Diuretics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Diuretics drug pharmacology topic samjhao
I have all the content from the previous research. Let me now give you a comprehensive explanation of Diuretics pharmacology in Hindi-English (Hinglish) style.
💊 Diuretics — Complete Pharmacology
🔑 Definition
Diuretics woh drugs hain jo urine output badhate hain — kidney se Na⁺ aur water ki reabsorption ko rokke.
"Most diuretics act on the luminal membrane from within the renal tubules — secreted by the proximal tubule via the organic anion pump." — Morgan & Mikhail's Clinical Anesthesiology
🗺️ Sites of Action — Nephron Diagram
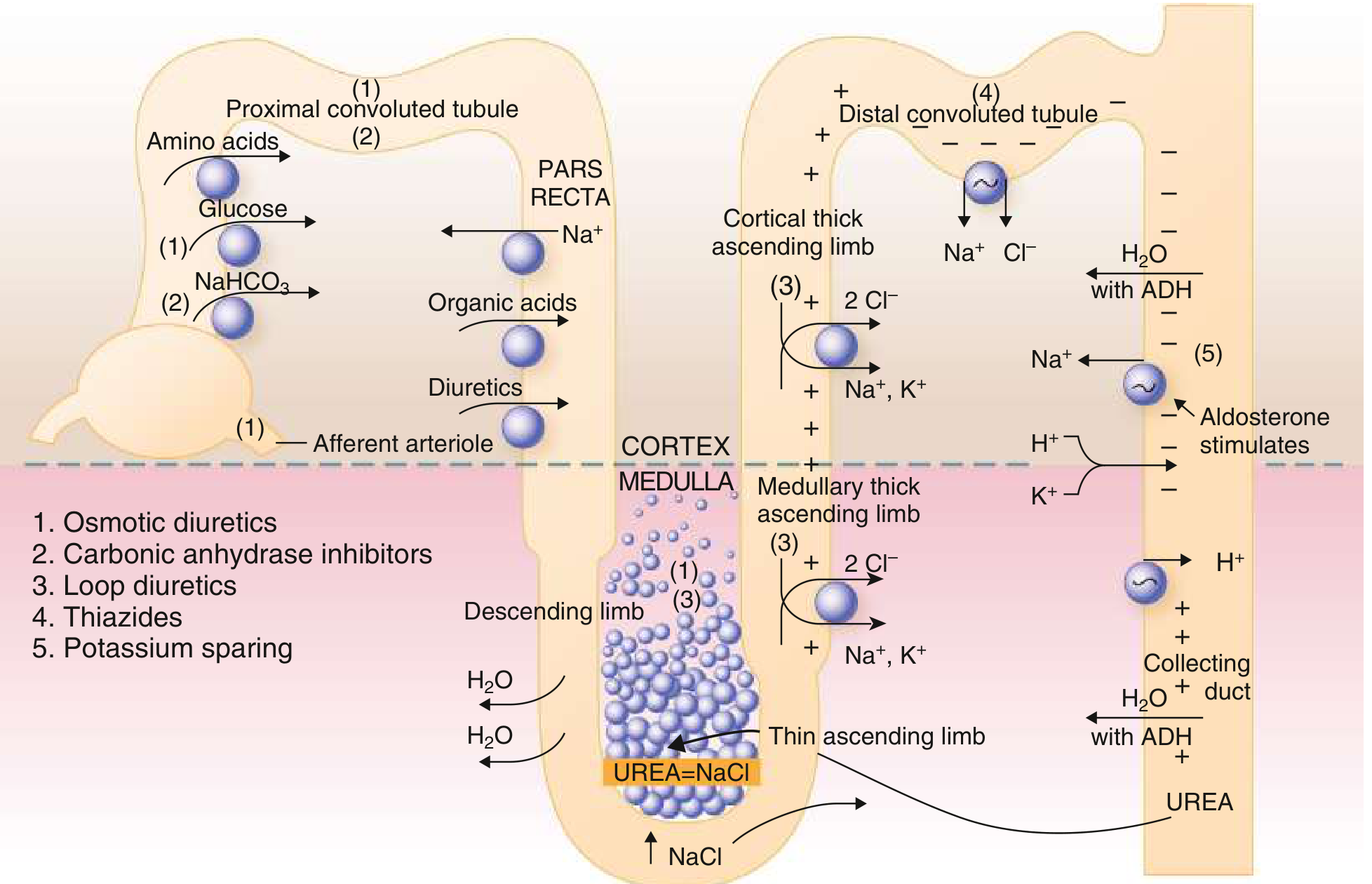
Nephron ke alag-alag segments pe alag classes kaam karti hain — Goldman-Cecil Medicine
📚 Classification (5 Major Classes)
| Class | Site of Action | Example Drugs |
|---|---|---|
| 1. Osmotic Diuretics | Proximal tubule + Loop of Henle | Mannitol |
| 2. Carbonic Anhydrase Inhibitors | Proximal tubule | Acetazolamide |
| 3. Loop Diuretics | Thick ascending limb of Loop of Henle | Furosemide, Bumetanide, Torsemide |
| 4. Thiazides | Distal convoluted tubule (DCT) | Hydrochlorothiazide, Chlorthalidone, Metolazone, Indapamide |
| 5. Potassium-Sparing | Late DCT + Collecting duct | Spironolactone, Eplerenone, Amiloride, Triamterene |
1️⃣ OSMOTIC DIURETICS (Mannitol)
Mechanism
- Glomerulus mein filter hota hai, reabsorb nahi hota
- Tubule lumen mein osmotically active rehta hai
- Water passive reabsorption block karta hai (jahan Na⁺ reabsorb hota hai, wahan paani follow nahi kar paata)
- Large doses mein electrolyte excretion bhi badhata hai
Extra Benefits of Mannitol
- Renal blood flow (RBF) badhata hai
- Vasodilating prostaglandins synthesize karta hai
- Free radical scavenger bhi hai
Dose
- IV: 0.25 to 1 g/kg
Uses
| Use | Detail |
|---|---|
| Raised ICP / Cerebral edema | Drug of choice |
| Raised intraocular pressure | Pre-op |
| Acute oliguria evaluation | Limited role |
⚠️ Note
High-dose mannitol nephrotoxic ho sakta hai — especially impaired kidney function mein. AKI se protection ka koi strong clinical evidence nahi hai.
2️⃣ CARBONIC ANHYDRASE INHIBITORS (Acetazolamide)
Mechanism
- Proximal tubule mein NaHCO₃ reabsorption block karta hai
- Carbonic anhydrase enzyme inhibit → H⁺ kam banta hai → Na⁺/H⁺ exchange kam hota hai
- Weak diuretic — because loop of Henle compensate kar leta hai
Uses
| Use | Detail |
|---|---|
| Glaucoma | Aqueous humor formation kam karta hai (ciliary body pe action) — most important use |
| Metabolic alkalosis | "Contraction alkalosis" jo other diuretics se hoti hai, use correct karta hai |
| Urine alkalinization | Uric acid, weakly acidic drugs ki excretion badhata hai |
| Altitude sickness | Prophylaxis |
Side Effects
- Hyperchloremic metabolic acidosis
- Hypokalemia (severe)
- Drowsiness, paresthesias (large doses)
- Topical forms: Dorzolamide, Brinzolamide (glaucoma ke liye)
Dose
- IV: 250–500 mg (acetazolamide)
3️⃣ LOOP DIURETICS ⭐ (Most Potent)
Drugs
Furosemide (Lasix), Bumetanide (Bumex), Torsemide (Demadex), Ethacrynic acid (Edecrin)
Mechanism
- Thick ascending limb of Loop of Henle pe kaam karta hai
- Na⁺-K⁺-2Cl⁻ cotransporter (NKCC2) ko block karta hai — Cl⁻ ke liye compete karta hai
- Sodium excretion upto 20–25% of filtered load (sabse zyada!)
- Free water clearance enhance karta hai
- Medullary hypertonicity destroy karta hai → concentrating ability impair
Extra Hemodynamic Effect
- IV furosemide venodilator hai — within minutes right atrial pressure aur PCWP girta hai
- Prostaglandins release se — NSAIDs se block ho sakta hai
- Acute SVR rise bhi ho sakta hai (RAAS activation se)
Drugs Are Secreted
- Protein-bound hain → filtration limited
- Proximal tubule se OAT1, OAT2 (organic anion transporters) via secreted hote hain
- CKD mein: tubular secretion slow → zyada dose chahiye
Uses
| Use | Dose |
|---|---|
| Acute Heart Failure (AHF) | Moderate: Furosemide 20–40 mg IV; Severe: upto 160 mg |
| Chronic HF, volume overload | Mainstay of treatment |
| Hypercalcemia | Saline + Furosemide combination |
| Acute Pulmonary Edema | IV furosemide |
| Hypertension | Second line |
DOSE Trial (Important!)
- 2×2 factorial design — bolus vs continuous infusion, low vs high dose
- High dose → better dyspnea relief, more fluid loss (but transient creatinine rise)
- Bolus vs infusion → no significant difference
Side Effects
| Effect | Mechanism |
|---|---|
| Hypokalemia | Na⁺ delivery to DCT badhta hai → K⁺ exchange badhta hai |
| Metabolic alkalosis | H⁺ loss, secondary hyperaldosteronism |
| Hypomagnesemia | Mg²⁺ wasting |
| Hypocalcemia | Ca²⁺ wasting (thiazide se OPPOSITE) |
| Hyperuricemia | Urate reabsorption badhta hai + proximal tubule mein competitive inhibition |
| Ototoxicity | Esp. furosemide & ethacrynic acid — reversible AND irreversible hearing loss |
| Hypovolemia, pre-renal azotemia | Volume depletion se |
4️⃣ THIAZIDE & THIAZIDE-LIKE DIURETICS
Drugs
- Thiazides: Hydrochlorothiazide (HCTZ), Chlorothiazide
- Thiazide-like: Chlorthalidone, Metolazone, Quinethazone, Indapamide
Mechanism
- Distal convoluted tubule (DCT) + connecting segment pe kaam karta hai
- Na⁺-Cl⁻ cotransporter ko block karta hai (Cl⁻ site pe compete karta hai)
- Na⁺ excretion sirf 3–5% of filtered load (loop se kam)
- Diluting capacity impair karta hai, but concentrating capacity normal rehti hai
- Ca²⁺ reabsorption BADHATA hai (DCT mein) ← loop diuretic se OPPOSITE!
- Carbonic anhydrase inhibition bhi hoti hai (proximal tubule mein) — but usually masked
Special Property of Indapamide
- Vasodilating properties bhi hain
- Significant hepatic excretion — sirf iska yeh property hai
Uses
| Use | Detail |
|---|---|
| Hypertension | First-line agent — long-term outcomes improve karta hai |
| Mild-moderate edema, mild HF | Second line |
| Hypercalciuria | Calcium-containing kidney stones prevent karta hai (Ca²⁺ reabsorption badhata hai) |
| Nephrogenic Diabetes Insipidus | Diluting capacity impair karta hai → urine osmolality badhti hai |
⚠️ Limitation
- GFR < 30–40 mL/min mein ineffective ho jaate hain
- Exception: Metolazone — GFR 20–30 mL/min tak kaam karta hai
Side Effects
| Effect | Note |
|---|---|
| Hypokalemia | DCT pe Na⁺ delivery badhti hai |
| Hyperglycemia | Beta-cell insulin secretion impair |
| Hyperuricemia | Gout worsen kar sakta hai |
| Hypercalcemia | Ca²⁺ reabsorption badhti hai |
| Hyponatremia | Diluting capacity impair |
| Rash, neutropenia, thrombocytopenia | Rare |
5️⃣ POTASSIUM-SPARING DIURETICS
Two Sub-Types:
A) Aldosterone Antagonists
- Spironolactone aur Eplerenone
- Late DCT + Collecting duct mein aldosterone receptor block karte hain
- Aldosterone kam kaam karta hai → Na⁺ reabsorption kam → K⁺ bacha rehta hai
- Cardiac remodeling improve karte hain systolic HF mein ← extra benefit!
B) ENaC Blockers
- Amiloride aur Triamterene
- Late DCT + Collecting duct mein epithelial Na⁺ channel (ENaC) block karte hain
- Direct — aldosterone-independent
- K⁺ exchange nahi hota → potassium retain hota hai
Uses
| Use | Detail |
|---|---|
| HF with reduced EF | Spironolactone (RALES trial), Eplerenone (EMPHASIS trial) — mortality reduce karte hain |
| Combined with loop/thiazide | K⁺ loss correct karna |
| Primary hyperaldosteronism | Spironolactone |
| Hypertension | Combination therapy |
Side Effects
| Drug | Side Effect |
|---|---|
| Spironolactone | Gynecomastia, menstrual irregularity (anti-androgen effect) |
| Eplerenone | Selective — gynecomastia kam (more selective MR antagonist) |
| Amiloride/Triamterene | Hyperkalemia — most important |
| All | Hyperkalemia — ACE inhibitor/ARB ke saath cautiously use karein |
🔄 Diuretic Synergism
Loop + Thiazide/Metolazone combination — sequential nephron blockade → synergistic natriuresis
- Loop diuretic se jo Na⁺ bachta hai, DCT mein reabsorb hota hai
- Thiazide add karo → DCT bhi block → double blockade
- Metolazone is preferred because works even in CKD
⚠️ DIURETIC RESISTANCE
Definition: Adequate dose dene ke bawajood desired natriuresis nahi milti
Algorithm:
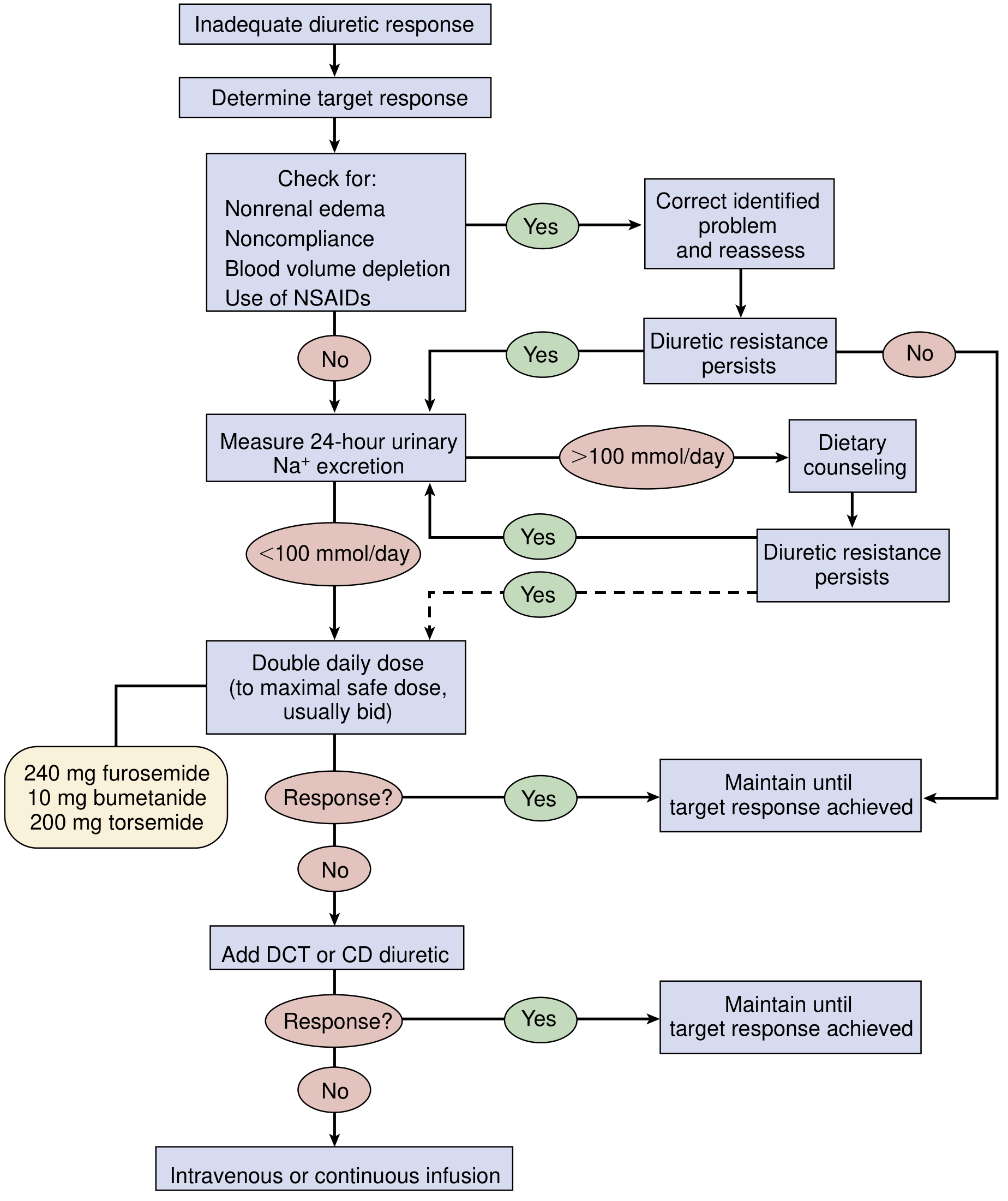
National Kidney Foundation Primer on Kidney Diseases
Common Causes:
| Cause | Solution |
|---|---|
| High Na⁺ intake | 24-hr urinary Na⁺ >100 mmol → dietary counseling |
| NSAIDs (block prostaglandins) | Stop NSAIDs |
| Non-compliance | Reassess |
| Hypoalbuminemia (nephrotic) | Drug delivery impaired → IV furosemide 80–120 mg |
| CKD | Tubular secretion slow → larger doses chahiye |
| Blood volume depletion | Correct first |
Steps to Overcome:
- Check for correctable causes first
- Measure 24-hr urinary Na⁺
- Double the daily dose (max: Furosemide 240 mg, Bumetanide 10 mg, Torsemide 200 mg)
- Add DCT diuretic (thiazide/metolazone)
- IV or continuous infusion — last resort
Quick Test:
FENa >2% (1–2 hr after diuretic) → true resistance unlikely — NKF Primer on Kidney Diseases
💉 Special Note: SGLT2 Inhibitors (Modern "Diuretics")
- Empagliflozin, Dapagliflozin — SGLT2 block → glucose + Na⁺ excretion
- Proximal tubule mein 1:1 stoichiometric Na⁺ + glucose inhibition
- Volume contraction → modest BP lowering
- Tubuloglomerular feedback → afferent arteriole vasoconstriction → glomerular hyperfiltration kam
- HFrEF mein significant mortality benefit (EMPEROR-Reduced, DAPA-HF)
📊 Quick Comparison Table
| Feature | Loop | Thiazide | K⁺-Sparing |
|---|---|---|---|
| Potency | ⭐⭐⭐ Highest | ⭐⭐ Moderate | ⭐ Weak |
| Na⁺ excretion | 20–25% | 3–5% | 1–2% |
| Site | Loop (TAL) | DCT | Late DCT/CD |
| K⁺ effect | ↓ Hypokalemia | ↓ Hypokalemia | ↑ Hyperkalemia |
| Ca²⁺ effect | ↑ Hypercalciuria | ↓ Hypocalciuria | Neutral |
| Use in CKD | ✅ Effective | ❌ Loses effect <30-40 mL/min | Careful (hyperK risk) |
| Ototoxicity | ✅ Yes | ❌ No | ❌ No |
🎯 High-Yield Points (Exam ke liye)
- Most potent diuretic → Loop diuretics (furosemide)
- First-line for hypertension → Thiazides
- Ototoxicity → Loop diuretics (esp. ethacrynic acid > furosemide)
- Hypercalciuria treatment → Thiazides (Ca²⁺ reabsorption badhate hain)
- Hypercalcemia treatment → Furosemide + IV saline
- Nephrogenic DI → Thiazides (paradoxical)
- Gynecomastia → Spironolactone
- Glaucoma + altitude sickness → Acetazolamide
- Mortality benefit in HFrEF → Spironolactone (RALES), Eplerenone (EMPHASIS)
- Mannitol → ICP kam karta hai, NOT kidney protection
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e | Braunwald's Heart Disease | Goldman-Cecil Medicine | Lippincott Pharmacology | NKF Primer on Kidney Diseases
Anti hypertensve drug
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Ab mere paas bahut rich content hai. Comprehensive answer likhta hoon:
💊 Antihypertensive Drugs — Complete Pharmacology
🔑 Definition
Hypertension: Systolic BP > 130 mmHg ya Diastolic BP > 80 mmHg
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
Antihypertensive drugs ya toh CO kam karte hain, ya PVR kam karte hain, ya dono.
🗺️ Sites of Action — Master Diagram
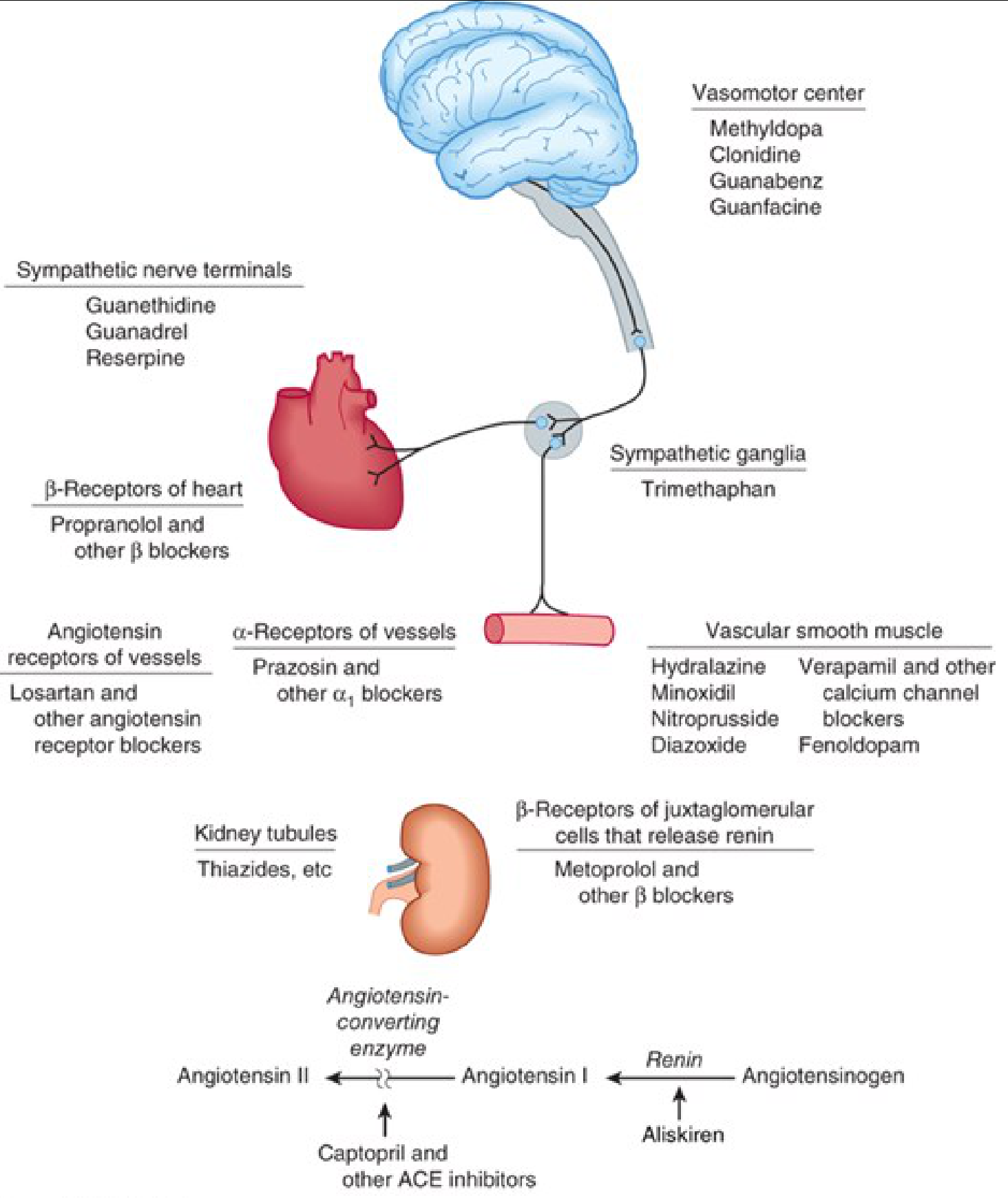
Katzung's Basic & Clinical Pharmacology — Har class kahaan kaam karti hai
📚 CLASSIFICATION (4 Major Groups)
| Group | Classes |
|---|---|
| 1. Diuretics | Thiazides, Loop, K⁺-sparing |
| 2. RAAS Blockers | ACE inhibitors, ARBs, Aliskiren |
| 3. Sympathoplegics | Beta-blockers, Alpha-blockers, Central agents |
| 4. Vasodilators | CCBs, Hydralazine, Minoxidil, Nitroprusside |
1️⃣ DIURETICS (Antihypertensive mechanism)
Mechanism in Hypertension
- Initial effect: Blood volume kam → Cardiac output kam → BP kam
- After 6-8 weeks: CO normal ho jaata hai, lekin PVR kam ho jaata hai
- Sodium vessel stiffness badhata hai → Na restriction se vessel reactivity kam hoti hai
BP lowering capacity
Diuretics akele 10-15 mmHg BP kam kar sakte hain
Drug of Choice for HTN
- Thiazides = First-line for uncomplicated hypertension
- Thiazide-like (Chlorthalidone, Indapamide) = preferred due to longer half-life
- Metolazone = CKD mein bhi kaam karta hai (GFR 20-30 mL/min tak)
2️⃣ RAAS BLOCKERS ⭐ (Most important group)
RAAS Pathway (Samajhna zaroori hai):
Angiotensinogen
↓ (Renin) ← Aliskiren block karta hai
Angiotensin I
↓ (ACE) ← ACE Inhibitors block karte hain
Angiotensin II ← ARBs receptor level pe block karte hain
↓
Aldosterone → Na+ retention → BP ↑
↓
Vasoconstriction → PVR ↑ → BP ↑
A) ACE INHIBITORS
Drugs: Captopril, Enalapril, Lisinopril, Ramipril, Benazepril, Fosinopril, Perindopril, Quinapril, Trandolapril
(Yaad karne ka trick: "CELBRQPFT")
Mechanism (Double Action):
- ACE block → Angiotensin II nahi banta → Vasodilation, Aldosterone kam
- Bradykinin inactivation nahi hoti → Bradykinin accumulate → Vasodilation (NO + Prostacyclin se)
Important Pharmacokinetics:
- Captopril = Direct active drug
- Enalapril = Prodrug → Liver mein Enalaprilat banta hai (IV form = Enalaprilat)
- Lisinopril = Lysine derivative of Enalaprilat (NOT a prodrug)
- Most others = Prodrugs, hepatic conversion
Hemodynamic Effect:
- PVR kam karta hai
- CO aur HR significant change nahi hoti
- No reflex tachycardia ← because baroreceptor resetting hoti hai (vasodilators se alag!)
Uses:
| Condition | Why Preferred |
|---|---|
| Hypertension | First-line |
| Heart Failure (HFrEF) | Mortality benefit |
| Post-MI | Cardiac remodeling rokta hai |
| Diabetic nephropathy | Proteinuria kam karta hai |
| CKD | Renoprotection |
| Left ventricular hypertrophy | Regression |
Side Effects (IMPORTANT!):
| Side Effect | Mechanism |
|---|---|
| Dry cough ⭐ | Bradykinin + Substance P accumulation (lungs) |
| Angioedema | Bradykinin accumulation (rare but dangerous) |
| Hyperkalemia | Aldosterone kam → K⁺ retain hoti hai |
| Hypotension (first dose) | Esp. if hypovolemic/on diuretics |
| Acute renal failure | Bilateral renal artery stenosis mein |
| Teratogenic | 2nd & 3rd trimester contraindicated |
| Neutropenia, proteinuria | Captopril high dose mein |
| Altered taste, skin rash | Minor (10% patients) |
Drug Interactions:
- NSAIDs → prostaglandin-mediated vasodilation block → efficacy kam
- K⁺ sparing diuretics → Hyperkalemia risk
- ACE + ARB combination = NOT recommended (toxicity)
B) ANGIOTENSIN RECEPTOR BLOCKERS (ARBs)
Drugs: Losartan, Valsartan, Candesartan, Irbesartan, Telmisartan, Olmesartan, Azilsartan, Eprosartan
(Yaad karne ka trick: Sab "-sartan" mein khatam hote hain)
Mechanism:
- AT1 receptor ko competitive block karte hain
- ACE inhibitors se zyada selective (bradykinin metabolism affect nahi karte)
- Angiotensin II ke sab sources ko block karte hain (ACE ke alawa bhi enzymes hain)
ARBs vs ACE inhibitors:
| Feature | ACE Inhibitor | ARB |
|---|---|---|
| Bradykinin | ↑ (accumulates) | Normal |
| Cough | Common ⭐ | Uncommon |
| Angioedema | More common | Rare (can occur) |
| Selectivity | Less (other ACE substrates bhi) | More selective |
| Angiotensin II block | Incomplete | More complete |
| Pregnancy | Contraindicated | Contraindicated |
Note: Valsartan + Sacubitril (Neprilysin inhibitor) = ARNI (Entresto) → HF treatment mein use hota hai
C) ALISKIREN (Direct Renin Inhibitor)
- RAAS ka pehla step (Renin) block karta hai
- Oral bioavailability
- ACE/ARB ke saath combination = avoid (toxicity in trials)
3️⃣ SYMPATHOPLEGIC DRUGS
Why Needed?
- BP badhane mein sympathetic system major role play karta hai
- Lekin ek important limitation: Sodium retain karne lagte hain → diuretic ke saath use karna chahiye
Compensatory response diagram:
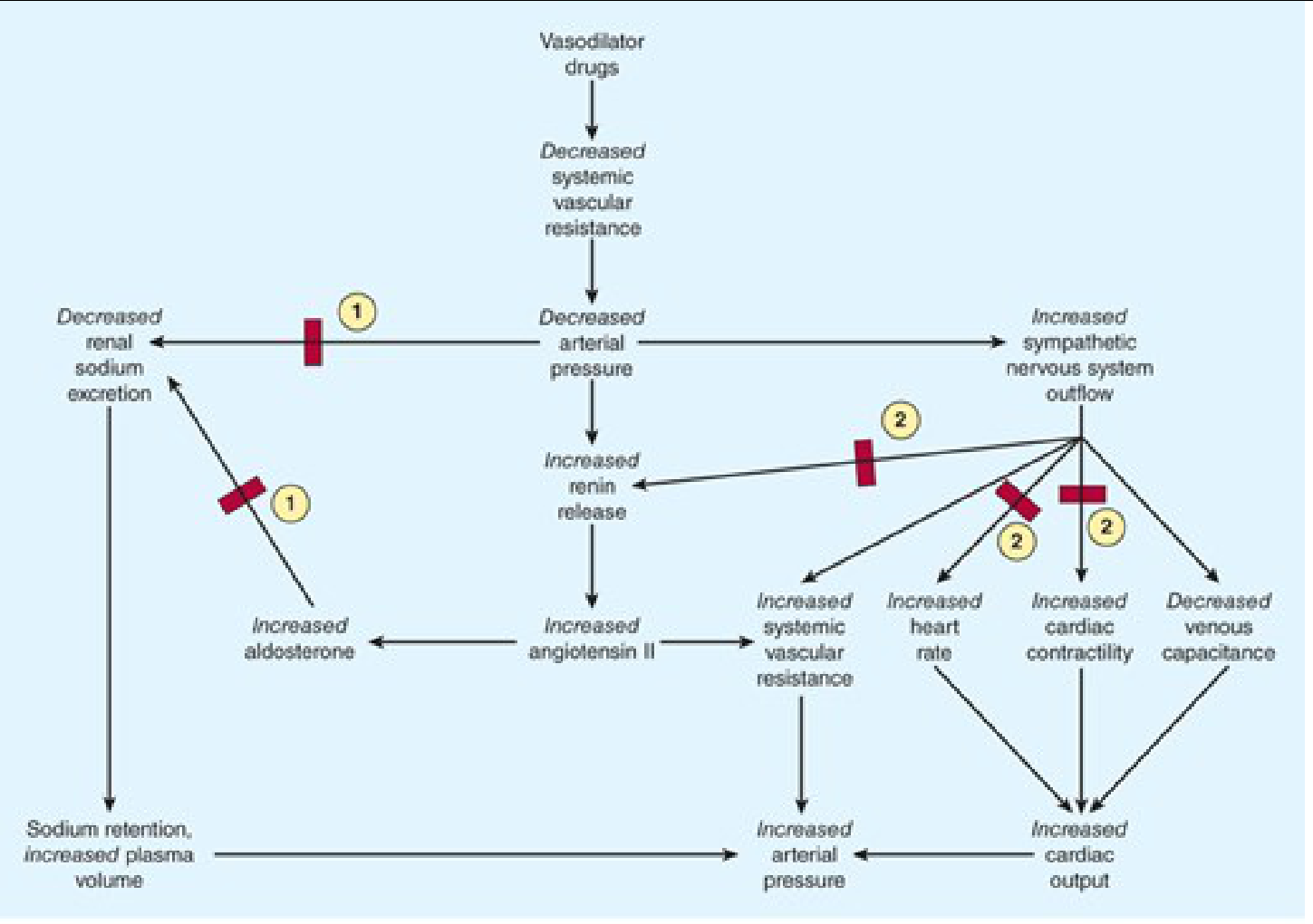
Block 1 = Diuretics block karte hain; Block 2 = Beta-blockers block karte hain
A) BETA-BLOCKERS (β-Blockers)
Drugs:
- Non-selective: Propranolol, Nadolol, Timolol, Carvedilol (α+β)
- Cardioselective (β1): Metoprolol, Atenolol, Bisoprolol, Esmolol
- Vasodilating β1-blocker: Nebivolol (β1 block + NO release)
Mechanism (Multiple):
- Heart mein β1 block → Heart rate ↓ + Contractility ↓ → CO ↓ → BP ↓
- Kidney mein β1 block (JGA cells) → Renin release ↓ → Angiotensin II ↓ → BP ↓
- CNS mein sympathetic outflow ↓
- Baroreceptor sensitivity reset
Uses in HTN:
| Condition | Drug |
|---|---|
| HTN + Angina | Beta-blocker preferred |
| HTN + Post-MI | Beta-blocker (mortality benefit) |
| HTN + HFrEF | Carvedilol, Metoprolol, Bisoprolol |
| HTN + AF | Rate control ke liye |
| Pheochromocytoma | Alpha-blocker PEHLE, then Beta |
Side Effects:
| Side Effect | Note |
|---|---|
| Bronchoconstriction | β2 block → Asthma/COPD mein contraindicated (non-selective) |
| Bradycardia, heart block | Conduction system pe |
| Masking of hypoglycemia | β2 block → Diabetics mein caution |
| Cold extremities | Peripheral vasoconstriction |
| Fatigue, sexual dysfunction | Common |
| Metabolic effects | Dyslipidemia, insulin resistance |
Contraindications:
- Asthma (non-selective)
- Bradycardia / 2nd-3rd degree heart block
- Severe peripheral vascular disease
- Acute decompensated HF
B) ALPHA-1 BLOCKERS (α1-Blockers)
Drugs: Prazosin, Doxazosin, Terazosin
Mechanism:
- Vascular smooth muscle ke α1 receptors block → Arteriolar + venous dilation → PVR ↓ → BP ↓
- Reflex tachycardia ho sakti hai
Uses:
- HTN with BPH (best choice — symptoms bhi theek ho jaate hain)
- Pheochromocytoma (Phenoxybenzamine — non-selective)
Side Effect — "First Dose Effect"
Prazosin ki pehli dose mein severe postural hypotension + syncope ho sakti hai Solution: Bedtime pe low dose se start karein
C) CENTRAL SYMPATHOLYTICS
Methyldopa
- L-dopa analog → α-methyldopamine → α-methylnorepinephrine banta hai
- False transmitter — vasomotor centers mein sympathetic outflow ↓ karta hai
- Drug of choice in PREGNANCY-induced hypertension ⭐
- Side effects: Sedation, hepatotoxicity, hemolytic anemia, positive Coombs test
Clonidine
- α2 agonist → Brainstem vasomotor center → Sympathetic outflow ↓
- Uses: HTN, opioid withdrawal, ADHD
- Withdrawal = Rebound hypertension (abruptly band mat karo!)
- Side effects: Sedation, dry mouth
4️⃣ VASODILATORS
A) CALCIUM CHANNEL BLOCKERS (CCBs) ⭐
Types:
| Type | Drugs | Selectivity |
|---|---|---|
| Dihydropyridines (DHP) | Nifedipine, Amlodipine, Felodipine, Nicardipine, Clevidipine | Vascular > Cardiac |
| Non-DHP: Phenylalkylamines | Verapamil | Cardiac > Vascular |
| Non-DHP: Benzothiazepines | Diltiazem | Intermediate |
Mechanism:
- Vascular smooth muscle + Cardiac cells mein L-type Ca²⁺ channels block
- Ca²⁺ entry kam → Smooth muscle relaxation → Vasodilation → PVR ↓ → BP ↓
- DHP mainly arteriolar dilation
- Verapamil + Diltiazem = Heart rate bhi slow karte hain (AV node effect)
Uses:
| Condition | CCB |
|---|---|
| HTN + Angina | All CCBs |
| HTN + Atrial Fibrillation (rate control) | Verapamil / Diltiazem |
| HTN + Elderly | Very effective |
| HTN + CKD | DHP preferred |
| Hypertensive Emergency | IV Nicardipine, IV Clevidipine |
| Raynaud's phenomenon | Nifedipine |
Side Effects:
| Drug | Side Effect |
|---|---|
| Amlodipine/Nifedipine | Peripheral edema, flushing, reflex tachycardia (DHP) |
| Verapamil | Constipation ⭐, bradycardia, heart block, avoid in HF |
| Diltiazem | Bradycardia (intermediate) |
| All | Headache, dizziness |
Verapamil + Beta-blocker = Dangerous combination → Complete heart block ka risk!
B) HYDRALAZINE
Mechanism:
- Arterioles dilate karta hai, veins nahi
- Nitric oxide release → Guanylyl cyclase activate → cGMP ↑ → Smooth muscle relax
Important Points:
- Oral bioavailability 25% only (high first-pass metabolism)
- Slow vs Fast acetylators mein different response
- Reflex tachycardia + Na/water retention hoti hai → Beta-blocker + Diuretic ke saath use karo
- Uses: Pregnancy HTN (IV), Severe HTN, HF (Hydralazine + Isosorbide dinitrate)
Side Effects:
| Side Effect | Note |
|---|---|
| Reflex tachycardia, palpitations | Sympathetic activation |
| Drug-induced SLE (Lupus-like syndrome) ⭐ | >200 mg/day, slow acetylators mein zyada |
| Headache, flushing | |
| Peripheral neuropathy | Pyridoxine (B6) deficiency se |
C) MINOXIDIL
Mechanism:
- K⁺ channels open karta hai → Cell hyperpolarize → Ca²⁺ entry kam → Vasodilation
- Most potent oral vasodilator — severe/resistant HTN mein
Must Use With:
- Beta-blocker (reflex tachycardia rokne ke liye)
- Diuretic (Na/water retention rokne ke liye)
Side Effects:
- Hypertrichosis (har jagah baal ugna) ⭐ — Topical minoxidil = Rogaine (baldness treatment!)
- Tachycardia, edema, angina
D) SODIUM NITROPRUSSIDE (IV — Emergency)
Mechanism:
- Arteries + Veins dono dilate karta hai (unique!)
- NO release → cGMP ↑ → Smooth muscle relax
Important Facts:
- Hypertensive Emergency drug of choice in most situations
- Onset: Immediate, Duration: 1-10 minutes after stopping
- Route: IV infusion only
- Light sensitive → Opaque foil se cover karo
- Fresh solution banana padta hai
Dose:
- Start: 0.5 mcg/kg/min
- Max: 10 mcg/kg/min
Toxicity:
- Cyanide toxicity — Nitroprusside → RBC mein NO + Cyanide release
- Cyanide → Rhodanese enzyme → Thiocyanate (less toxic)
- Thiocyanate accumulation → Nausea, confusion, hypothyroidism (renal failure mein zyada risk)
E) FENOLDOPAM (IV — Emergency)
- Dopamine D1 receptor agonist
- Vasodilation + Renal blood flow badhata hai (unique advantage)
- HTN emergency mein — especially renal function preserve karna ho
🚨 HYPERTENSIVE EMERGENCY vs URGENCY
| Feature | Emergency | Urgency |
|---|---|---|
| BP | >180/120 mmHg | >180/120 mmHg |
| Target Organ Damage | Present (stroke, MI, AKI) | Absent |
| Treatment | IV drugs, ICU | Oral drugs, outpatient |
| BP reduction speed | 25% in 1st hour, then slow | Gradual over 24-48 hrs |
Drugs for Hypertensive Emergency:
| Drug | Preferred When |
|---|---|
| Nitroprusside | Most emergencies, aortic dissection |
| Labetalol (α+β blocker) | Stroke, pregnancy |
| Nicardipine (IV CCB) | Neuro emergencies |
| Clevidipine | Perioperative HTN |
| Esmolol | Tachyarrhythmia + HTN |
| Fenoldopam | Renal impairment ke saath |
| Enalaprilat (IV ACE-I) | HTN + HF |
| Hydralazine (IV) | Pregnancy-induced HTN |
| Nitroglycerin (IV) | ACS + HTN |
| Phentolamine (α-blocker) | Pheochromocytoma, MAOI crisis |
⚠️ "Rapid BP reduction as dangerous as hypertensive state itself" — Goldman-Cecil Medicine
🎯 Compelling Indications Table (Must Know!)
| Condition | Preferred Drug | Avoid |
|---|---|---|
| Uncomplicated HTN | Thiazide, CCB, ACE-I, ARB | - |
| Diabetes + HTN | ACE-I or ARB | Beta-blocker (masks hypoglycemia) |
| CKD + proteinuria | ACE-I or ARB | - |
| Post-MI | Beta-blocker + ACE-I | - |
| HFrEF | ACE-I/ARB, Beta-blocker, MRA | Verapamil/Diltiazem |
| Angina + HTN | Beta-blocker or CCB | - |
| Pregnancy HTN | Methyldopa, Labetalol, Hydralazine | ACE-I, ARBs ❌ |
| BPH + HTN | Alpha-1 blocker (Doxazosin) | - |
| Elderly | Thiazide, CCB | Beta-blocker less preferred |
| Pheochromocytoma | Phenoxybenzamine (alpha FIRST) | Beta alone ❌ |
| AF + HTN | Verapamil/Diltiazem or Beta-blocker | - |
| Raynaud's | CCB (Nifedipine) | Beta-blocker ❌ |
💊 Resistant Hypertension
Definition: BP above goal despite 3 drugs (including a diuretic) at optimal doses
Common Causes:
- Poor compliance
- Excessive salt intake
- NSAIDs use
- Secondary HTN (sleep apnea, renal artery stenosis, primary aldosteronism)
- Obesity, excessive alcohol
Management:
- 3-drug combination (Diuretic + CCB + ACE-I/ARB) — kaafi patients ke liye standard
- Add Spironolactone — 4th drug ke roop mein very effective
- Sometimes 4+ drugs lagte hain
📊 Quick Drug Summary Table
| Class | Examples | Main Action | Key SE |
|---|---|---|---|
| Thiazides | HCTZ, Chlorthalidone | Na excretion, volume ↓ | Hypokalemia, Hyperuricemia |
| ACE-I | Enalapril, Ramipril | RAAS block, Bradykinin ↑ | Cough, Hyperkalemia, Teratogenic |
| ARBs | Losartan, Valsartan | AT1 block | Hyperkalemia, Teratogenic |
| Beta-blockers | Metoprolol, Carvedilol | HR ↓, CO ↓, Renin ↓ | Bronchospasm, Bradycardia |
| DHP-CCBs | Amlodipine, Nifedipine | Arterial vasodilation | Edema, Reflex tachy |
| Non-DHP CCBs | Verapamil, Diltiazem | Vasodilation + HR ↓ | Constipation, Bradycardia |
| Hydralazine | Hydralazine | Arteriolar dilation | SLE-like, Tachycardia |
| Minoxidil | Minoxidil | K⁺ channel open | Hypertrichosis |
| Nitroprusside | Nitroprusside | NO release (art + vein) | Cyanide toxicity |
| Central | Methyldopa, Clonidine | Sympathetic outflow ↓ | Sedation, Rebound HTN |
| α1-blockers | Prazosin, Doxazosin | α1 block → Vasodilation | First dose hypotension |
🎯 High-Yield Exam Points
- First-line HTN → Thiazide / CCB / ACE-I / ARB (any one)
- ACE-I side effect → Dry cough (bradykinin se)
- ARB advantage over ACE-I → No cough
- Pregnancy HTN → Methyldopa / Labetalol / Hydralazine; ACE-I & ARB contraindicated
- Hypertensive emergency → IV Nitroprusside (most cases)
- Drug-induced SLE → Hydralazine (>200 mg, slow acetylators)
- Hypertrichosis → Minoxidil (topically = Rogaine for baldness)
- First dose hypotension → Prazosin (α1 blocker)
- Verapamil + Beta-blocker → Complete heart block risk
- Rebound hypertension on stopping → Clonidine
- Pheochromocytoma → Alpha-blocker PEHLE, beta-blocker baad mein
- BPH + HTN → Alpha-1 blocker (dual benefit)
- Cyanide toxicity → Nitroprusside (overdose/prolonged use)
- Constipation → Verapamil (classic SE)
- Resistant HTN 4th drug → Spironolactone
Sources: Katzung's Basic & Clinical Pharmacology 16e | Lippincott Illustrated Reviews Pharmacology | Goldman-Cecil Medicine | Braunwald's Heart Disease | Morgan & Mikhail's Clinical Anesthesiology
This is a shared conversation. Sign in to Orris to start your own chat.