Grades of atelectasis and its management
Reading File
Finding Sources
Finding Sources
Searching PubMed
atelectasis classification management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
grades of atelectasis radiological classification postoperative management
Reading File
Reading Web Page
https://publishingimages.s3.amazonaws.com/eZineImages/Practi…
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Atelectasis: Grades (Types) and Management
Atelectasis (from Greek: ateles = incomplete + ektasis = expansion) is the loss of lung volume due to collapse of lung tissue. It is the most common respiratory complication in postoperative patients and can affect an entire lung, a lobe, a segment, or a subsegment.
Classification / "Grades" of Atelectasis
Atelectasis is classified in three overlapping ways: by pathophysiologic mechanism, by anatomical extent (which reflects clinical severity), and by radiographic pattern.
A. By Pathophysiologic Mechanism
| Type | Mechanism | Common Causes |
|---|---|---|
| Obstructive (Resorptive) | Airway blockage - gas distal to the obstruction is resorbed | Mucus plugs, foreign bodies, endobronchial tumors, external lymph node compression |
| Compressive (Passive / Relaxation) | Lung recoils inward due to adjacent pleural space process | Pleural effusion, pneumothorax, elevated hemidiaphragm |
| Adhesive | Alveolar instability from surfactant deficiency | ARDS, RDS of newborn, post-anesthesia |
| Cicatrization | Fibrotic contraction of lung parenchyma | Granulomatous disease (TB, sarcoid), radiation fibrosis |
| Replacement | Alveolar filling by cells or fluid | Tumor, infection, hemorrhage |
| Rounded (Folded Lung / Blesovsky's syndrome) | Pleural thickening invaginates and traps adjacent lung | Asbestos-related pleural disease, any chronic pleural disease |
- Goldman-Cecil Medicine, p. 918
B. By Anatomical Extent (Severity Grades)
This is the most clinically used grading system - ranked from least to most severe:
| Grade | Extent | Radiographic Finding | Clinical Significance |
|---|---|---|---|
| 1 - Subsegmental (Plate-like / Discoid / Linear) | Sub-segment only | Horizontal or curvilinear lines on CXR, often fleeting | Usually asymptomatic; very common postoperatively |
| 2 - Segmental | One bronchopulmonary segment | Triangular density, mild volume loss | May cause mild hypoxemia |
| 3 - Lobar | Entire lobe | Lobar consolidation, fissure displacement, mediastinal shift | Significant hypoxemia; often requires active treatment |
| 4 - Whole Lung | Entire lung | Complete opacification of hemithorax, massive mediastinal shift toward collapsed side | Severe respiratory failure; emergency management required |
- Tintinalli's Emergency Medicine, p. 1756; Goldman-Cecil Medicine, p. 918
C. By Radiographic Pattern
- Plate-like (linear/discoid): Horizontal lines, usually in lower zones; most common postoperative type
- Triangular density: Segmental involvement; base toward pleura
- Lobar consolidation: Dense opacification with fissure or mediastinal shift
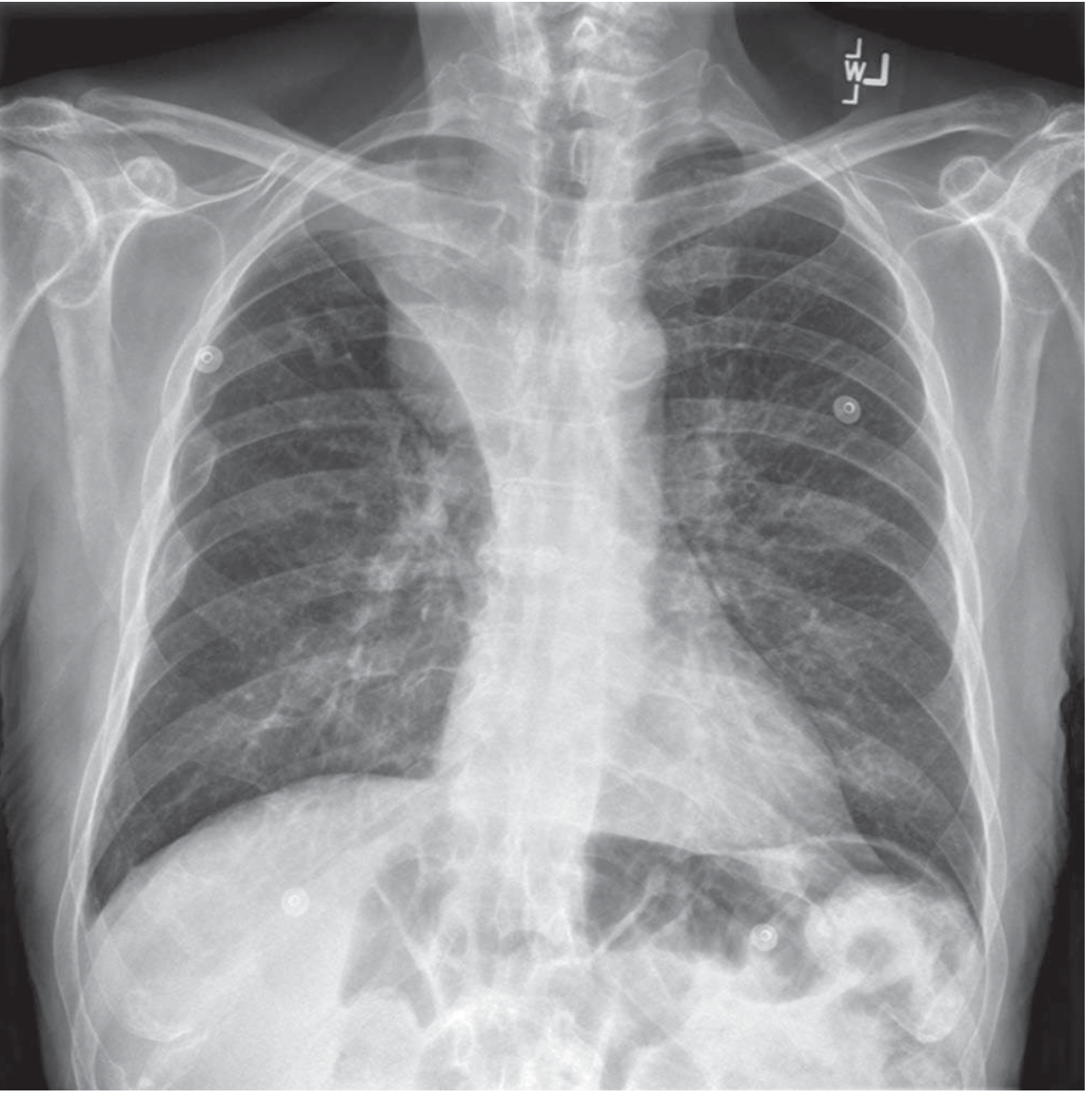
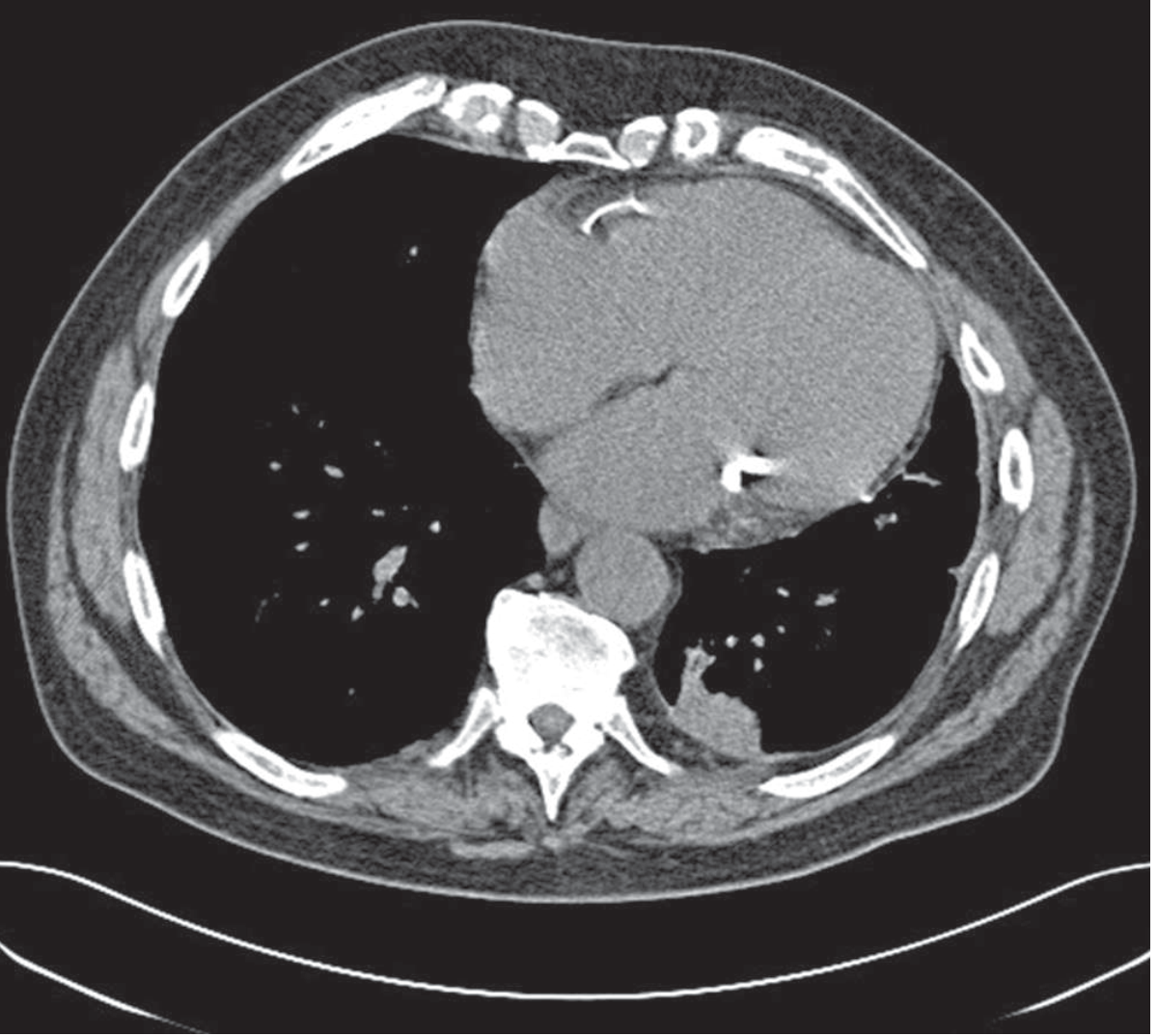
- Rounded atelectasis: Ovoid masslike density abutting the pleura - can mimic a tumor (important to distinguish via CT)
CXR - Right upper lobe atelectasis (endobronchial tumor):
CT - Rounded atelectasis:
Pathophysiology (Key Points)
-
Lung bases and posterior segments are most vulnerable due to dependent positioning
-
Anesthesia reduces FRC, impairs mucociliary clearance, and causes V/Q mismatch
-
Rapid, shallow breathing produces small airway closure with inspissated secretions, leading to alveolar air resorption
-
The result is hypoxemia (V/Q mismatch and shunt) proportional to the extent of atelectasis
-
Fever in the first 24-48 hours postoperatively is often attributed to atelectasis, though evidence for this association is debated
-
Barash Clinical Anesthesia, p. 3267; Sabiston Surgery, p. 446
Management
Management is tailored to the type and severity.
1. Prevention (Perioperative)
| Measure | Mechanism |
|---|---|
| Incentive spirometry | Increases tidal volume and FRC |
| Deep breathing exercises (5 sequential breaths, held 5-6 s) | Re-expands collapsed alveoli |
| Early ambulation and mobilization | Reduces dependent atelectasis |
| Adequate analgesia (multimodal - paracetamol + NSAIDs + regional blocks) | Reduces splinting and promotes deep breathing |
| Epidural analgesia (thoracic) | Shown to reduce atelectasis and pneumonia after thoracotomy |
| Chest physiotherapy | Clears secretions |
| Preoperative inspiratory muscle training | Reduces post-cardiac/upper abdominal surgery atelectasis |
| Oral care (ICOUGH protocol) | Reduces colonization, lowers pneumonia risk |
| Head-of-bed elevation | Prevents compression from abdominal contents |
2. Treatment by Grade
Subsegmental / Plate-like Atelectasis (Grade 1)
- Usually resolves spontaneously
- Deep breathing exercises, incentive spirometry, coughing
- Adequate pain control
- Mild hypoxemia: supplemental O2 via nasal cannula
- May manage as outpatient if no hypoxemia and no underlying disease
- Tintinalli's Emergency Medicine
Segmental / Lobar Atelectasis (Grades 2-3)
- Hospital admission if debilitated, underlying lung disease, or hypoxemia present
- Chest physiotherapy + bronchodilators
- CPAP / bilevel positive airway pressure (BiPAP) - increases transpulmonary pressure, expands alveoli
- Positioning: lateral decubitus with the healthy lung dependent (improves matching, facilitates mucus clearance from the obstructed lung)
- Exception: Do NOT place operative side down after pneumonectomy (risk of cardiac herniation)
- Bronchoscopy for mucus plugging not responding to physiotherapy
- Mechanical ventilation (increases airway pressure and transpulmonary pressure) if respiratory failure
- Goldman-Cecil Medicine, p. 918; Barash Clinical Anesthesia, p. 3267
Whole-Lung / Massive Atelectasis (Grade 4)
- Urgent bronchoscopy - both diagnostic (intrinsic vs. extrinsic obstruction) and therapeutic (mucus plug removal)
- Mechanical ventilation with PEEP
- Treat the underlying cause (tumor, foreign body, effusion drainage)
- Multiple bronchoscopies may be required for retained secretions, though mucus often reaccumulates until overall status improves
3. Treatment by Type
| Type | Specific Treatment |
|---|---|
| Obstructive / Resorptive | Bronchoscopy to remove obstruction (mucus plug, foreign body); treat endobronchial tumor |
| Compressive | Drain the pleural space (thoracocentesis for effusion, chest tube for pneumothorax) |
| Patchy / Adhesive | Treat underlying lung parenchymal disease (e.g., ARDS management, surfactant in neonates) |
| Rounded | No treatment required; CT to distinguish from malignancy |
| Cicatrization | Treat underlying fibrotic disease; surgical resection only if persistently symptomatic with good remaining lung function |
4. In Cystic Fibrosis
- Vigorous chest physiotherapy + antibiotics - often successfully re-expands the affected lung
- Bronchoscopy if physiotherapy fails (though not more effective than physiotherapy overall)
- Surgical resection of a persistently atelectatic/bronchiectatic lobe only if: remaining lung is in good condition, overall pulmonary function is adequate, and the affected segment is causing intolerable symptoms
- Fishman's Pulmonary Diseases, p. 1313
Key Diagnostic Points
| Modality | Findings |
|---|---|
| CXR | Loss of lung volume, fissure/mediastinal/diaphragm displacement toward involved lung; plate-like linear densities; air bronchograms |
| CT | More sensitive; shows cause (tumor, effusion, mucus plug); distinguishes rounded atelectasis from neoplasm |
| Bedside ultrasound | Confirms diagnosis; especially useful ICU/bedside |
| Pulse oximetry / ABG | SpO2 ≤96% on Venturi mask O2 after 30 min is moderately sensitive/specific for postoperative atelectasis |
| Bronchoscopy | Confirms intrinsic vs. extrinsic obstruction; defines exact pathology |
Sources: Goldman-Cecil Medicine 25e, p. 918 | Sabiston Textbook of Surgery 21e, p. 446 | Barash Clinical Anesthesia 9e, p. 3267 | Tintinalli's Emergency Medicine, p. 1756 | Fishman's Pulmonary Diseases and Disorders, p. 1313
Grades of atelectasis of ear and its management
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.