
b4c34863-3113-4cf8-ab6b-ff7efd00b52e.jpeg
2 3 4
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I now have sufficient information from the textbooks. Let me compile the complete answers.
Here are the answers to Questions 2, 3, and 4:
Question 2: Effect of Sympathetic and Parasympathetic Nervous System on Pacemaker Potentials
The SA node is the natural pacemaker of the heart and is under dual autonomic control, with a baseline preponderance of parasympathetic tone.
Pacemaker potential recap:
SA nodal cells undergo spontaneous phase 4 (slow diastolic depolarization). When this reaches threshold, an action potential fires. The upstroke (phase 0) is slow, mediated by Ca²⁺ current (not Na⁺ as in ventricular cells). This gives a resting intrinsic rate of ~100 beats/min.
Sympathetic stimulation (norepinephrine/β₁-adrenoceptors):
- Increases the slope of phase 4 depolarization - threshold is reached faster
- Result: increased heart rate (positive chronotropy)
- Also increases contractility (positive inotropy) and conduction velocity (positive dromotropy)
- In denervated hearts (no parasympathetic tone), the natural intrinsic rate is ~100 bpm
Parasympathetic stimulation (acetylcholine/muscarinic M2 receptors):
- Opens K⁺ channels (IKACh) - hyperpolarizes the cell
- Decreases the slope of phase 4 depolarization - takes longer to reach threshold
- Also decreases the funny current (If)
- Result: decreased heart rate (negative chronotropy)
- At baseline, parasympathetic dominance keeps resting HR at 60-100 bpm (below the intrinsic 100 bpm)
"Removal of parasympathetic tone or an increase in sympathetic innervation leads to an increase in rate of depolarization." - Harrison's Principles of Internal Medicine 22E
Question 3: Frank-Starling's Law - Definition and Clinical Importance
Definition:
Frank-Starling's law states that "the energy of contraction is proportional to the initial length of the cardiac muscle fiber." In practical terms: the greater the end-diastolic volume (preload/stretch), the greater the stroke volume, up to a physiological limit.
- The relationship between ventricular stroke volume and end-diastolic volume is called the Frank-Starling curve
- When regulated by changes in fiber length, this is called heterometric regulation
- In the heart, the preload = end-diastolic volume (EDV); afterload = resistance against which blood is expelled
"Starling pointed this out when he stated that the 'energy of contraction is proportional to the initial length of the cardiac muscle fiber'" - Ganong's Review of Medical Physiology, 26th Ed.
Clinical Importance:
- Cardiac compensation in heart failure: When the ventricle dilates (increased EDV), the heart initially maintains stroke volume by using the Frank-Starling mechanism - the basis of compensated heart failure
- Matching output of left and right ventricles: If the right ventricle pumps more, more blood returns to the left, increasing its preload and thus automatically increasing its output to match
- Response to exercise: Increased venous return during exercise stretches the ventricle, boosting cardiac output
- Basis of preload optimization in ICU: Volume resuscitation targets optimizing the preload on the Frank-Starling curve
- Valvular disease: In aortic or mitral regurgitation, ventricular dilation uses this mechanism for compensation until the heart decompensates (moves down the descending limb of the curve)
Question 4: Significance of Long Refractory Period in Cardiac Muscle - Why Cardiac Muscle Cannot Be Tetanised
The long refractory period explained:
- During phases 0 to 2 and approximately half of phase 3 (until membrane potential reaches ~-50 mV during repolarization), cardiac muscle is in its absolute refractory period - it cannot be excited again regardless of stimulus strength
- It remains in the relative refractory period until phase 4
- This refractory period lasts nearly as long as the entire contraction (~200-250 ms), in contrast to skeletal muscle where the refractory period (~1-2 ms) is far shorter than the twitch duration
Why cardiac muscle cannot be tetanised:
In skeletal muscle, because the refractory period is much shorter than the twitch, repeated rapid stimuli can summate and produce sustained tetanic contraction. In cardiac muscle, by the time the refractory period is over, the contraction is almost finished - so a new stimulus cannot summate with the ongoing contraction to produce tetanus.
"During phases 0 to 2 and about half of phase 3, cardiac muscle cannot be excited again; that is, it is in its absolute refractory period. It remains relatively refractory until phase 4. Therefore, tetanus of the type seen in skeletal muscle cannot occur." - Ganong's Review of Medical Physiology, 26th Ed.
Physiological/Clinical Significance of this property:
- Prevents tetanic cardiac arrest: If the heart could tetanize, it would remain in sustained contraction with no relaxation phase - making ventricular filling impossible and causing immediate death
- Ensures rhythmic pumping: The long refractory period guarantees alternating contraction and relaxation, which is essential for filling (diastole) and ejection (systole)
- Basis of the "vulnerable period": Near the end of the relative refractory period (corresponds to the peak of the T wave on ECG), a stimulus can trigger a premature beat. This is the "R-on-T phenomenon" - delivering a shock during this window can precipitate ventricular fibrillation
- Explains why antiarrhythmics work by modifying refractory periods: Class Ia, Ic, and III drugs prolong the effective refractory period to terminate re-entrant arrhythmias
"Of course, tetanization of cardiac muscle for any length of time would have lethal consequences." - Ganong's Review of Medical Physiology, 26th Ed.
Describe regulations of co as heterometric and homometric
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough, exam-ready explanation:
Regulation of Cardiac Output: Heterometric vs. Homometric
CO = Heart Rate × Stroke Volume. Stroke volume is regulated by two broad mechanisms:
1. Heterometric Regulation (Starling's Mechanism)
"Hetero" = different length - regulation that works by changing the resting length of cardiac muscle fibers before they contract.
Basis
When venous return increases, the ventricle fills more - end-diastolic volume (EDV) rises - the muscle fibers are stretched to a greater initial length. According to the Frank-Starling law, this increased stretch produces a more forceful contraction, generating a larger stroke volume.
"When cardiac output is regulated by changes in cardiac muscle fiber length, this is referred to as heterometric regulation." - Ganong's Review of Medical Physiology, 26th Ed.
Mechanism (molecular)
At optimal sarcomere length, there is maximal overlap between actin and myosin filaments, allowing maximum cross-bridge formation. More stretch → more optimal overlap → greater tension developed.
The Length-Tension Curve
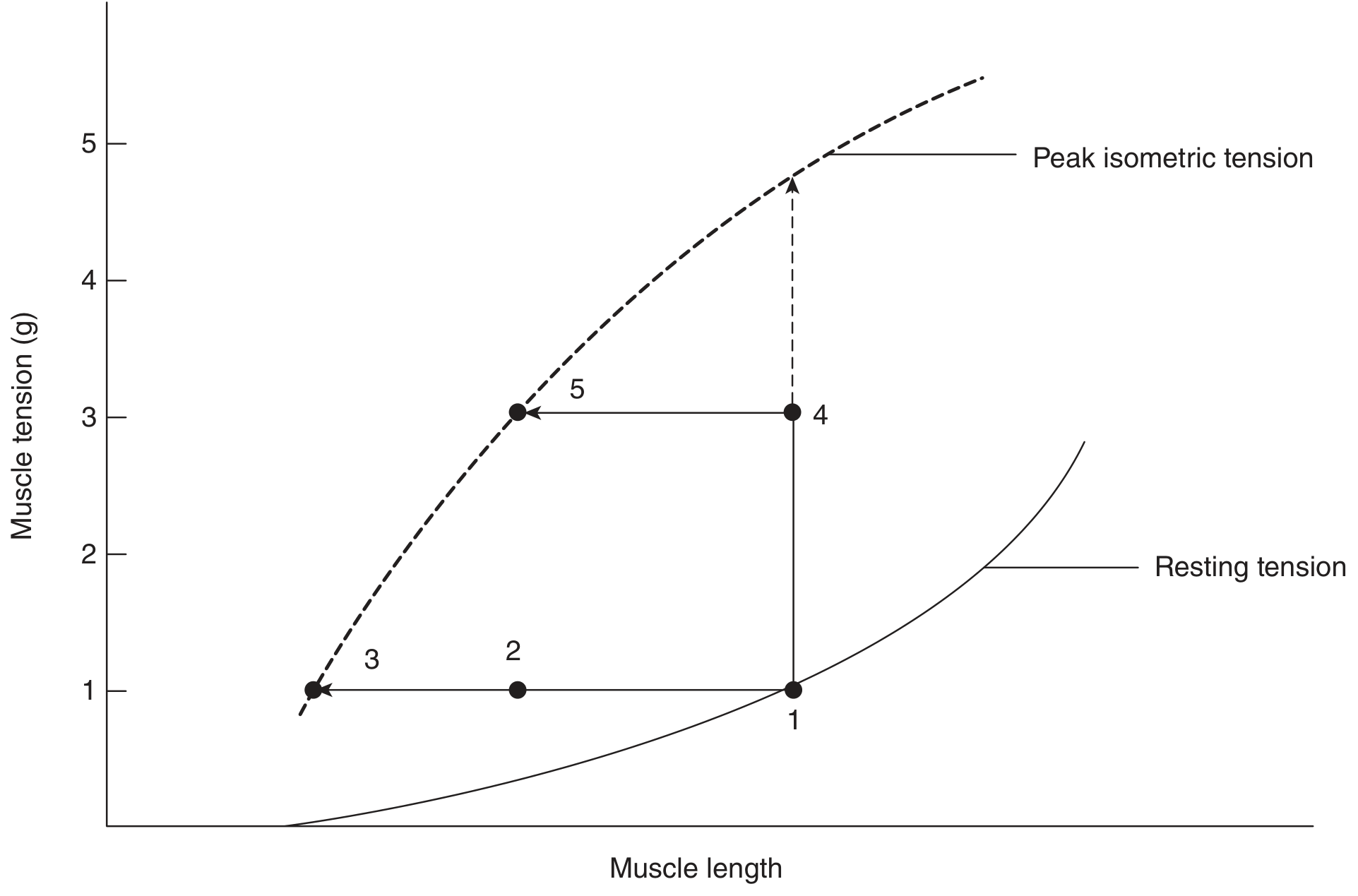
The dashed curve shows peak isometric tension rising as muscle length increases. The heart normally operates on the ascending limb of this curve (points 1-4), so any increase in EDV increases stroke volume.
Key features
| Parameter | Effect |
|---|---|
| Preload (EDV) increases | Stroke volume increases |
| Preload decreases | Stroke volume decreases |
| Contractility | Unchanged |
| Heart rate | Unchanged |
Physiological examples
- Exercise: Increased venous return stretches the ventricle → greater SV
- Lying down: More venous return than standing → SV increases
- Balancing RV and LV output: If RV pumps more, LV receives more → LV stretches more → LV automatically pumps more to match
Clinical relevance
- Basis of compensated heart failure - dilated ventricle uses this mechanism to maintain CO temporarily
- Basis of fluid challenge/volume resuscitation in ICU - we are trying to move the patient up their Frank-Starling curve
- When the heart overdilates (beyond optimal length), the mechanism fails - this is decompensated heart failure (descending limb of the curve)
2. Homometric Regulation
"Homo" = same length - regulation that alters contractility without any change in initial fiber length (resting length stays the same; the muscle simply contracts more or less forcefully from the same starting point).
"Regulation due to changes in contractility independent of length is sometimes called homometric regulation." - Ganong's Review of Medical Physiology, 26th Ed.
Mechanism
The whole length-tension curve shifts upward and to the left (sympathetic stimulation) or downward and to the right (vagal stimulation/heart failure) - meaning at any given fiber length, the muscle generates more or less force than before.
Key features
| Parameter | Effect |
|---|---|
| Fiber length (preload/EDV) | Unchanged |
| Contractility (inotropy) | Changed |
| Stroke volume | Changed due to altered contractility |
Factors that increase contractility (positive inotropes - upward curve shift)
- Sympathetic stimulation / catecholamines (norepinephrine, epinephrine) - act via β₁ receptors → ↑ cAMP → ↑ intracellular Ca²⁺ → stronger contraction
- Digitalis / cardiac glycosides - inhibit Na⁺/K⁺ ATPase → ↑ intracellular Na⁺ → ↓ Na⁺/Ca²⁺ exchanger activity → ↑ intracellular Ca²⁺
- Xanthines (caffeine, theophylline) - inhibit phosphodiesterase → ↑ cAMP
- Increased heart rate (Bowditch/Treppe effect) - more Ca²⁺ accumulates intracellularly with faster rates
- Post-extrasystolic potentiation - the contraction following an ectopic beat is stronger (due to increased Ca²⁺ availability); this is independent of ventricular filling
Factors that decrease contractility (negative inotropes - downward curve shift)
- Vagal stimulation - negative inotropic effect on atrial and (to a lesser extent) ventricular muscle
- Heart disease / myocardial infarction - loss of contractile tissue
- Beta-blockers, calcium channel blockers
- Hypoxia, acidosis
Comparison Summary
| Feature | Heterometric | Homometric |
|---|---|---|
| Alternate name | Starling's mechanism / Frank-Starling | Bowditch effect / Treppe (for rate-dependent); autonomic regulation |
| What changes | Initial fiber length (preload/EDV) | Contractility (inotropy) |
| Fiber length | Changes | Does NOT change |
| Mechanism | Actin-myosin overlap optimization | Ca²⁺ availability / signaling |
| Key mediators | Venous return, blood volume, posture | Sympathetic NS, drugs, heart rate |
| Frank-Starling curve | Movement along the curve | Shift of the entire curve |
| Clinical use | Volume resuscitation, preload optimization | Inotropes in heart failure, β-blockers |
In short: Heterometric regulation adjusts CO by changing how much the heart is filled (preload = fiber length). Homometric regulation adjusts CO by changing how vigorously the heart squeezes from that same starting point (contractility), independent of filling.
This is a shared conversation. Sign in to Orris to start your own chat.