common site of fibrinoid necrosis
Reading File
Finding Sources
Reading File
Reading File
Here is a complete, textbook-based answer on the common sites of fibrinoid necrosis:
Fibrinoid Necrosis - Common Sites
Fibrinoid necrosis is a special form of necrosis visible by light microscopy, characterized by a bright pink, amorphous, fibrin-like appearance on H&E staining due to deposition of immune complexes and leaked plasma proteins in vessel walls.
Pathogenesis
It arises in two main settings:
- Immune complex deposition - antigen-antibody complexes deposited in vessel walls
- Severe/malignant hypertension - high intravascular pressure damages vessel walls, causing plasma protein leakage
Common Sites
| Condition | Site/Location |
|---|---|
| Vasculitis (polyarteritis nodosa, microscopic polyangiitis) | Walls of small and medium arteries |
| Malignant hypertension | Walls of arterioles |
| SLE (Lupus) | Small blood vessel walls (immune complex-mediated) |
| Rheumatoid arthritis | Rheumatoid nodules (center of the nodule) |
| Wegener granulomatosis (GPA) | Vessel walls |
| Transplant rejection | Transplanted organ vessels |
| Pauci-immune glomerulonephritis | Glomerular capillaries (segmental fibrinoid necrosis) |
Key Exam Points
- Most classic association: Polyarteritis nodosa (PAN) - the textbook image shows fibrinoid necrosis in the wall of an artery in a PAN patient, with "circumferential bright pink area of necrosis with protein deposition and inflammation"
- Vessel type: Predominantly affects small vessels and arterioles
- Mechanism: Immune complexes + leaked plasma proteins → fibrin-like material in vessel walls
- Seen most often in: Vasculitis and transplant rejection
Histological Appearance
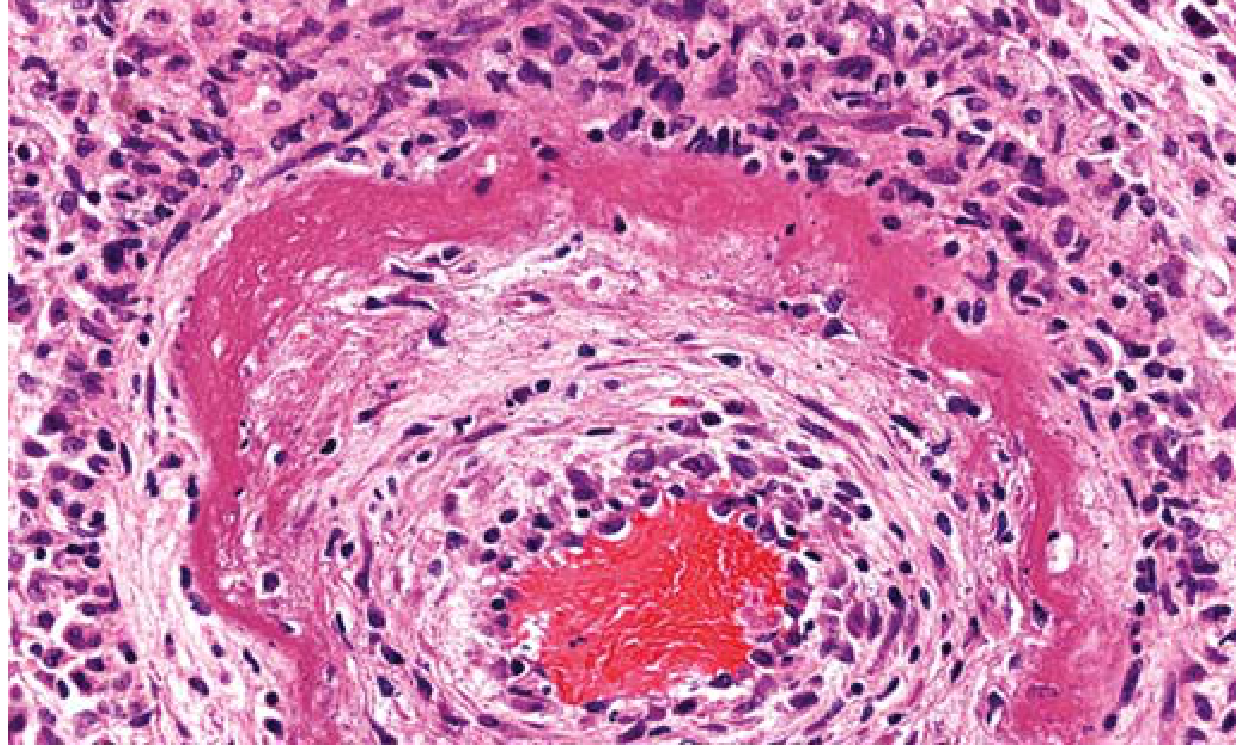
FIG. 1.10 - Fibrinoid necrosis in an artery in a patient with polyarteritis nodosa. The wall of the artery shows a circumferential bright pink area of necrosis with protein deposition and inflammation.
Bottom line for exams: The single most commonly tested association is blood vessel walls in vasculitis (especially PAN) and malignant hypertension. The necrosis is confined to vessel walls, not parenchyma, which distinguishes it from other types of necrosis.
- Robbins & Kumar Basic Pathology, p. 22
26 yr old pregnant women 1st baby complaints about oedema on leg.also numbness of hand,and jim jim kre.8 months start from today. What is the most likely cause
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete clinical breakdown:
Most Likely Diagnosis: Carpal Tunnel Syndrome (CTS) of Pregnancy
Understanding the Symptoms
| Symptom | Explanation |
|---|---|
| Leg edema | Physiological dependent edema of late pregnancy (8 months / ~32 weeks) - increased blood volume, uterine compression of IVC, reduced oncotic pressure |
| Hand numbness + "jim jim" (tingling/paresthesia) | Compression of the median nerve at the wrist due to fluid retention and soft tissue edema |
The combination of generalized edema + hand tingling in a 3rd trimester primigravida is the classic presentation of pregnancy-induced Carpal Tunnel Syndrome.
Why Does CTS Happen in Pregnancy?
Pregnancy causes:
- Fluid retention and soft tissue edema - increases pressure within the carpal tunnel
- Hormonal changes (relaxin, progesterone) - cause ligamentous laxity and connective tissue fluid accumulation
- Increased blood volume - adds to tissue swelling
This raises pressure in the fibro-osseous carpal tunnel beyond the normal 20-30 mmHg threshold, compressing the median nerve, which produces:
-
Numbness and tingling (paresthesia / "jim jim") in thumb, index, and middle fingers
-
Pain often worse at night
-
Sometimes clumsiness of the hand
-
Sabiston Textbook of Surgery, p. 2763 - "Metabolic, in which disturbances of fluid balance cause increased pressure on the nerve, particularly at the carpal tunnel (e.g., myxedema, pregnancy)"
-
Localization in Clinical Neurology, 8e - "conditions such as diabetes mellitus, rheumatoid arthritis, mucopolysaccharidosis, pregnancy, amyloidosis, hypothyroidism...may predispose to this syndrome"
Key Clinical Features of CTS in Pregnancy
- Bilateral in >50% of cases (but usually worse in the dominant hand)
- Symptoms worst at night or after sustained activity
- Relieved by shaking or rubbing the hand ("flick sign")
- Paresthesias in the median nerve distribution: thumb, index, middle, and radial half of ring finger
- Usually resolves after delivery as edema resolves
Positive Clinical Tests to Confirm
| Test | How to Perform | Positive if... |
|---|---|---|
| Phalen's test | Hyperflexion of wrist for 60 seconds | Tingling/numbness reproduced |
| Tinel's sign | Tap over carpal tunnel at wrist | Tingling shoots into fingers |
| Durkan sign | Direct compression of carpal canal | Paresthesias reproduced |
Important Differential to Rule Out
| Condition | Why Less Likely Here |
|---|---|
| Pre-eclampsia | No mention of hypertension, proteinuria, or headache |
| Cervical radiculopathy | Would follow a dermatomal pattern, not purely hand |
| Peripheral neuropathy | Usually feet involved first, no focal wrist pattern |
| DVT | Leg edema in pregnancy is physiological at 8 months with no other features |
Management in Pregnancy
- Wrist splints at night (neutral position) - first-line
- Activity modification - avoid prolonged wrist flexion
- Reassurance - most cases resolve within weeks after delivery
- Local corticosteroid injection - if severe, can be used in pregnancy
- Surgical decompression - rarely needed; reserved for postpartum persistent cases
Summary: A 26-year-old primigravida at 8 months with leg edema + hand numbness/tingling has Carpal Tunnel Syndrome secondary to pregnancy-associated fluid retention. The leg edema is physiological. The hand symptoms are from median nerve compression in the edematous carpal tunnel. This is one of the most common neurological complications of pregnancy.
This is a shared conversation. Sign in to Orris to start your own chat.