Treatment for IBS d type
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome" AND "diarrhea" AND treatment
Searching the Web
IBS-D treatment guidelines 2025 2026
Reading File
Finding Sources
Reading Web Page
https://www.aafp.org/afp/2023/1100/practice-guidelines-irrit…
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced answer.
Treatment of IBS-D (Diarrhea-Predominant IBS)
IBS-D is diagnosed using Rome IV criteria after excluding alarm symptoms. Up to 40% of IBS cases are the diarrhea-predominant subtype. Treatment targets abdominal pain, stool frequency/consistency, and urgency.
1. Non-Pharmacologic Measures (First-Line)
- Low-FODMAP diet - reduces fermentable carbohydrates that trigger symptoms
- Psychosocial modifications - cognitive-behavioral therapy, gut-directed hypnotherapy
- Regular exercise - shown to reduce GI symptom burden
- Avoid triggers - caffeine, fatty foods, alcohol, dairy (lactose)
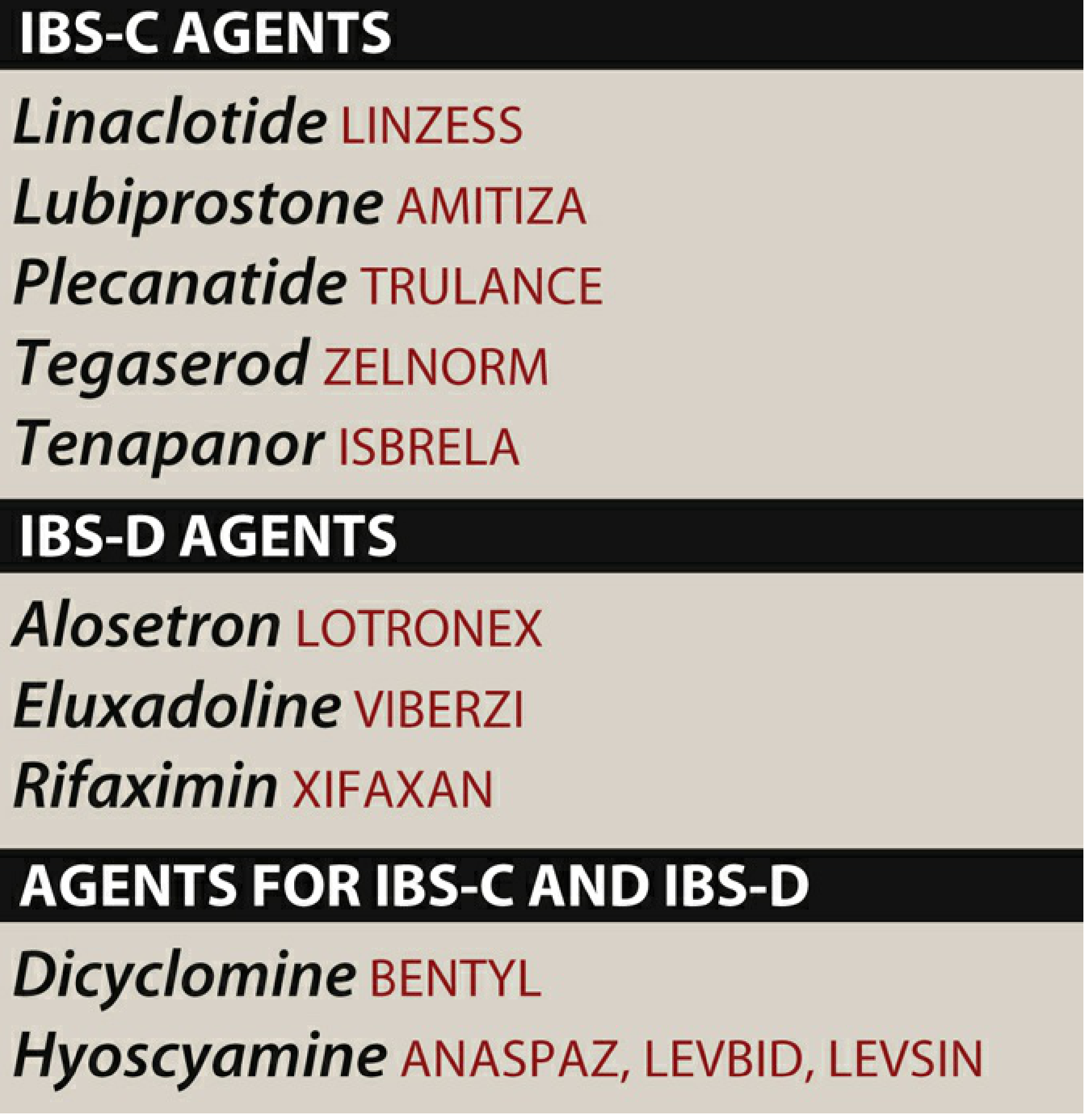
2. IBS-D-Specific Pharmacologic Agents
Rifaximin (Xifaxan)
- Mechanism: Non-absorbable antibiotic (structural analog of rifampin); reduces intraluminal bacterial load and gas production
- Use: Short-term treatment of IBS-D; 550 mg TID x 14 days - can be repeated for recurrent symptoms
- Efficacy: Improves global discomfort, bloating, stool consistency, and abdominal pain
- Safety: Adverse effects (nausea, fatigue, headache) are not significantly different from placebo; small risk of C. difficile infection
- Key point (AGA guideline): First-line IBS-D-specific drug recommended by AGA
Alosetron (Lotronex)
- Mechanism: Highly potent, selective 5-HT3 receptor antagonist - blocks serotonin receptors on enteric afferents and cholinergic neurons, slows left colonic transit, reduces visceral pain and urgency
- Use: Women only with severe IBS-D who have failed conventional therapies
- Dose: 0.5-1 mg once or twice daily
- Efficacy: ~50-60% adequate relief vs. 30-40% placebo; reduces bowel frequency, urgency, and pain
- Adverse effects:
- Constipation in up to 30% (discontinuation in 10%)
- Ischemic colitis (up to 3 per 1,000 patients, some fatal)
- Serious constipation requiring hospitalization in 1 per 1,000
- Restriction: Prescribed only through a Risk Evaluation and Mitigation Strategy (REMS) program
Eluxadoline (Viberzi)
- Mechanism: Mixed mu-opioid (μ) receptor agonist / delta-opioid antagonist - acts locally in the gut to reduce motility and secretion without significant CNS effects
- Use: IBS-D in both men and women
- Dose: 75 mg or 100 mg BID with food
- Efficacy: Reduces diarrhea, abdominal pain, and urgency
- Adverse effects: Constipation, abdominal pain, nausea
- Serious risk: Pancreatitis (rare but potentially severe)
- Contraindications: History of pancreatitis, biliary duct obstruction, severe hepatic impairment, cholecystectomy (sphincter of Oddi spasm risk), alcohol use disorder
3. General Agents Used in IBS-D
| Drug | Mechanism | Notes |
|---|---|---|
| Loperamide | Peripheral μ-opioid agonist; inhibits peristalsis, reduces secretion, prolongs transit | Very low-quality evidence but widely used; improves stool consistency and urgency; does NOT cross BBB |
| Tricyclic antidepressants (amitriptyline, desipramine 10-50 mg/d) | Central processing of visceral afferents; anticholinergic effects reduce stool frequency | Useful for chronic abdominal pain; effective at sub-antidepressant doses; evidence is low quality |
| Antispasmodics (dicyclomine, hyoscyamine) | Antimuscarinic - reduce GI spasms | Short-term relief of abdominal cramps; long-term efficacy not convincingly established; anticholinergic side effects at higher doses |
4. Agents NOT Recommended in IBS-D
- SSRIs - do not improve global IBS-D symptoms or abdominal pain
- Polyethylene glycol (PEG) - not effective for IBS pain
- Fiber supplements - may worsen bloating in IBS-D
5. Quick Reference: AGA Guideline Highlights (2023)
| Drug | AGA Recommendation |
|---|---|
| Rifaximin | Suggested for IBS-D (improves discomfort, bloating) |
| Alosetron | Suggested for women with severe IBS-D only (REMS required) |
| Eluxadoline | Suggested; avoid in cholecystectomy / alcohol use |
| Loperamide | Very low quality evidence; suggested for stool consistency |
| TCAs | Suggested for global symptoms/pain |
| Antispasmodics | Conditionally suggested for abdominal pain |
AGA FDA responder definition: At least 30% reduction in average daily worst abdominal pain AND ≥50% reduction in days per week with Bristol type 6 or 7 stool.
Recent Evidence
A 2026 systematic review and meta-analysis on IBS pharmacotherapy safety (PMID: 40471839) confirmed that most IBS-D drugs have acceptable safety profiles, with eluxadoline and alosetron carrying the most serious adverse event risks. A 2023 network meta-analysis (PMID: 37686889) found specific probiotic strains may offer modest benefit for IBS symptoms including diarrhea predominant subtypes.
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed., pp. 1713-1714 | Lippincott Illustrated Reviews: Pharmacology, p. 1441-1442 | AGA Clinical Practice Guidelines (summarized via AAFP 2023)
This is a shared conversation. Sign in to Orris to start your own chat.