Pathogenesis of nephrotic syndrome according to book ramdasnaik
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information on the pathogenesis of nephrotic syndrome. Before responding, I should note that the book "Ramdasnaik" (likely referring to "Pathology" by Ramdas Naik or a similar Indian medical textbook) is not available in this library. However, the pathogenesis as described in standard textbooks is consistent. Let me now provide a thorough, well-structured answer.
Note: The book "Ramdasnaik" (Ramdas Naik's Pathology) is not available in this textbook library. The content below is drawn from Comprehensive Clinical Nephrology, 7th Edition and Brenner and Rector's The Kidney — the standard nephrology references — and reflects the same pathogenesis content taught in Indian medical curricula textbooks on this topic.
Pathogenesis of Nephrotic Syndrome
Core Defect: Glomerular Barrier Dysfunction
The fundamental defect in nephrotic syndrome is disruption of the glomerular filtration barrier, which normally restricts proteins (especially albumin) from passing into the filtrate. This barrier consists of three layers:
- Fenestrated glomerular endothelium — negatively charged, repels anionic proteins
- Glomerular basement membrane (GBM) — type IV collagen, laminin, heparan sulfate (negative charge)
- Podocytes (visceral epithelial cells) — foot processes linked by the slit diaphragm (nephrin, podocin)
Injury to any of these layers — particularly the podocyte foot processes and the slit diaphragm — leads to massive proteinuria (>3.5 g/day in adults).
Consequences of Proteinuria
1. Hypoalbuminaemia
Urinary loss of albumin exceeds hepatic synthetic capacity → serum albumin falls below 3 g/dL.
2. Oedema Formation — Two Theories
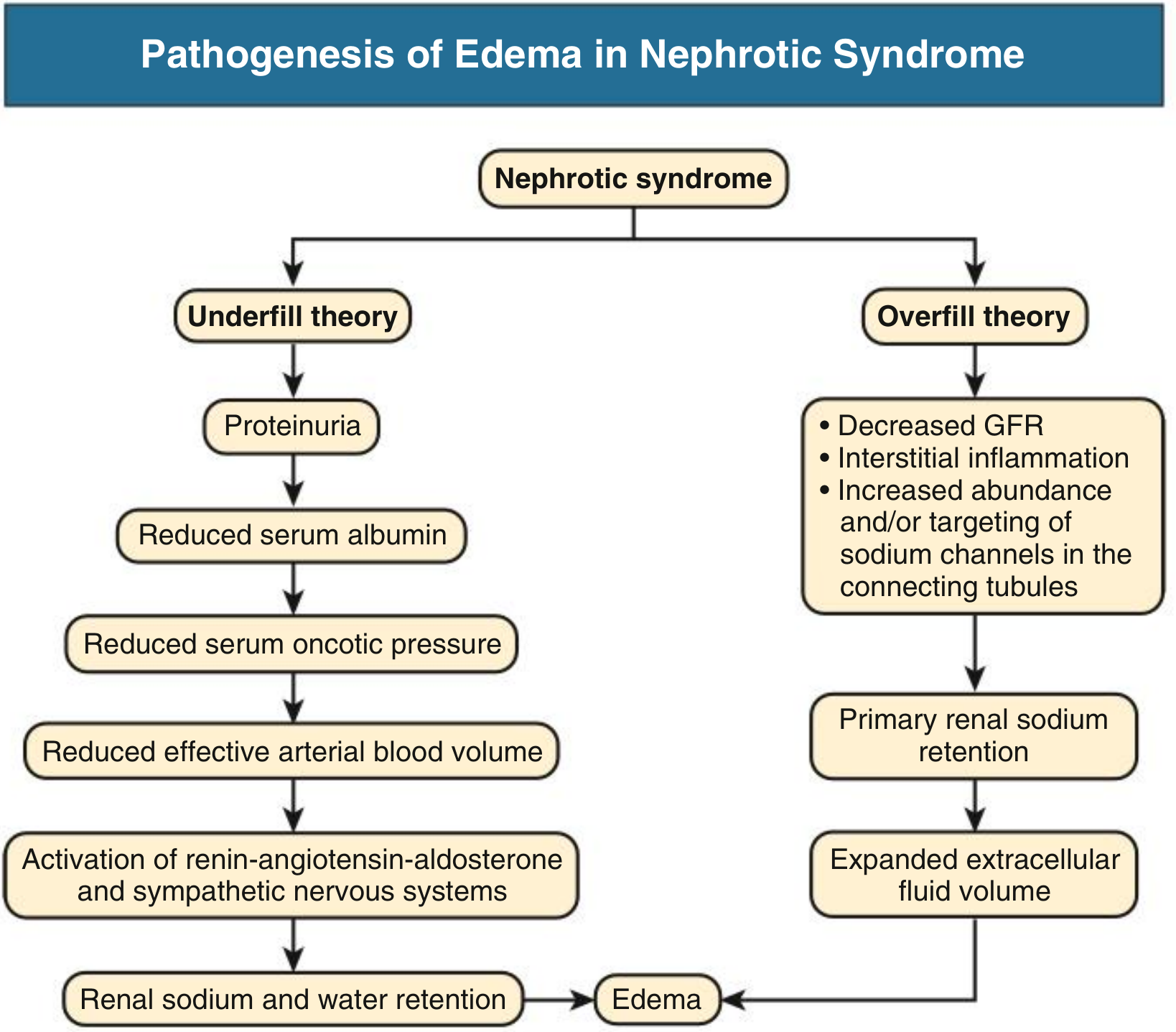
A. Underfill Theory (classical)
- Proteinuria → ↓ serum albumin → ↓ plasma oncotic pressure
- Fluid shifts from intravascular → interstitial compartment (Starling forces)
- ↓ Effective arterial blood volume (EABV) → activates:
- Renin-Angiotensin-Aldosterone System (RAAS) → Na⁺ and water retention
- Sympathetic Nervous System (SNS) → renal vasoconstriction
- ADH → water retention
- This leads to renal Na⁺/water retention → worsens oedema
- More common in Minimal Change Disease (MCD) with severe hypoalbuminaemia (<2 g/dL), normal/low BP, preserved GFR
B. Overfill Theory (primary renal retention)
- Primary intrinsic renal Na⁺ retention occurs independently of oncotic pressure
- Mechanisms: ↓ GFR + interstitial inflammation + increased abundance/apical targeting of ENaC (epithelial sodium channels) in collecting tubules
- Filtered proteases (serine proteases) in tubular fluid proteolytically cleave ENaC, activating it → excess Na⁺ reabsorption
- Results in: ↑ plasma volume, hypertension, suppressed RAAS
- More common in inflammatory glomerulonephritides (membranous, FSGS, diabetic nephropathy)
In clinical practice, components of both mechanisms coexist, with the dominant mechanism varying by disease type and stage.
3. Hyperlipidaemia & Lipiduria
- ↓ Oncotic pressure → liver increases lipoprotein synthesis (VLDL, LDL)
- ↓ Lipoprotein lipase activity → impaired triglyceride clearance
- Lipiduria: oval fat bodies, fatty casts in urine
4. Hypercoagulable State
- Loss of anticoagulant proteins in urine: antithrombin III, protein C, protein S
- ↑ Hepatic synthesis of clotting factors (fibrinogen, factor V, VIII)
- ↑ Platelet aggregation
- → Risk of renal vein thrombosis, DVT, pulmonary embolism
5. Susceptibility to Infections
- Urinary loss of immunoglobulins (IgG) and complement factors (factor B, properdin)
- Impaired opsonisation → susceptibility to encapsulated organisms (e.g., Streptococcus pneumoniae)
Summary Flow
Glomerular injury (immune, toxic, genetic)
↓
Podocyte/slit diaphragm damage
↓
Massive proteinuria (>3.5 g/day)
↓
Hypoalbuminaemia
↓
↓ Plasma oncotic pressure
↓
┌────────────────┬────────────────┐
Underfill theory Overfill theory
↓ EABV Primary ENaC activation
↑ RAAS, SNS, ADH ↑ Na⁺ tubular reabsorption
Renal Na⁺/H₂O retention ↑ Plasma volume
└────────────────┴────────────────┘
↓
Oedema
+
Hyperlipidaemia, lipiduria, hypercoagulability, infections
Sources: Comprehensive Clinical Nephrology, 7th Ed. (Ch. 8); Brenner and Rector's The Kidney, 2-Vol Set
This is a shared conversation. Sign in to Orris to start your own chat.