Explain the complete histology of organs associated with the digestive system
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have sufficient content from Junqueira's Basic Histology to provide a complete, authoritative answer. Let me compose the full response.
Histology of the Digestive System
The digestive system includes the gastrointestinal (GI) tract - a hollow tube from mouth to anus - and the accessory organs (salivary glands, liver, gallbladder, and pancreas). Below is a complete histological account of each organ.
I. General Wall Structure of the GI Tract
From the esophagus to the rectum, the wall has four concentric layers:
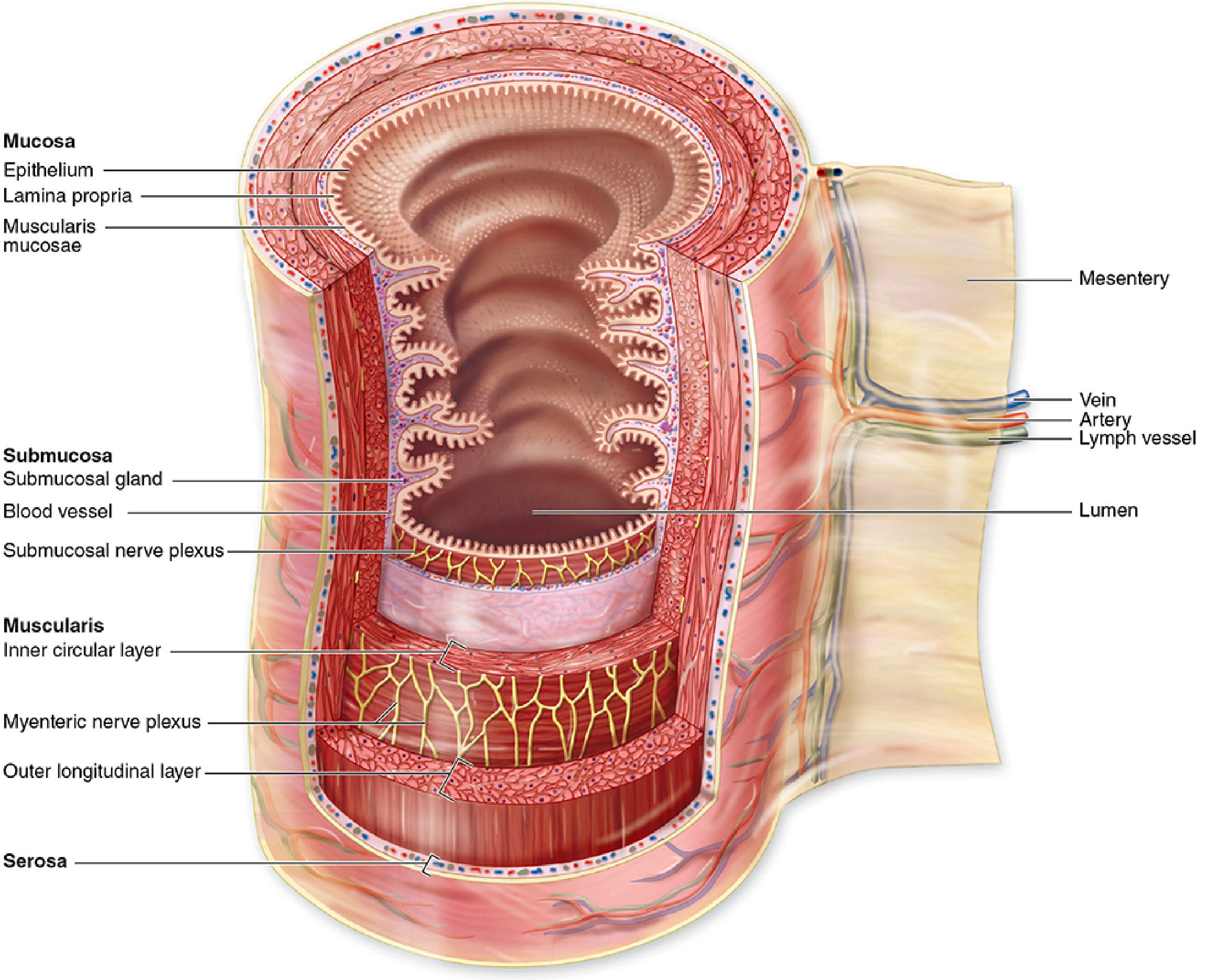
1. Mucosa
- Epithelium: varies by region (stratified squamous, simple columnar, etc.)
- Lamina propria: loose connective tissue with capillaries, lymphatics, free immune cells (macrophages, lymphocytes, IgA-secreting plasma cells), and small glands
- Muscularis mucosae: thin inner circular + outer longitudinal smooth muscle; permits local mucosal movements
2. Submucosa
- Denser connective tissue with larger blood vessels, lymphatics, adipose tissue
- Contains Meissner (submucosal) plexus of autonomic ganglia
- May contain glands (e.g., Brunner's glands in the duodenum) and lymphoid tissue (MALT)
3. Muscularis (Muscularis Externa)
- Two smooth muscle sublayers: inner circular + outer longitudinal
- Myenteric (Auerbach) plexus between the layers: generates and coordinates peristalsis
- Together with the Meissner plexus, forms the enteric nervous system
- Exception: the upper esophagus has striated muscle
4. Serosa / Adventitia
- Stomach and intestines: serosa = loose connective tissue covered by simple squamous mesothelium, continuous with the mesentery
- Esophagus and retroperitoneal portions: adventitia = connective tissue blending with surrounding structures (no mesothelial cover)
MALT (Mucosa-Associated Lymphoid Tissue): Abundant throughout, with lamina propria lymphocytes producing secretory IgA, which undergoes transcytosis into the lumen and resists proteolytic digestion.
II. Oral Cavity
Mucosa
- Lining mucosa (cheeks, soft palate, floor of mouth, oral pharynx): nonkeratinized stratified squamous epithelium over a thick submucosa with minor salivary glands
- Masticatory mucosa (hard palate, gingiva): keratinized stratified squamous epithelium; lamina propria attaches directly to periosteum
- Both regions contain antigen-presenting cells and dense sensory innervation
Lips
- Internal surface: nonkeratinized lining mucosa + labial salivary glands
- Vermilion zone: thin keratinized epithelium, richly vascularized (imparts the red color), no sweat or sebaceous glands - prone to dryness
- External surface: typical skin with hair follicles and sweat glands
- Core: striated muscle for mobility
Tongue
- Mass of striated muscle running in three planes, covered by mucosa; lamina propria penetrates between fascicles, making mucosa firmly adherent
- Lower surface: typical lining mucosa
- Dorsal surface: four types of lingual papillae:
| Papilla Type | Shape | Keratinization | Taste Buds | Special Features |
|---|---|---|---|---|
| Filiform | Elongated, conical | Heavily keratinized | None | Most numerous; aids food movement |
| Fungiform | Mushroom-shaped | Lightly keratinized | Scattered | Rich vascular/innervated cores |
| Foliate | Parallel ridges on tongue edges | Moderate | Present | Rudimentary in adult humans |
| Vallate (circumvallate) | Large (1-3 mm), surrounded by deep moat | Lightly keratinized | Very abundant (most taste buds) | 8-12 in V-shaped row; von Ebner serous glands drain into moat |
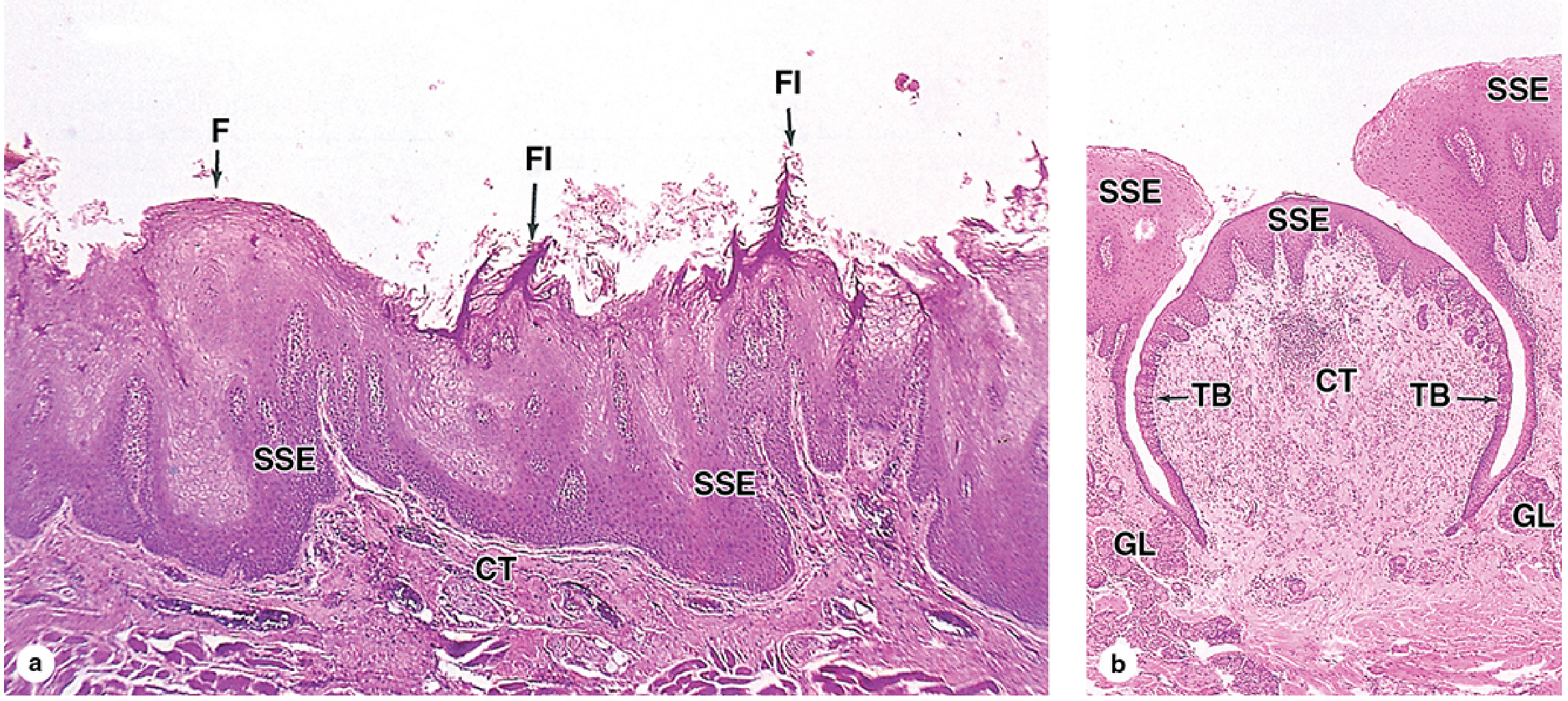
Taste buds: Barrel-shaped structures in stratified squamous epithelium; contain:
- Gustatory (taste) cells: microvilli projecting through apical taste pore; synapse with afferent sensory axons at base
- Supporting cells: poorly understood function
- Basal stem cells: regenerate gustatory and supporting cells
Teeth
- Enamel: covers crown and neck; the hardest tissue in the body; formed by ameloblasts (columnar epithelial cells of the enamel organ) which deposit parallel enamel rods guided by the protein amelogenin; ameloblasts are lost after tooth eruption - enamel cannot regenerate
- Dentin: makes up the roots and extends to the neck; secreted as predentin (with dentinal tubules) by tall odontoblasts lining the pulp cavity; odontoblast processes persist in tubules of the mature tooth
- Cementum: thin bone-like layer surrounding dentin of roots; part of the periodontium
- Periodontal ligament: binds cementum to alveolar bone
- Pulp cavity: vascularized and innervated central cavity lined by odontoblasts
III. Salivary Glands (Accessory Organs)
Three major paired glands produce approximately 1.5 L/day of saliva. All have secretory acini and a duct system.
| Gland | Acinar Type | Secretion | Key Feature |
|---|---|---|---|
| Parotid | Purely serous | Watery, enzyme-rich (amylase) | Largest; entirely serous acini |
| Submandibular | Mixed (serous + mucous) | Mixed | Serous cells form demilunes ("half-moons") capping mucous acini |
| Sublingual | Predominantly mucous | Viscous, mucin-rich | Smallest; few serous demilunes |
Acinar cells:
- Serous: pyramidal, basophilic cytoplasm (rER), apical zymogen granules; secrete amylase, lysozyme
- Mucous: columnar; pale cytoplasm (mucin granules displace nucleus basally); secrete mucins
Duct system (from lumen outward):
- Intercalated ducts: lined by low cuboidal epithelium; connect acini to striated ducts
- Striated (excretory) ducts: columnar cells with prominent basolateral plasma membrane infoldings and mitochondria (visible as striations); active in Na+ reabsorption and K+ secretion, making saliva hypotonic
- Interlobular ducts: larger; pseudostratified then stratified columnar epithelium
Myoepithelial cells: lie between acinar cells and basal lamina; stellate or basket-shaped; contract (via oxytocin/neurotransmitters) to expel secretion from acini
IV. Esophagus
- Epithelium: nonkeratinized stratified squamous - protects against abrasion
- Lamina propria: loose CT; contains esophageal cardiac glands near cardia (secrete mucus)
- Submucosa: esophageal glands proper (branched tubulo-acinar mucous glands) scattered along the entire length - produce lubricating mucus
- Muscularis:
- Superior third: striated muscle (under voluntary control)
- Middle third: mixed striated + smooth
- Inferior third: smooth muscle only
- Outer coat: adventitia along most of its length (no mesothelium), merging with mediastinal tissue; becomes serosa at the abdominal segment
- Esophagogastric junction: abrupt transition from stratified squamous to simple columnar epithelium; adventitia replaced by serosa
V. Stomach
Regions
Four regions; histologically: cardia + pylorus resemble each other; fundus + body are similar.
Wall layers
- Epithelium: simple columnar (surface mucous cells) lining the lumen and the gastric pits (foveolae gastricae)
- Surface mucous cells: secrete a thick gel of viscous mucus + bicarbonate ions, forming a protective unstirred layer
Gastric Glands (Fundus/Body)
The pits open into branching tubular gastric glands with five cell types:
| Cell Type | Location in Gland | Secretion / Function |
|---|---|---|
| Mucous neck cells | Narrow neck (isthmus) | Acid mucus; immature precursors of surface mucous cells |
| Parietal (oxyntic) cells | Upper-mid gland | HCl (via H+/K+ ATPase in intracellular canaliculi); intrinsic factor (for vitamin B12 absorption); very large cells with numerous mitochondria |
| Chief (zymogenic) cells | Lower half of gland | Pepsinogen (activated by low pH → pepsin, major protease); also gastric lipase |
| Enteroendocrine cells | Scattered throughout | Peptide hormones: gastrin (G cells, pylorus), somatostatin (D cells), histamine (enterochromaffin-like cells), serotonin |
| Stem cells | Neck (isthmus) region | Pluripotent; give rise to all above cell types; renew every 3-7 days |
Cardiac and Pyloric Regions
- Cardiac glands: branching tubular; almost entirely columnar mucous cells; absent parietal and chief cells
- Pyloric glands: similar; G cells (gastrin-secreting) abundant here
- Pyloric sphincter: prominent thickening of the inner circular smooth muscle
VI. Small Intestine
The key specialization is maximizing absorptive surface area through three structural levels: folds (plicae circulares), villi, and microvilli (brush border) - increasing surface area ~600-fold.
Three Regions
| Region | Key Histological Feature |
|---|---|
| Duodenum | Brunner (duodenal) glands in submucosa - branched tubulo-acinar; secrete alkaline mucus + bicarbonate to neutralize acidic chyme |
| Jejunum | Tallest villi (leaf-shaped); most developed plicae circulares |
| Ileum | Peyer's patches (large submucosal lymphoid nodules); shorter villi; M cells over follicles |
Mucosa
- Epithelium: simple columnar lining villi and crypts (intestinal glands / crypts of Lieberkühn)
- Villi: finger-like projections of epithelium over a lamina propria core containing capillaries, lymphatics, and a central lacteal (lymph capillary for fat absorption)
- Crypts of Lieberkühn: simple tubular glands between villi base; contain stem cells
Cell Types of the Intestinal Epithelium
| Cell | Location | Function |
|---|---|---|
| Enterocytes (absorptive cells) | Villi | Tall columnar; dense apical microvilli (brush border / glycocalyx); final digestion of carbohydrates and peptides; transcytosis of sugars, amino acids into capillaries |
| Goblet cells | Villi and crypts | Mucus secretion; increase in number from duodenum to colon |
| Paneth cells | Base of crypts | Pyramidal; apical eosinophilic granules; secrete defensins (antimicrobial peptides), lysozyme, TNF; regulate microbiome |
| Enteroendocrine cells | Crypts and villi | Secrete CCK, secretin, GIP, motilin, VIP, etc. |
| M (microfold) cells | Epithelium over Peyer's patches (ileum) | Antigen sampling; transport antigens to underlying lymphocytes |
| Stem cells | Lower crypt | Self-renewing; generate all villus cell types; turnover ~3-5 days |
Fat Absorption
Lipid digestion products associate with bile salts, are taken up by enterocytes, converted to triglycerides and lipoproteins, packaged as chylomicrons, and released into the lacteal for transport via lymph (not portal blood).
VII. Large Intestine (Colon)
- No villi - flat mucosal surface
- Epithelium: simple columnar
- Intestinal glands: millions of simple tubular crypts, lined by:
- Colonocytes (absorptive cells): absorb water and electrolytes
- Goblet cells: very abundant (more than in small intestine); produce copious mucus for lubrication of feces
- Lamina propria: rich in lymphocytes and plasma cells
- Muscularis: outer longitudinal layer condensed into three teniae coli (bands of smooth muscle visible externally); between the bands the wall bulges into haustra
- Serosa: covers the outer surface
- Appendix: blind-ending diverticulum of the cecum; thin mucosa with short crypts; abundant lymphoid nodules in lamina propria and submucosa (MALT organ)
VIII. Anal Canal
- Transition zone: simple columnar of rectum abruptly shifts to stratified squamous epithelium (at the pectinate/dentate line)
- Stratified squamous epithelium of the anal canal has no skin appendages, unlike the perianal skin below the anus
- Internal anal sphincter: thickening of the circular smooth muscle of the muscularis
- External anal sphincter: striated (skeletal) muscle under voluntary control
IX. Liver
The liver is the largest gland in the body. Its parenchymal cells (hepatocytes) are arranged in plates radiating from central veins.
Structural Organization
Classic hepatic lobule: Hexagonal unit centered on a central vein (terminal hepatic venule); at each corner sits a portal triad (portal vein branch, hepatic artery branch, bile ductule).
- Blood flows from portal triads inward to the central vein (portal → sinusoids → central vein)
- Bile flows outward from hepatocytes → bile canaliculi → canal of Hering → interlobular bile ducts in portal triads
Hepatocytes
- Large polygonal cells; one or two round nuclei (often polyploid); abundant rER, sER, Golgi, mitochondria, and glycogen
- Arranged in hepatic plates (1-2 cells thick) that radiate from central vein to portal tracts
- Secretion: bile (exocrine) and plasma proteins - albumin, clotting factors, lipoproteins (endocrine)
Sinusoids
- Wide, fenestrated capillaries lined by sinusoidal endothelial cells (with large fenestrae, no diaphragm or basal lamina) between hepatic plates
- Space of Disse: narrow perisinusoidal space between endothelium and hepatocytes; contains hepatic stellate cells (Ito cells/lipocytes) - normally store vitamin A as lipid droplets; activated in injury they produce collagen (fibrosis/cirrhosis)
- Kupffer cells: resident macrophages lining sinusoids; phagocytose bacteria, debris, old erythrocytes
Bile Canaliculi
- Tiny grooves between adjacent hepatocytes formed by specialized apical membrane domains sealed by tight junctions
- Not separate ducts - simply modified intercellular space
- Bile flows toward portal triads → enters bile ductules (canal of Hering, lined by cholangiocytes)
Portal Triad Contents
- Branch of portal vein (largest, thin wall)
- Branch of hepatic artery (thicker wall, smaller lumen)
- Bile ductule (simple cuboidal epithelium / cholangiocytes)
- Lymphatic vessels and autonomic nerves
X. Gallbladder
- Mucosa: simple columnar epithelium with tall cells having apical microvilli; highly folded into irregular rugae (especially when contracted/empty); lamina propria with no glands (except near neck)
- Muscularis: irregularly arranged smooth muscle bundles (no distinct layers)
- Perimuscular connective tissue: replaces submucosa; contains nerves, vessels
- Serosa/adventitia: upper (hepatic) surface is adventitia; free surface is serosa
- Rokitansky-Aschoff sinuses: invaginations of the epithelium through the muscularis into the perimuscular connective tissue - become more pronounced in chronic cholecystitis
- Function: concentrates and stores bile by actively absorbing Na+, Cl-, and water from bile
XI. Pancreas
The pancreas is a mixed exocrine-endocrine gland.
Exocrine Pancreas (~99% of mass)
- Acinar cells: pyramidal; arranged in grape-like acini
- Basophilic base (abundant rER for enzyme synthesis)
- Apical zymogen granules (eosinophilic): contain digestive enzyme precursors (trypsinogen, chymotrypsinogen, proelastase, lipase, amylase)
- Release enzymes into acinar lumen by exocytosis, stimulated by CCK and vagal input
- Centroacinar cells: flattened pale cells that extend from duct epithelium into the acinar lumen; secrete bicarbonate-rich fluid (stimulated by secretin)
- Duct system: intercalated ducts → interlobular ducts → main pancreatic duct
Endocrine Pancreas - Islets of Langerhans (~1% of mass)
- Compact, pale-staining spherical clusters scattered within the exocrine tissue; well vascularized
- Cell types:
| Cell | Hormone | Location in Islet | Function |
|---|---|---|---|
| Beta (B) cells | Insulin | Central (majority, ~70%) | Lowers blood glucose; promotes glycogen, fat, protein synthesis |
| Alpha (A) cells | Glucagon | Peripheral (~20%) | Raises blood glucose; promotes glycogenolysis, gluconeogenesis |
| Delta (D) cells | Somatostatin | Scattered (~5%) | Inhibits both insulin and glucagon release |
| PP (F) cells | Pancreatic polypeptide | Peripheral (~5%) | Inhibits pancreatic exocrine secretion |
Summary Table: Epithelial Types at a Glance
| Organ / Region | Epithelium Type |
|---|---|
| Oral cavity (cheeks, floor, soft palate) | Nonkeratinized stratified squamous |
| Hard palate, gingiva | Keratinized stratified squamous |
| Esophagus | Nonkeratinized stratified squamous |
| Stomach | Simple columnar (mucous) |
| Small intestine | Simple columnar with brush border |
| Large intestine | Simple columnar (predominantly goblet cells) |
| Anal canal (below dentate line) | Stratified squamous |
| Gallbladder | Simple columnar (absorptive) |
| Bile ducts (interlobular) | Simple cuboidal (cholangiocytes) |
| Liver parenchyma | Hepatocytes (polyhedral glandular) |
| Pancreas acini | Simple pyramidal (serous) |
Source: Junqueira's Basic Histology: Text and Atlas, 17th edition; Yamada's Textbook of Gastroenterology, 7th edition; Sleisenger and Fordtran's Gastrointestinal and Liver Disease.
This is a shared conversation. Sign in to Orris to start your own chat.