Ludwig angina
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Ludwig angina" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough answer on Ludwig's angina.
Ludwig's Angina
Definition and Historical Note
Ludwig's angina is a rapidly progressive, bilateral, gangrenous cellulitis involving all three primary mandibular spaces (bilateral sublingual and bilateral submandibular spaces). It was first described by Wilhelm Friedrich von Ludwig in 1836. Before antibiotics it was a common, frequently fatal condition. The name "angina" comes from the Latin for "choking" - reflecting its most feared complication.
- Rosen's Emergency Medicine, p. 961
- Cummings Otolaryngology, p. 204
Anatomy - Why It Is Always Bilateral
The key to understanding why this infection is inherently bilateral lies in the anatomy of the floor of the mouth:
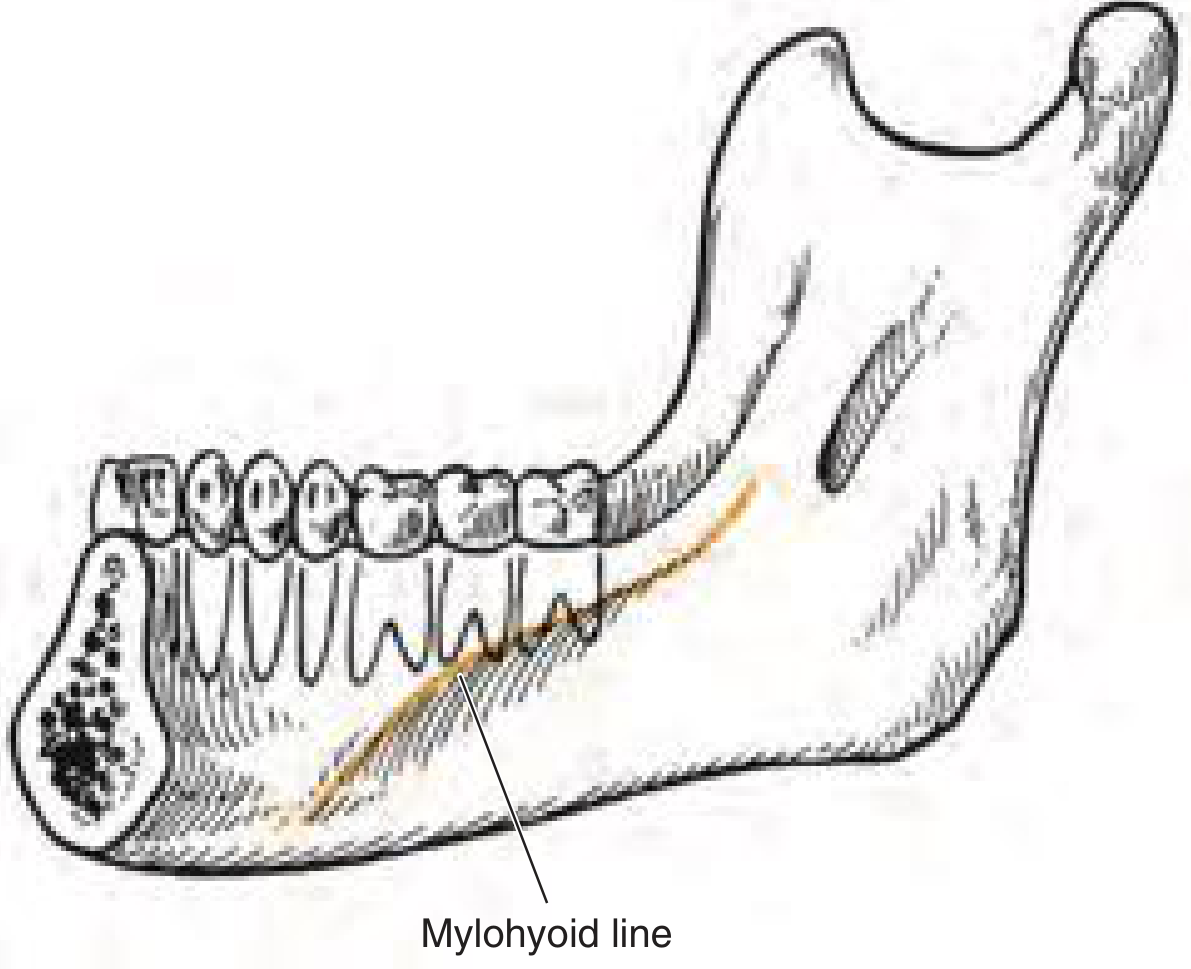
The mylohyoid line: infections above this line involve the sublingual space; below it, the submandibular space.
- The sublingual space lies between the lingual mucosa and the mylohyoid muscle; its posterior boundary is open, communicating freely with the submandibular space.
- The submandibular space lies between the mylohyoid and the skin; it too has an open posterior boundary.
- Because both spaces communicate posteriorly, infection spreads bilaterally through these open fascial planes - NOT via lymphatics.
- When all three primary mandibular spaces bilaterally become infected, the result is Ludwig's angina.
The space involvement by tooth level:
- Premolars and first molar (apex superior to mylohyoid) → sublingual space
- Second and third molars (apex inferior to mylohyoid) → submandibular space
Etiology / Causes
| Cause | Notes |
|---|---|
| Mandibular molar dental infection | Most common (80%+); apices of 2nd/3rd molars dip below the mylohyoid muscle |
| Mandibular fracture | Direct communication across fascial planes |
| Oral trauma | Tongue piercing, lingual laceration, iatrogenic (e.g., intubation trauma) |
| Secondary infection of oral malignancy | |
| Suppurative parotitis | |
| Adjacent head and neck infections |
Risk factors: Immunocompromised patients and diabetics are at higher risk.
Spread can occur posteriorly between the submandibular and parapharyngeal spaces via the styloglossus muscle, leading to deep neck infections.
Microbiology
The infection is typically polymicrobial:
- Virulent Streptococcus species (most common)
- Gram-negative rods
- Anaerobes (which contribute to the gangrenous character)
Clinical Features
The classic presentation ("bull neck"):

Symptoms:
- Recent dental caries, infection, or dental procedure
- Progressive pain and swelling of the floor of mouth
- Dysphagia and odynophagia
- Drooling (unable to manage secretions)
- Muffled ("hot potato") voice
- Fever
- Neck stiffness
Signs:
- Submental and submandibular swelling with tongue protrusion
- Elevation of floor of mouth
- Woody induration on palpation (characteristic - NOT fluctuant)
- Tense brawny edema from submandibular region to hyoid - the "bull neck"
- Putrid halitosis
- Cervical adenopathy and fluctuation are usually absent (this is cellulitis, not abscess)
Late/alarming signs (impending airway compromise):
- Trismus
- Dyspnea and tachypnea
- Stridor
- Hoarse voice
- Progressive anxiety
Diagnosis
Clinical diagnosis - imaging is not required for diagnosis and patients may not tolerate lying supine.
- Contrast-enhanced CT scan can help identify:
- The deep neck structures involved
- Extent of infection
- Any abscess collection (rare but important if present)
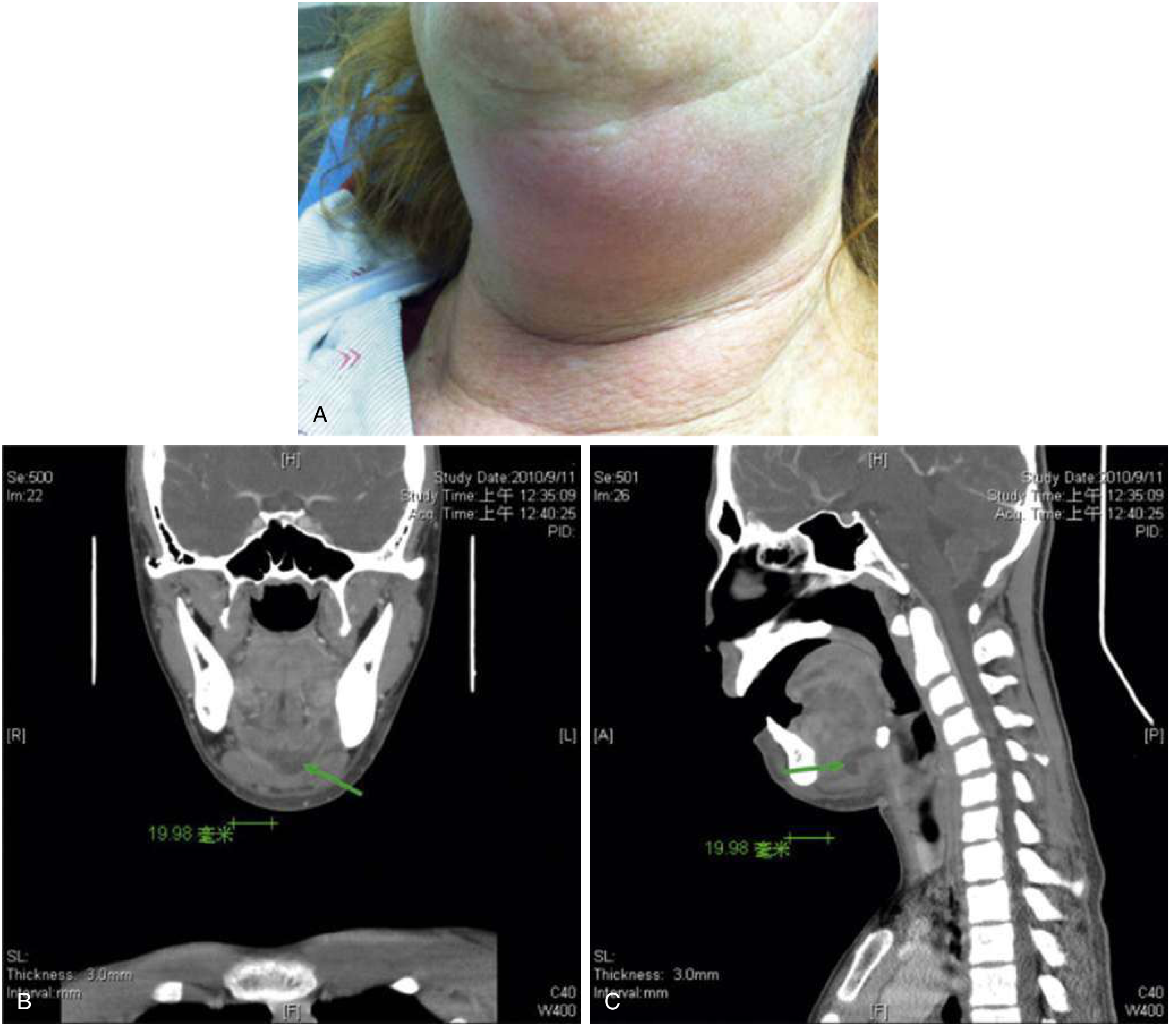
Coronal and sagittal CT demonstrating the extent of submandibular and sublingual space involvement.
Differential Diagnosis
- Pharyngeal or retropharyngeal abscess
- Parotid or submandibular gland abscess
- Parapharyngeal abscess
- Sublingual hematoma
- Glossal/posterior oropharyngeal angioedema
- Oropharyngeal tumors
- Laryngeal diphtheria
Management
1. Airway (FIRST PRIORITY)
Asphyxia from progressive edema is the leading cause of death. Airway management takes precedence over everything else.
Indications for airway intervention: dyspnea, tachypnea, inability to manage secretions, agitation, stridor, progressive edema.
- Preferred: Awake fiberoptic nasal or oral intubation with a flexible bronchoscope after adequate topicalization
- Oral laryngoscopy may be impossible due to edema and tongue displacement
- Do NOT paralyze prior to securing the airway - this removes the patient's only protective reflexes
- Surgical airway (tracheostomy): May be required if endotracheal intubation fails; more challenging in Ludwig's due to anterior neck distortion from edema and risk of spreading infection. It is the safest approach when severe edema makes the view impossible.
2. IV Antibiotics
Broad-spectrum coverage including anaerobes:
| Antibiotic | Dosage | Notes |
|---|---|---|
| Ampicillin/sulbactam + vancomycin | 3 g IV q6h + 15-20 mg/kg q8-12h (max 2 g) | First-line |
| Clindamycin | 600 mg IV q8h | Penicillin allergy |
| Meropenem + vancomycin | 1 g IV q8h + 20 mg/kg (max 2 g) | Immunocompromised |
- Rosen's Emergency Medicine, p. 962
3. Surgical Intervention
Usually NOT required - antibiotic therapy is usually sufficient. Indications for surgery:
- Infected tooth extraction
- Debridement of necrotizing infection
- Drainage of purulent (pus) collections
- Persistent or progressive infection despite antibiotics
Surgical approach: Curved submental incision to drain both submandibular triangles; the mylohyoid muscle may be incised to decompress the floor of mouth; corrugated drains placed. Rarely, tracheostomy.
- Bailey & Love's Surgery, p. (block7)
- Scott-Brown's ENT, Vol. 2
4. Disposition
ICU admission is mandatory for all patients with Ludwig's angina.
Complications
- Airway obstruction / asphyxia - the primary killer
- Spread to parapharyngeal space → mediastinitis (descending necrotizing mediastinitis)
- Septicemia / septic shock
- Aspiration pneumonia
- Glottic edema from laryngeal involvement
- Cavernous sinus thrombosis (spread from adjacent structures)
Key Summary Points (KJ Lee's Otolaryngology)
- Severe infection of the sublingual and submental spaces
- High mortality from asphyxia
- Most commonly dental in origin
- Rapid spread through fascial planes (NOT lymphatics)
- Swelling causes posterior tongue displacement and airway obstruction
- Classic presentation: erect, drooling patient with edema of tongue and floor of mouth; woody, indurated neck
- Airway management is first priority (tracheotomy vs. awake fiberoptic intubation)
- Wide drainage of bilateral submandibular and sublingual spaces if needed
- IV antibiotic therapy with anaerobic coverage
This is a shared conversation. Sign in to Orris to start your own chat.