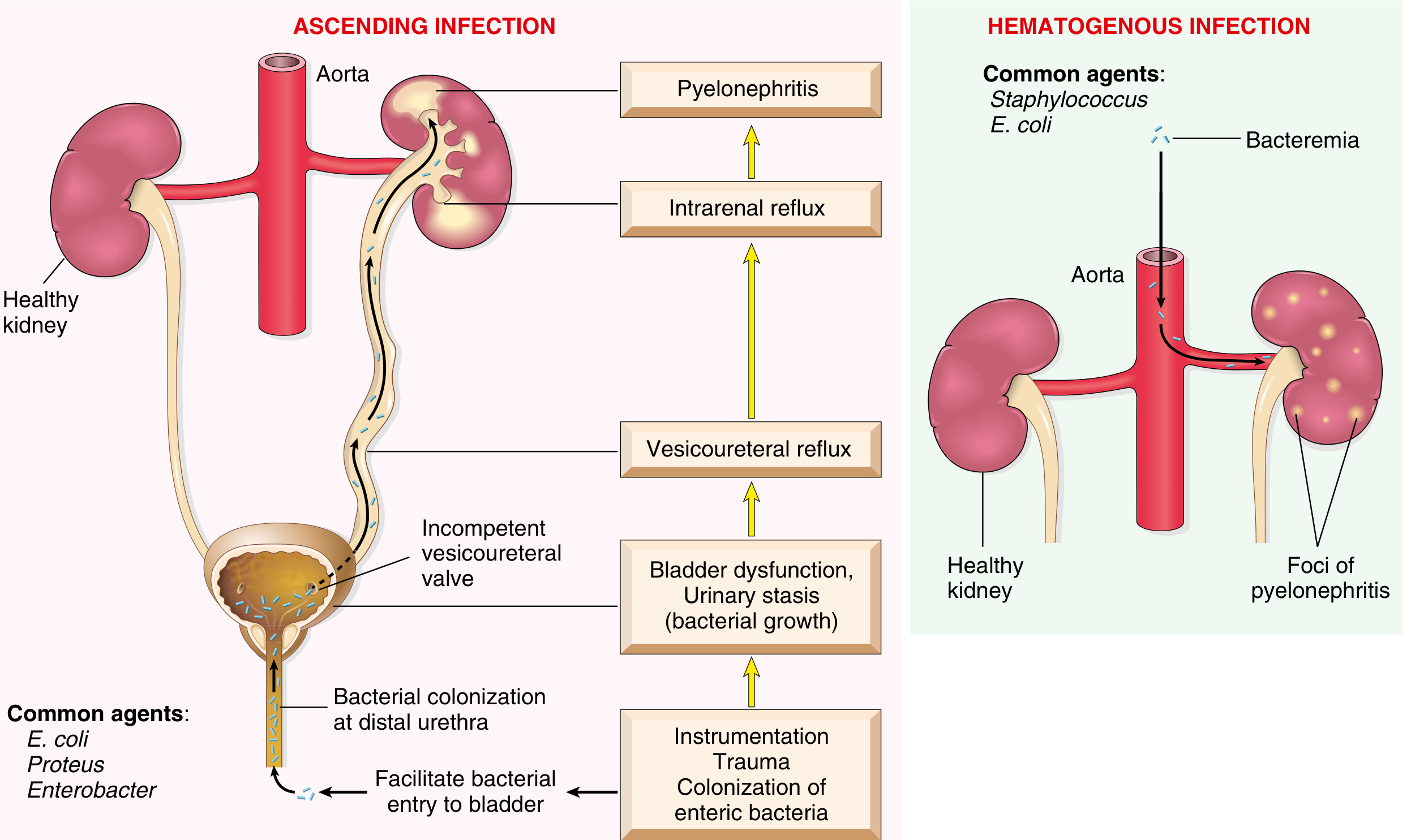
Two routes:
1. Ascending infection (most common):
- Enteric bacteria colonize the distal urethra and perineum
- Bacteria ascend to the bladder (facilitated by instrumentation, catheterization, or sexual intercourse)
- An incompetent vesicoureteral valve allows reflux up the ureter
- Intrarenal reflux then seeds the renal parenchyma
- Women are disproportionately affected due to the short urethra and proximity of the urethral meatus to the rectum
2. Hematogenous (less common):
-
Secondary to bacteremia, sepsis, or endocarditis
-
Common agents: Staphylococcus, E. coli
-
Produces multifocal cortical abscesses
-
Robbins & Kumar Basic Pathology; Campbell Walsh Wein Urology
Predisposing Factors
| Factor | Mechanism |
|---|---|
| Urinary tract obstruction (BPH, stones, uterine prolapse) | Urine stasis, bacterial overgrowth |
| Vesicoureteral reflux (VUR) | Congenital or acquired; present in 20-40% of children with UTI |
| Diabetes mellitus | Immune suppression + neurogenic bladder |
| Pregnancy | Ureteral compression by gravid uterus, progesterone-induced relaxation |
| Catheterization / instrumentation | Direct bacterial inoculation |
| Immunosuppression | Impaired bacterial clearance |
| Spinal cord injury / neurogenic bladder | Urinary stasis |
Microbiology
- E. coli - by far the most common (~80%), possesses special virulence factors (P pili, K antigens, endotoxin, type 1 fimbriae)
- Proteus, Klebsiella, Enterobacter, Pseudomonas - in complicated cases, recurrent UTIs, hospitalized patients, catheterized patients
- Enterococcus faecalis, S. epidermidis, S. aureus - gram-positives (less common)
Note: About 20% of patients have urine cultures with <10^5 CFU/mL (i.e., a "negative" culture by traditional thresholds).
- Campbell Walsh Wein Urology
Morphology (Pathology)
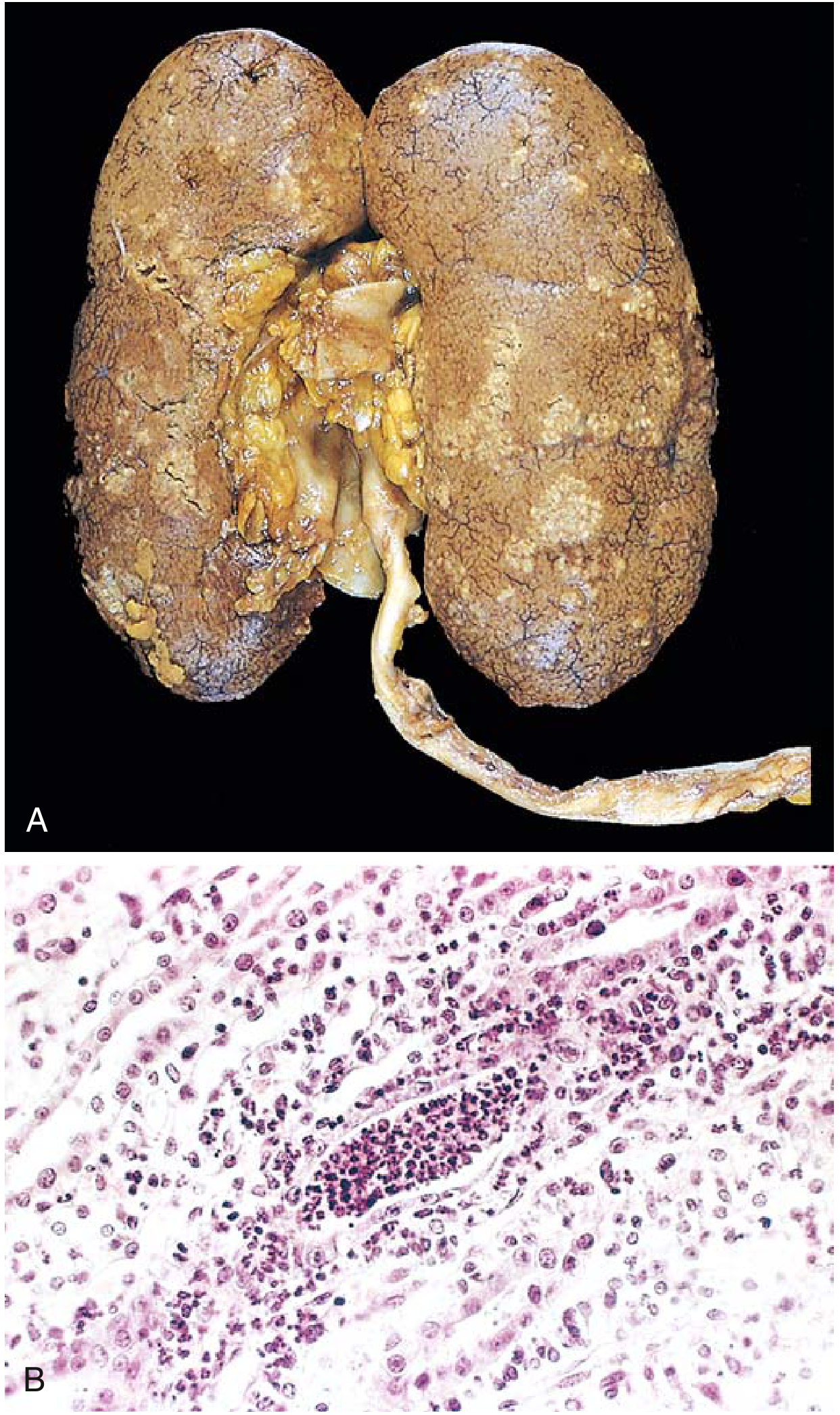
Gross: The kidney may be normal sized or enlarged, with discrete yellowish raised abscesses on the cortical surface.
Microscopic: Neutrophil-rich inflammation initially confined to tubules, then spreading to the interstitium. Neutrophils extending into collecting ducts form WBC casts in urine. Glomeruli are typically spared.
Complications of severe disease:
-
Pyonephrosis - when obstruction prevents pus drainage, filling the renal pelvis and calyces
-
Perinephric abscess - extension through the renal capsule into perinephric fat
-
Papillary necrosis - ischemic/suppurative necrosis of papillae; seen in diabetics, patients with urinary obstruction, and sickle cell anemia
-
Robbins & Kumar Basic Pathology
Clinical Presentation
- Classic triad: Abrupt onset of fever (≥38.0°C/100.3°F), chills, and unilateral or bilateral flank pain / costovertebral angle (CVA) tenderness
- Lower urinary tract symptoms (dysuria, frequency, urgency) may or may not be present
- Nausea, vomiting, and diarrhea can simulate a GI presentation
- Asymptomatic progression is possible, especially in immunocompromised patients
- Acute renal failure is rare but can occur
Note: PID is frequently misdiagnosed as acute pyelonephritis. A pelvic exam is warranted when STI risk factors are present.
- Campbell Walsh Wein Urology; Textbook of Family Medicine 9e
Diagnosis
Urinalysis
- Pyuria - numerous WBCs, often in clumps
- WBC casts - nearly pathognomonic when combined with fever and flank pain
- Bacteriuria (rods or cocci chains on microscopy)
- Mild proteinuria and hematuria are common
Urine Culture
- Always obtain before starting antibiotics
- Guides therapy if initial empiric treatment fails
- Nitrite dipstick lacks sensitivity and does not identify the organism
Blood Tests
- Leukocytosis with neutrophilia
- Elevated CRP and ESR
- Elevated creatinine if renal failure is present
Blood Cultures
- Positive in ~25% of cases
- Not routinely required for uncomplicated pyelonephritis in women
- Should be obtained in: men, pregnant women, those with systemic toxicity, hospitalized patients
Imaging
-
Ultrasound - focal parenchymal swelling, increased or decreased echogenicity; useful to exclude obstruction/stones
-
CT (contrast) - gold standard for complicated cases; shows focal swelling with diminished, inhomogeneous contrast enhancement; can detect abscesses, gas, and obstruction
-
MRI - focal swelling and restricted diffusion on DWI
-
Campbell Walsh Wein Urology
Management
Classification for Management
| Category | Features |
|---|---|
| Uncomplicated outpatient | Normal urinary tract, tolerating PO, no sepsis |
| Uncomplicated inpatient | Normal urinary tract, too ill for outpatient (high fever, vomiting, dehydration, sepsis) |
| Complicated | Hospitalized, catheterized, post-urologic surgery, structural abnormalities |
Antibiotic Regimens (per IDSA / Campbell Walsh Wein)
Outpatient (oral):
| Drug | Dose | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg q12h | 7 days |
| Ciprofloxacin XR | 1000 mg q24h | 7 days |
| Levofloxacin | 750 mg q24h | 5 days |
| TMP-SMX DS | 160/800 mg q12h | 14 days (only if susceptibility known) |
- Fluoroquinolones: first-line only if local resistance is <10%
- TMP-SMX: use only if the causative organism is known susceptible; otherwise, precede with one-time IV ceftriaxone 1 g
Inpatient (parenteral):
| Drug | Notes |
|---|---|
| Fluoroquinolone IV | First-line if susceptible |
| Ceftriaxone 1 g IV q24h | Broad coverage |
| Aminoglycoside ± ampicillin | Good Gram-negative coverage |
| Carbapenem | For resistant organisms, ESBL producers |
| Ampicillin/sulbactam ± aminoglycoside | If Gram-positive cocci suspected |
- Transition to oral therapy once afebrile and clinically stable
- Total duration: 10-14 days for hospitalized patients
In pregnancy:
- Parenteral: ampicillin + gentamicin, or aztreonam
- Oral: cephalexin 500 mg q6h for 10-14 days (fluoroquinolones and TMP-SMX avoided in pregnancy)
Indications for Hospitalization
- Severe sepsis
- Inability to tolerate oral fluids/medications
- Diagnostic uncertainty
- Failure to improve on outpatient therapy within 48-72 hours
- Pregnancy with significant illness
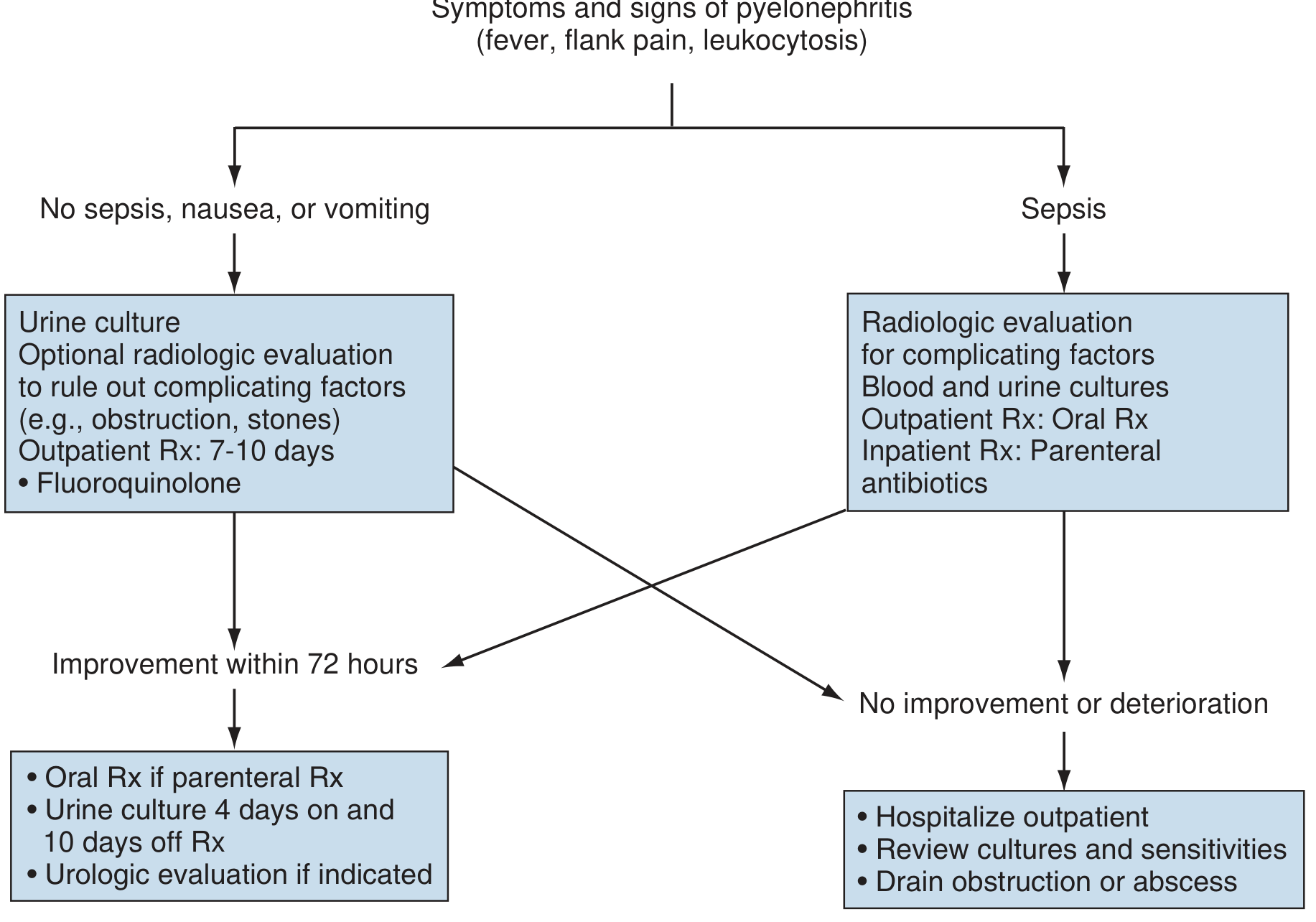
Subsequent / Follow-up Management
- Even with successful treatment, fever and flank pain may persist for several days
- Urine culture: repeat 4 days on therapy, and 10 days after completing antibiotics
- If no improvement within 72 hours: re-culture, adjust antibiotics, obtain imaging (CT preferred)
- If obstruction or abscess found: drainage via ureteral stent or percutaneous nephrostomy
Differential Diagnosis
- Acute appendicitis (right-sided; normal urinalysis)
- Acute diverticulitis
- Pancreatitis
- Ovarian pathology / PID
- Herpes zoster (dermatomal pain without urinary symptoms)
- Renal colic (colicky pain, hematuria, no fever typically)
Complications
- Renal abscess / perinephric abscess
- Pyonephrosis (obstructed infected kidney)
- Papillary necrosis (diabetics, sickle cell, obstruction)
- Gram-negative sepsis / septic shock
- Chronic pyelonephritis and renal scarring (especially with VUR in children)
- Acute kidney injury (rare; more common with bilateral involvement or solitary kidney)
Special Populations
- Children: VUR is the major predisposing factor; renal scarring (reflux nephropathy) is a key long-term concern
- Pregnant women: Carries risk of preterm labor and maternal sepsis; all cases warrant hospitalization
- Diabetics: Higher risk of emphysematous pyelonephritis, fungal infection, and papillary necrosis
- Immunocompromised: May present atypically or asymptomatically; higher risk of complicated course
Recent evidence note: A 2024 systematic review (PMID 38339768) examined the utility of ultrasound in acute pyelonephritis, reinforcing its value as an initial imaging modality for detecting complications. A 2025 meta-analysis (PMID 39885375) raised awareness of SGLT2 inhibitors as a risk factor for severe UTIs, relevant when managing pyelonephritis in diabetic patients on these agents.
Sources: Robbins & Kumar Basic Pathology; Campbell Walsh Wein Urology (3-Vol Set); Textbook of Family Medicine 9e; Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.