What is stroke volume
Reading File
Finding Sources
Searching the Web
stroke volume physiology determinants normal values
Reading File
Reading File
Loading Image
Reading File
Here is a thorough explanation of stroke volume, drawn from authoritative physiology and anesthesiology textbooks.
Stroke Volume
Stroke volume (SV) is the volume of blood ejected by the left ventricle during a single contraction (systole). It is simply the difference between two ventricular volumes:
SV = End-Diastolic Volume (EDV) - End-Systolic Volume (ESV)
- End-Diastolic Volume (EDV): the amount of blood in the ventricle just before it contracts (~120 mL)
- End-Systolic Volume (ESV): the amount of blood remaining after contraction (~50 mL)
- Typical SV at rest: ~70 mL
(Costanzo Physiology 7th Edition, p. 155)
Ejection Fraction
A related measure is the ejection fraction (EF), which expresses how efficiently the ventricle ejects its contents:
EF = SV / EDV
Normally ~55-65%. A falling ejection fraction signals reduced contractility (as seen in heart failure).
Cardiac Output
Stroke volume is multiplied by heart rate to give cardiac output:
Cardiac Output = SV × Heart Rate
At rest in a 70-kg man: 70 mL × 72 beats/min ≈ 5,000 mL/min (5 L/min)
The Three Major Determinants of Stroke Volume
According to Morgan and Mikhail's Clinical Anesthesiology, stroke volume is governed by three factors:
| Factor | Definition | Effect on SV |
|---|---|---|
| Preload | Ventricular end-diastolic volume (degree of fiber stretch before contraction) | More preload → more SV (up to a limit) |
| Afterload | Resistance the ventricle must overcome to eject blood (aortic impedance / wall stress) | More afterload → less SV |
| Contractility | Intrinsic force of myocardial contraction, independent of preload and afterload | More contractility → more SV |
Additional factors that can affect SV include wall motion abnormalities and valvular dysfunction.
Preload and the Frank-Starling Law
Preload is primarily determined by venous return. As end-diastolic volume increases, cardiac muscle fibers are stretched, which increases the force of contraction and therefore SV. This is the Frank-Starling Law of the Heart - the strength of contraction depends on initial fiber length.
The graph below (from Starling's original work, as reproduced in Morgan & Mikhail) shows how cardiac output varies with ventricular end-diastolic volume under different contractile states:
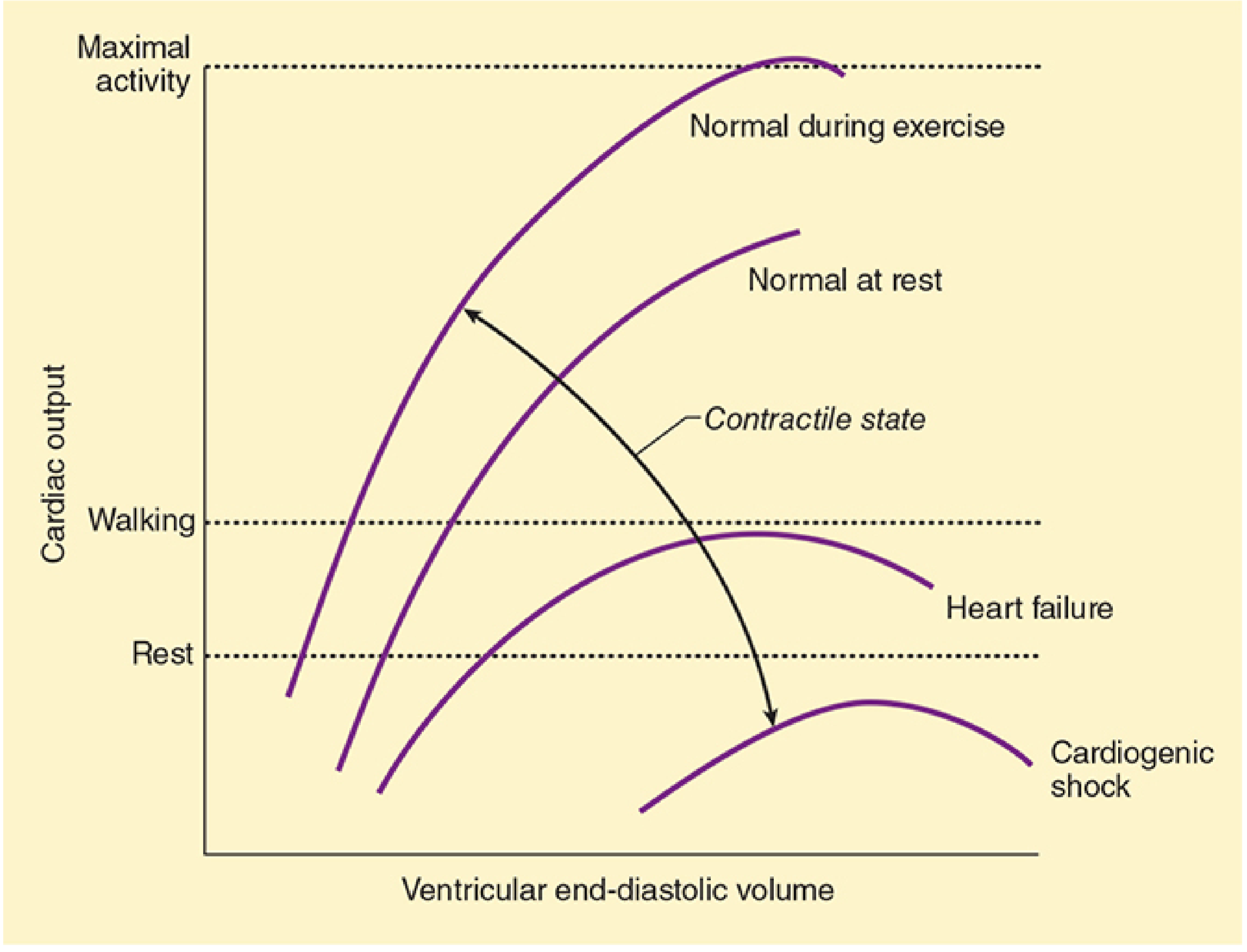
- The upper curves (exercise, normal at rest) reflect higher contractility
- The lower curves (heart failure, cardiogenic shock) reflect depressed contractility
- Each curve peaks and can decline at very high EDV (ventricular overdistension)
Factors Affecting Preload
(Morgan & Mikhail's Clinical Anesthesiology, p. 658)
- Blood volume
- Distribution of blood volume (posture, venous tone)
- Intrathoracic pressure (e.g., positive-pressure ventilation reduces venous return)
- Pericardial pressure
- Heart rate and rhythm (atrial contraction contributes 20-30% of filling)
Quick Reference: Sample Calculation
A patient with EDV = 140 mL, ESV = 70 mL, HR = 75 beats/min:
- SV = 140 - 70 = 70 mL
- Cardiac Output = 70 × 75 = 5,250 mL/min
- Ejection Fraction = 70/140 = 50%
(Costanzo Physiology 7th Edition, p. 155)
This is a shared conversation. Sign in to Orris to start your own chat.