I was in the ward, tell me gynec and obstetrics history taken in MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
I have sufficient content from the textbook. Now let me compile a comprehensive, well-structured answer for an MBBS student doing a ward posting in gynecology and obstetrics.
Gynecology & Obstetrics History Taking (MBBS Ward Guide)
Based on Berek & Novak's Gynecology, here is the complete structured history you take in a gynec/obs ward posting.
1. Patient Identification (Biodata)
- Name, Age, Address
- Marital status, Duration of marriage
- Occupation (patient and husband)
- Religion (relevant for certain practices)
- Date of admission
2. Chief Complaint (CC)
The patient's presenting symptom(s) in her own words, with duration. Allow her to talk freely before guiding.
Common gynec complaints: abnormal uterine bleeding, vaginal discharge, pelvic pain, lower abdominal mass, dysmenorrhea, infertility, urinary symptoms.
Common obstetric complaints: amenorrhea, vomiting, abdominal pain, bleeding in pregnancy, decreased fetal movements.
3. History of Present Illness (HPI)
Use the structured SOCRATES approach:
- Onset - When did it begin? Sudden or gradual?
- Character - Nature of complaint (e.g., colicky, dull, burning)
- Duration - How long has it been present?
- Severity - Mild, moderate, severe? Effect on daily activities?
- Radiation - Does pain go anywhere?
- Associated symptoms - Any related complaints?
- Aggravating/Relieving factors
- Timing - Constant or intermittent? Related to menstrual cycle?
Ask about the temporal relationship of symptoms to the total illness. Establish the date of first appearance.
4. Menstrual History (MH) - The Most Important Part of Gynec History
This is unique to gynecology and must always be thorough.
| Parameter | What to Ask |
|---|---|
| Age of menarche | At what age did periods start? |
| LMP (Last Menstrual Period) | Date of first day of last period |
| Cycle regularity | Regular or irregular? |
| Cycle length (interval) | How many days between periods? (Normal: 21-35 days) |
| Duration of flow | How many days does the period last? (Normal: 3-7 days) |
| Amount of flow | Light, moderate, heavy? Number of pads soaked per day? Clots? (Normal: <80 mL total) |
| Dysmenorrhea | Is there pain during periods? Primary or secondary? |
| Intermenstrual bleeding | Any bleeding between periods? |
| Postcoital bleeding | Bleeding after intercourse? |
| Premenstrual symptoms | Breast tenderness, bloating, mood changes? |
| Menopause (if relevant) | Age of menopause, any postmenopausal bleeding? |
Key terms to know:
- Menorrhagia: heavy regular periods
- Metrorrhagia: irregular bleeding between periods
- Menometrorrhagia: heavy and irregular
- Oligomenorrhea: periods >35 days apart
- Amenorrhea: no periods for >3 months (secondary) or never started (primary)
- Dysmenorrhea: painful periods
5. Obstetric History (OH)
This is recorded as G_P_A_L_ (Gravida, Para, Abortion, Living children).
| Term | Meaning |
|---|---|
| Gravida (G) | Total number of pregnancies including current |
| Para (P) | Deliveries after 28 weeks (viability), regardless of outcome |
| Abortion (A) | Pregnancy loss before 28 weeks (spontaneous or induced) |
| Living (L) | Number of currently living children |
For each past pregnancy, ask:
- Year of delivery
- Place of delivery (home/hospital)
- Duration of pregnancy (term/preterm/post-term)
- Mode of delivery (normal vaginal / LSCS / forceps / vacuum) - if LSCS, reason?
- Birth weight and sex of baby
- Any complications during pregnancy (hypertension, diabetes, antepartum hemorrhage)
- Any complications during/after delivery (PPH, retained placenta, eclampsia)
- Puerperium - any fever, breast problems, wound issues?
- Outcome of baby - alive and well, neonatal death, congenital anomaly?
If current pregnancy (Obstetric case):
- Date of LMP
- Expected Date of Delivery (EDD) - LMP + 9 months + 7 days (Naegele's rule)
- Gestational age in weeks
- Fetal movements - when first felt (quickening)? Frequency now?
- Antenatal visits done? Investigations done (blood group, Hb, ultrasound)?
- Any complications in this pregnancy?
6. Contraceptive History
- Type of contraceptive used (OCP, IUCD, condoms, sterilization, injectable)
- Duration of use
- Compliance and side effects
- Reason for stopping
7. Sexual History
Ask sensitively and with privacy:
- Age at first intercourse (coitarche)
- Number of partners
- Dyspareunia (pain during intercourse - superficial or deep?)
- Any history of STIs
8. Past Medical History (PMH)
- Any previous medical illnesses: hypertension, diabetes, thyroid disorder, epilepsy, TB, cardiac disease
- Previous surgeries (especially abdominal/pelvic): cesarean section, myomectomy, appendicectomy, D&C
- Previous hospitalizations
- Blood transfusions
9. Family History (FH)
Ask specifically for:
- Hypertension, diabetes (especially relevant in obstetrics)
- Twins (familial tendency)
- Breast cancer, ovarian cancer, cervical cancer, colorectal cancer
- Congenital anomalies or genetic diseases
- BRCA1/BRCA2 mutations (if relevant)
- Bleeding disorders
10. Personal and Social History
- Marital status and duration of marriage
- Consanguinity (cousin marriage - important for genetic conditions)
- Socioeconomic status
- Diet and nutrition (especially in pregnancy - iron, folic acid)
- Smoking, alcohol, substance use
- Occupation - exposure to toxins, radiation, stress
- Domestic violence screening (sensitively)
- Level of education
11. Drug and Allergy History
- Current medications including oral contraceptive pills, hormone therapy
- Over-the-counter and herbal medications
- Known drug allergies - drug name and type of reaction
12. Review of Systems (ROS)
Quickly screen other systems not already covered:
- Urinary symptoms: frequency, urgency, incontinence, dysuria (urogynecology)
- Bowel symptoms: constipation, dyschezia (pain on defecation - endometriosis)
- Respiratory/cardiovascular: relevant in obstetric patients with comorbidities
- Weight changes, fatigue, heat/cold intolerance (thyroid)
Quick Memory Aid for Gynaec History
"BC MOP SFPAD"
- Biodata
- Chief Complaint
- Menstrual History
- Obstetric History
- Past medical/surgical history
- Sexual and Contraceptive History
- Family History
- Personal/Social History
- Allergy and Drug History
- Drug Review of Systems
Special Notes for Ward Bedside Clerking
- Always begin by introducing yourself and ensuring privacy.
- The LMP is the single most important date in both gynec and obstetric history.
- In obstetrics, always confirm fetal movements and calculate gestational age yourself.
- Menstrual history must precede the physical exam - it guides what you look for.
- Record the obstetric history as G_P_A_L_ notation at the top of your write-up.
- Ask about domestic violence and sexual history privately, without the husband or family present.
- For a gynec patient, also ask about last Pap smear and any prior abnormal cervical results.
Source: Berek & Novak's Gynecology (based on clinical history-taking framework from Chapter 1: Initial Assessment and Communication)
Tell me history taking with examination and proper chronology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a complete, well-illustrated answer. Let me compile the full chronological guide.
Gynecology & Obstetrics: Complete History + Examination in Chronological Order
Sources: Berek & Novak's Gynecology; Textbook of Family Medicine 9e
PART A: HISTORY TAKING (Chronological Order)
Step 1 - Patient Introduction & Setting
Before starting:
- Introduce yourself by name and role
- Ensure privacy (close curtains, ask relatives to step out - especially for sexual/social history)
- Obtain verbal consent for history and examination
- Note: husband/partner should NOT be present for sensitive parts
Step 2 - Biodata
| Parameter | Details |
|---|---|
| Name, Age | |
| Address | |
| Marital status | Married / Unmarried / Widowed / Divorced |
| Duration of marriage | In years |
| Occupation | Patient + husband |
| Religion | (relevant for certain practices, consanguinity) |
| Date of admission |
Step 3 - Chief Complaint (CC)
Let the patient speak freely first. Record in her own words + duration.
Examples:
- "Bleeding per vaginum since 3 months"
- "No period since 4 months with nausea"
- "Lower abdominal pain for 2 weeks"
Textbook tip: "Allow the patient to talk about her chief symptom. Do not interrupt the patient's account, except for minor promptings such as 'When did it begin?' and 'How did it begin?'" - Berek & Novak's Gynecology
Step 4 - History of Present Illness (HPI)
Explore using the structured approach from Table 1-5 (Berek & Novak):
- Onset - Sudden or gradual? Date of first appearance?
- Duration - How long has it been going on?
- Character - Nature of the symptom
- Severity - Mild/moderate/severe? Effect on daily life?
- Aggravating and relieving factors
- Associated symptoms - Ask related complaints
- Temporal relationship - Is it related to menstrual cycle / pregnancy?
- Previous similar episodes
- Treatment taken so far - What was given? Did it help?
Also assess:
- Systemic symptoms: fever, weight loss, fatigue, anorexia (suggest malignancy or systemic illness)
- Psychological reaction: anxiety, depression, fear
Step 5 - MENSTRUAL HISTORY (MH) - Unique to Gynecology
This is the single most important part of a gynec history.
| Parameter | Question to Ask | Normal Range |
|---|---|---|
| Age of menarche | "How old were you when periods first started?" | 11-14 years |
| Regularity | "Are your periods regular?" | Regular |
| Cycle length (interval) | "How many days between first day of one period to first day of next?" | 21-35 days |
| Duration of flow | "How many days does your period last?" | 3-7 days |
| Amount of flow | "How many pads do you soak per day? Any clots?" | <80 mL total |
| LMP | "When was the first day of your last period?" | Must record |
| Dysmenorrhea | "Do you have pain during periods?" | None |
| Intermenstrual bleeding | "Any bleeding between periods?" | None |
| Postcoital bleeding | "Any bleeding after intercourse?" | None |
| PMS | "Any breast tenderness, bloating, mood changes before periods?" | |
| PALM | "Any history of fibroids, polyps, bleeding disorders?" | |
| If postmenopausal | Age of menopause, any bleeding since? | Menopause: ~51 years |
Key menstrual terms:
- Menorrhagia: Heavy regular periods (>80 mL or >7 days)
- Metrorrhagia: Irregular/intermenstrual bleeding
- Menometrorrhagia: Heavy AND irregular
- Oligomenorrhea: Cycles >35 days apart
- Amenorrhea: Primary (never menstruated by 16) / Secondary (absent >3 months)
- Dysmenorrhea: Painful periods - Primary (no pathology) / Secondary (endometriosis, fibroids)
- Polymenorrhea: Cycles <21 days
Step 6 - OBSTETRIC HISTORY (OH)
Recorded as: G_ P_ A_ L_
| Symbol | Meaning |
|---|---|
| G (Gravida) | Total pregnancies including current |
| P (Para) | Deliveries after 28 weeks gestation |
| A (Abortion) | Pregnancy loss before 28 weeks |
| L (Living) | Currently living children |
For EACH past pregnancy, ask in order:
- Year of delivery
- Where delivered (home/hospital)
- Gestational age (term / preterm / post-term)
- Mode of delivery: Normal vaginal / LSCS (if LSCS - what was the indication?) / Forceps / Vacuum
- Baby sex and birth weight
- Complications in pregnancy (APH, PIH, GDM)
- Complications in labor/delivery (prolonged labor, PPH, perineal tear)
- Puerperium (fever, wound infection, breast problems)
- Outcome of baby (healthy / stillbirth / neonatal death / congenital anomaly)
If current pregnancy (for an obstetric patient):
- LMP and EDD (Naegele's rule: LMP + 9 months + 7 days)
- Gestational age in completed weeks
- Quickening (first fetal movements felt) - multigravida ~18 weeks, primigravida ~20 weeks
- Current fetal movements - frequency, any reduction?
- Antenatal visits attended (ANC)
- Investigations done (Hb, blood group, VDRL, HIV, obstetric ultrasound)
- Any complications in this pregnancy
Step 7 - Contraceptive History
- Type used: OCP / IUCD / condom / injectable / sterilization / barrier
- Duration of use
- Compliance and side effects
- Reason for stopping
Step 8 - Sexual History
(Ask privately, non-judgmentally)
- Sexually active? Age at first intercourse?
- Number of partners
- Dyspareunia - pain during intercourse? Superficial (introital) or deep (pelvic)?
- Any history of STI (gonorrhea, chlamydia, herpes, HPV)
- Last Pap smear and result
Step 9 - Past Medical and Surgical History
- Hypertension, diabetes, thyroid disease, epilepsy, TB, cardiac disease, asthma
- Previous surgeries: cesarean section, myomectomy, appendicectomy, D&C, tubal ligation
- Previous hospitalizations
- Blood transfusions
Step 10 - Family History
- Hypertension, diabetes (especially important in obstetric patients)
- Multiple pregnancies (twins)
- Breast, ovarian, cervical, colorectal cancer
- BRCA1/BRCA2 carriers
- Congenital anomalies or genetic diseases
- Bleeding disorders
Step 11 - Personal and Social History
- Marital status and duration
- Consanguinity (cousin marriage - important for genetic disorders)
- Socioeconomic status
- Diet and nutrition (iron, folic acid in pregnancy)
- Smoking (pack-years), alcohol, recreational drugs
- Occupation - occupational hazards, radiation exposure
- Domestic violence (ask sensitively, alone)
Step 12 - Drug and Allergy History
- Current medications (OCP, HRT, iron, folic acid, antihypertensives)
- Herbal and over-the-counter medications
- Known drug allergies (drug name + reaction type)
Step 13 - Review of Systems (ROS)
Screen quickly:
- Urinary: frequency, urgency, leakage (urogynecology)
- Bowel: constipation, dyschezia (pain on defecation - endometriosis)
- General: weight loss, fatigue, heat/cold intolerance (thyroid)
- Breast: discharge, lump, pain
PART B: PHYSICAL EXAMINATION (Chronological Order)
Step 1 - General Physical Examination (GPE)
Before the patient undresses, observe and record:
| Parameter | What to Note |
|---|---|
| General appearance | Well/ill-looking, conscious, cooperative |
| Built and nutrition | Thin, average, obese; BMI |
| Pallor | Conjunctival pallor - grade mild/moderate/severe |
| Icterus | Scleral yellowing |
| Cyanosis | Peripheral/central |
| Clubbing | Grades 1-4 |
| Lymphadenopathy | Especially inguinal and supraclavicular nodes |
| Oedema | Pedal oedema (graded +1 to +4), especially in obstetric patients |
| Vital signs | Pulse, BP, RR, Temperature |
| Height, Weight, BMI | |
| Secondary sexual characters | Breast development, pubic hair, axillary hair (Tanner staging if needed) |
| Thyroid | Palpate for goiter |
Step 2 - Breast Examination
The gynecologist routinely examines the breasts.
Inspection (patient sitting, arms at side, then arms raised):
- Size and symmetry
- Skin changes: peau d'orange, erythema, dimpling, retraction
- Nipple changes: inversion, discharge, ulceration
Palpation (patient supine, arm raised behind head):
- All four quadrants + axillary tail + nipple-areola complex
- Any mass: site, size, shape, surface, consistency, tenderness, mobility, margin, skin fixity
- Axillary lymph nodes (anterior, posterior, central, apical groups)
- Supraclavicular nodes
Step 3 - Abdominal Examination
Position: Patient supine, bladder emptied (very important), knees slightly flexed, hands by sides.
Inspection
- Shape: flat, scaphoid, distended
- Symmetry
- Any visible mass or distention (gravid uterus? Ovarian cyst?)
- Umbilicus: central/displaced, inverted/everted
- Skin: linea nigra, striae gravidarum (pregnancy), striae albicans (old), surgical scars
- Movements: with respiration
Palpation
- Check for tenderness first (ask patient to point to painful area - examine that area last)
- All four quadrants systematically (clockwise from right upper quadrant)
- Liver edge (ask to breathe in/out)
- Spleen
- Uterus/pelvic mass: size (in weeks of gestation from pubic symphysis), surface, consistency, tenderness, mobility
- Rebound tenderness (peritoneal irritation)
- Free fluid/ascites: shifting dullness, fluid thrill
For Obstetric Patients - Uterine Size
| Gestational age | Level of fundus |
|---|---|
| 12 weeks | Just palpable above pubic symphysis |
| 16 weeks | Between symphysis and umbilicus |
| 20 weeks | At umbilicus |
| 24 weeks | 4 cm above umbilicus |
| 28 weeks | Halfway between umbilicus and xiphisternum |
| 32 weeks | 3/4 of distance to xiphisternum |
| 36 weeks | At xiphisternum |
| 40 weeks | Slightly below xiphisternum (due to lightening) |
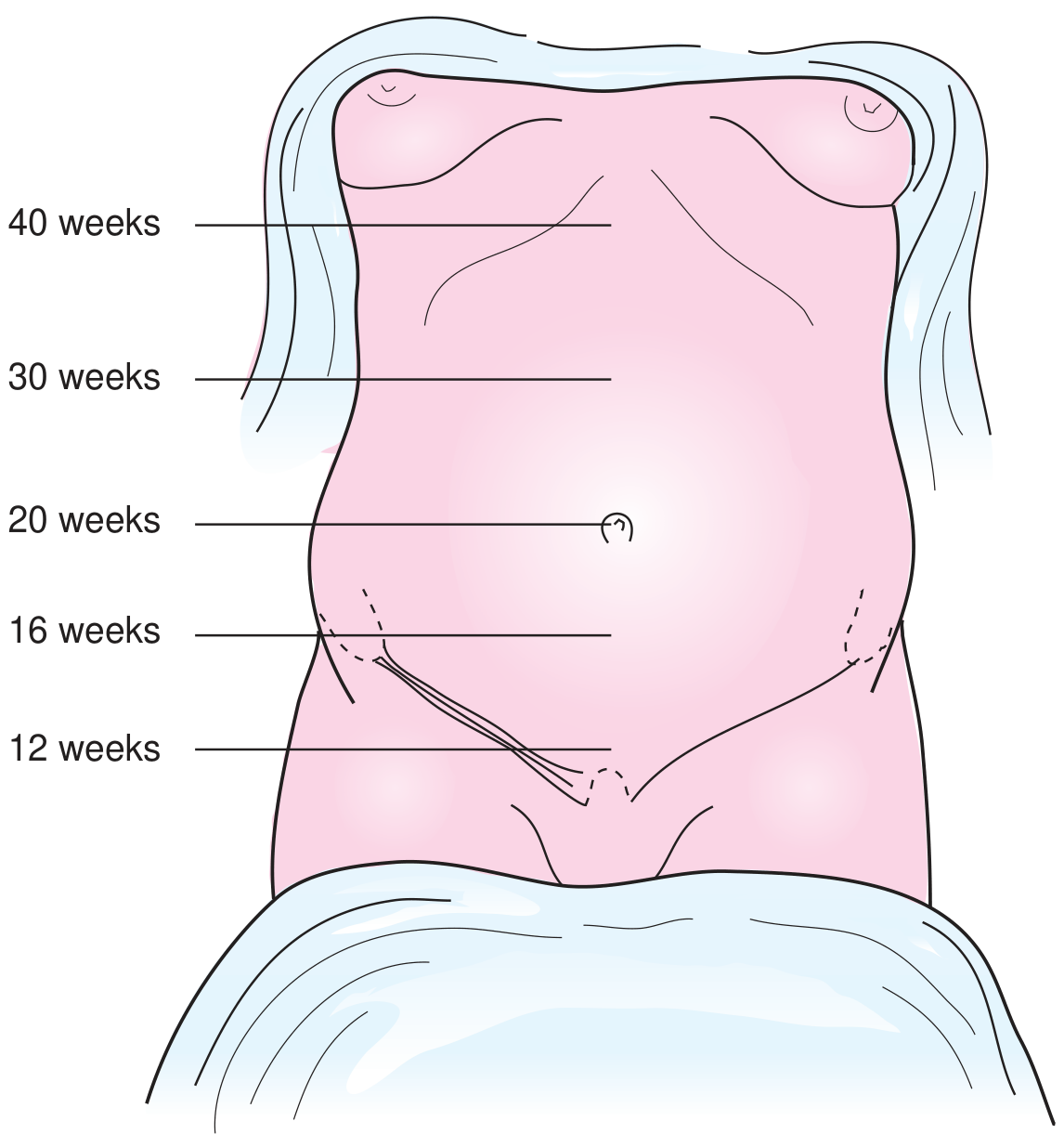
Fundal height measurement (after 20 weeks): Measure in cm from top of pubic symphysis to top of fundus. Centimeters = gestational weeks (±2 cm). Berek & Novak's Gynecology
For Obstetric Patients - Leopold's Maneuvers (from 30 weeks)
Performed with the patient supine after bladder is emptied.
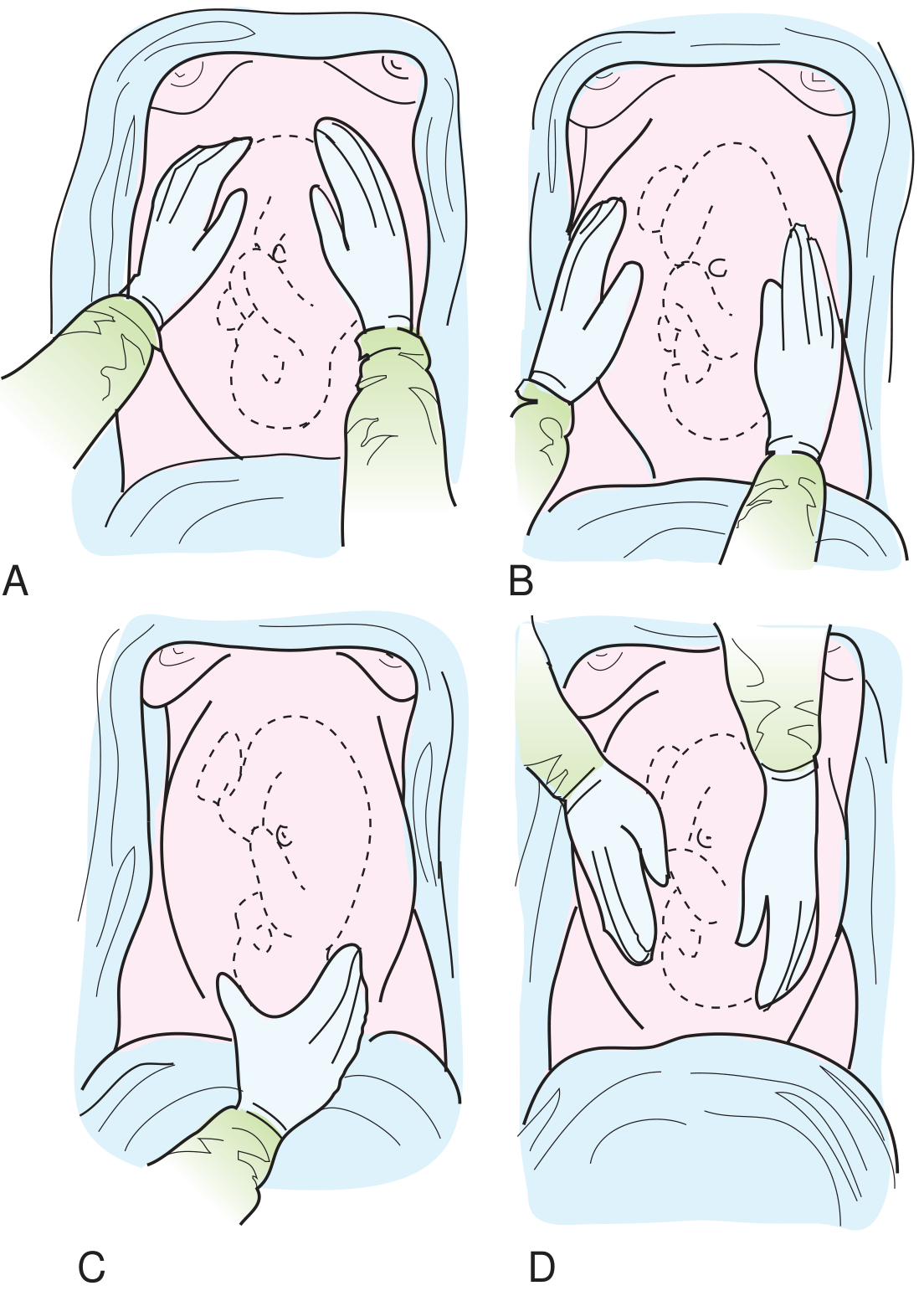
| Maneuver | Action | What you find |
|---|---|---|
| 1st Maneuver (Fundal grip) | Both hands cup the fundus | Identifies which fetal part is at the fundus (head = hard, round, ballotable; breech = soft, irregular) |
| 2nd Maneuver (Lateral/Umbilical grip) | Both hands slide down laterally | Identifies fetal back (firm, smooth, resistant) vs limbs (irregular, knobby) - determines lie and position |
| 3rd Maneuver (Pawlick's grip) | One hand grasps presenting part above symphysis | Identifies presenting part and degree of engagement (fixed = engaged, ballotable = not engaged) |
| 4th Maneuver (Pelvic grip) | Examiner faces patient's feet, fingers point toward pelvis | Determines degree of flexion/descent; palpates cephalic prominence |
Fetal heart auscultation: Using Pinard's stethoscope or Doppler (after 20 weeks). Normal FHR: 110-160 bpm. Best heard through fetal back.
Percussion
- Shifting dullness for ascites (ovarian cancer)
- Percuss uterine mass if gynec case
Auscultation
- Bowel sounds
- Fetal heart tones (obstetric)
Step 4 - Pelvic Examination
Prerequisites:
- Patient empties bladder
- Chaperone present (mandatory)
- Patient's consent obtained
- Good lighting
- Patient in dorsal lithotomy position
Before starting: Ask about previous difficult examinations, history of trauma, or abuse. Warn the patient before each step.
A. Inspection of External Genitalia
Inspect systematically (Berek & Novak, Table 1-6):
- Mons pubis, labia majora, labia minora, perineal body, anal region
- With labia separated:
- Labia minora
- Clitoris (size, any abnormality)
- Urethral orifice (any caruncle, discharge)
- Vaginal introitus/hymen
- Perineal body
- Anus
- Note: skin quality, pigmentation, erythema, lesions, excoriations, ecchymosis, swelling
- Ask patient to bear down: observe for cystocele (anterior bulge), rectocele (posterior bulge), uterine prolapse
- Check Bartholin's glands (posterior labia majora) - swelling, tenderness, cyst/abscess
- Check Skene's glands (paraurethral) - milk undersurface of urethra for discharge if indicated
B. Speculum Examination
Not done in prepubertal girls without anesthesia. Use smallest appropriate speculum.
Types of specula: Cusco's (most common), Sims' (for prolapse), Pederson's (narrow), Graves' (large), Huffman's (virginal)
Procedure:
- Warm the speculum
- Insert obliquely with downward pressure (not into urethra)
- Rotate and open blades under vision
Inspect:
- Vaginal walls: color, rugosity, discharge (amount, color, odor, consistency), lesions
- Cervix: size, shape (multiparous - transverse os; nulliparous - pinpoint), color, ectopy/erosion, polyps, ulcers, bleeding, abnormal discharge from os
- Collect Pap smear / HVS / endocervical swab if indicated
C. Bimanual Palpation
(Index and middle fingers of one hand in vagina; other hand on lower abdomen)
Step-by-step (Berek & Novak):
- Vagina: Note tenderness, masses, structural abnormality
- Cervix:
- Position (anterior/posterior)
- Consistency (firm/soft - Hegar's sign in pregnancy = soft isthmus)
- Surface irregularity
- Cervical motion tenderness (CMT): gentle movement of cervix - pain indicates pelvic inflammatory disease
- Uterus (coordinate both hands):
- Position: anteflexed / retroflexed / anteverted / retroverted
- Size: normal (pear-sized, 7-8 cm) or enlarged (in weeks)
- Shape: regular or irregular (fibroids)
- Consistency: firm/soft
- Tenderness
- Mobility
- Right adnexa (right lateral fornix + right iliac fossa):
- Normal tube is not palpable
- Normal ovary: ~4×2×3 cm, slightly tender, mobile
- Mass: size, consistency, tenderness, mobility, relationship to uterus
- Left adnexa: same technique on left side
- Posterior fornix / Pouch of Douglas (POD): any fullness, tenderness, nodularity (endometriosis)
D. Recto-vaginal Examination
- Index finger in vagina, middle finger in rectum
- Allows palpation higher in the pelvis beyond the POD
- Checks uterosacral ligaments (nodularity = endometriosis)
- Checks rectal mucosa
- Essential if retroversion of uterus is suspected
- In women with intact hymen: rectal-abdominal examination only
E. Rectal Examination
- Inspect perianal area: skin tags, fissures, fistula, hemorrhoids, pilonidal sinus
- Insert lubricated gloved finger
- Note anal sphincter tone
- Palpate rectal wall circumferentially
- In gynec: feel for cervix, posterior uterine wall, uterosacral ligaments
Step 5 - Vaginal (Per Vaginum) Examination in Labor (Obstetric)
Done only in obstetric patients in labor or for specific indications (PROM, cervical assessment).
Assess and record:
| Parameter | What to Note |
|---|---|
| Cervical dilatation | 0-10 cm (fully dilated = 10 cm) |
| Cervical effacement | % of cervical canal that has been taken up |
| Cervical consistency | Firm / soft / medium |
| Cervical position | Posterior / mid / anterior |
| Presenting part | Vertex (head) / Breech / Shoulder |
| Station | Level of presenting part relative to ischial spines (-3 to +3) |
| Membranes | Intact / ruptured |
| Denominator / position | Occiput anterior / posterior / transverse |
| Moulding | Overlap of fetal skull bones (0 to +++) |
Bishop Score (used to assess cervical readiness for labor induction):
- Dilatation + Effacement + Station + Consistency + Position
- Score ≥8 = favorable cervix
SUMMARY: Full Chronological Sequence for Ward
HISTORY
1. Biodata
2. Chief Complaint + Duration
3. History of Present Illness
4. Menstrual History (LMP, cycle, duration, flow, dysmenorrhea)
5. Obstetric History (G_P_A_L_ + each pregnancy details)
6. Contraceptive History
7. Sexual History
8. Past Medical + Surgical History
9. Family History
10. Personal + Social History
11. Drug + Allergy History
12. Review of Systems
EXAMINATION
1. General Physical Examination (GPE) + Vitals
2. Breast Examination
3. Abdominal Examination
- Inspection
- Palpation (± Leopold's maneuvers in obstetric cases)
- Fundal height measurement
- Fetal heart auscultation (obstetric)
- Percussion
- Auscultation
4. Pelvic Examination (lithotomy position)
A. External genitalia inspection
B. Speculum examination (vagina + cervix)
C. Bimanual palpation (vagina, cervix, uterus, adnexa)
D. Recto-vaginal examination
E. Rectal examination
5. Per Vaginum (PV) examination (if in labor - obstetric)
Pro tip for ward rounds: Always record your findings in SOAP format - Subjective (history), Objective (examination), Assessment (provisional diagnosis), Plan (investigations and management). Your attendings will be impressed.
Is cns etc system examination do in gynaecology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I have enough information. Now let me give a thorough, practical answer.
Do CNS and Other Systemic Examinations Apply in Gynecology/Obstetrics?
Yes - but with a very important rule: examine what is clinically relevant to the patient's condition. You do NOT routinely do a full neurological exam on every gynec patient. But for certain conditions, specific system exams become mandatory. Here is the complete breakdown:
The Golden Rule for MBBS Students
In Gynecology/Obstetrics, the examination is problem-directed. The systems you examine depend on the diagnosis you are suspecting.
There are two levels:
- Routine for every patient - GPE + breast + abdomen + pelvis (as covered before)
- Condition-specific - added systems based on the clinical situation
System-by-System Breakdown
1. CNS (Neurological) Examination
Routine gynecology case? - NO, not done.
Done when? - Specific obstetric emergencies where the brain is at risk.
| Clinical Situation | What CNS Examination to Do |
|---|---|
| Preeclampsia / Eclampsia | Deep tendon reflexes (DTR) - patellar (knee jerk), ankle clonus; visual disturbances (blurring, scotoma); headache assessment; GCS/conscious level |
| Eclampsia post-seizure | Full neurological exam - GCS, pupils, plantar reflex, cranial nerves |
| During Magnesium Sulfate therapy | Patellar reflex is the KEY monitoring sign - loss of patellar reflex = first sign of Mg toxicity; check before every dose |
| Headache in pregnancy | Full neurological exam + fundoscopy (to rule out raised ICP, cerebral venous sinus thrombosis) |
| Cerebral venous sinus thrombosis (CVST) | Full neuro exam; common in postpartum period |
| Hyperemesis gravidarum (severe) | Check for Wernicke's encephalopathy signs (confusion, ophthalmoplegia, ataxia) |
| Infertility / amenorrhea workup | Visual field testing (bitemporal hemianopia = pituitary tumor/prolactinoma pressing on optic chiasm) |
Most important CNS sign in obstetrics:
- Patellar reflex (knee jerk) - checked before EVERY dose of MgSO4 in eclampsia management
- Ankle clonus (>3 beats = pathological) - sign of CNS irritability in preeclampsia
- Papilledema on fundoscopy - raised ICP in severe preeclampsia
2. Cardiovascular System (CVS) Examination
Done routinely? - Yes, in all obstetric patients as part of booking visit and high-risk assessment. In gynecology, done when cardiorespiratory comorbidity is present.
| Clinical Situation | Why CVS Exam Matters |
|---|---|
| All antenatal patients (booking visit) | Baseline heart rate, BP, murmurs; undiagnosed RHD is common in Indian wards |
| Hypertension in pregnancy / Preeclampsia | BP measurement (both arms if aortic coarctation suspected), peripheral pulses, JVP |
| Cardiac disease in pregnancy | Full CVS exam - murmurs, added sounds, signs of heart failure (raised JVP, basal crepitations, pedal edema) |
| Anemia in gynec/obstetric patient | Tachycardia, flow murmurs, cardiomegaly |
| Pre-operative gynec assessment | Mandatory CVS exam before any surgery |
| Preeclampsia | JVP, signs of pulmonary edema |
What to examine:
- Pulse - rate, rhythm, volume, character
- Blood pressure - both arms if needed
- JVP
- Precordium - inspection, palpation (apex beat), percussion, auscultation (heart sounds, murmurs)
- Peripheral pulses
3. Respiratory System (RS) Examination
Done routinely? - In obstetric high-risk patients, yes. In routine gynecology, only if symptoms present.
| Clinical Situation | Why RS Exam Matters |
|---|---|
| Pulmonary edema in preeclampsia/eclampsia | Basal crepitations, reduced air entry |
| PPH (Postpartum hemorrhage) | Tachypnea, signs of shock, ARDS |
| Amniotic fluid embolism | Acute respiratory distress - RS exam critical |
| Pre-operative assessment | Chest auscultation mandatory |
| Pulmonary embolism (postpartum) | Tachypnea, pleural rub, reduced air entry |
| Cardiac disease in pregnancy | Pulmonary congestion - basal crepitations |
| COVID/respiratory illness in pregnancy | Full RS exam |
What to examine:
- Respiratory rate
- Chest expansion
- Tactile vocal fremitus
- Percussion note
- Auscultation - air entry, added sounds (crepitations, wheezes, pleural rub)
4. Thyroid Examination
Done routinely? - Yes, in gynecology especially for specific presentations.
| Clinical Situation | Why Thyroid Matters |
|---|---|
| Menstrual irregularity / Amenorrhea | Hypothyroidism causes oligomenorrhea/amenorrhea; hyperthyroidism causes irregular cycles |
| Infertility workup | Thyroid disorders are a major reversible cause |
| Weight changes + menstrual symptoms | Always examine thyroid |
| Galactorrhea | Hypothyroidism raises TRH → raises prolactin → galactorrhea |
| Hyperemesis gravidarum | Gestational transient thyrotoxicosis (hCG stimulates TSH receptor) |
| First antenatal booking visit | Screen clinically for thyroid disease |
What to examine:
- Inspection of neck (visible goiter?)
- Palpation - size, surface, consistency, bruit, mobility on swallowing
- Auscultation - thyroid bruit (hyperthyroidism)
- Signs of hypothyroidism: dry skin, hair loss, bradycardia, delayed ankle reflex, periorbital puffiness
- Signs of hyperthyroidism: tremor, warm moist skin, tachycardia, exophthalmos, lid lag
5. Musculoskeletal / Spine Examination
| Clinical Situation | Relevance |
|---|---|
| Assessment of pelvis (obstetrics) | Clinical pelvimetry - shape and adequacy of pelvis for vaginal delivery |
| Low back pain in pregnancy | Sacroiliac joint tenderness, lumbar lordosis |
| Symphysis pubis dysfunction | Tenderness over pubic symphysis |
| Spinal deformities | Kyphoscoliosis - affects lung function and anesthesia planning |
6. Eyes (Ophthalmic) Examination
| Clinical Situation | What to Check |
|---|---|
| Preeclampsia / Eclampsia | Fundoscopy - papilledema, retinal hemorrhages, retinal detachment (rare) |
| Prolactinoma / Pituitary tumor | Visual field defect - bitemporal hemianopia (sit opposite the patient and check fields by confrontation) |
| Diabetes in pregnancy | Diabetic retinopathy on fundoscopy |
| Jaundice in obstetric patient | Scleral icterus |
7. Skin and Mucous Membranes
Always examined as part of GPE:
| Sign | Condition |
|---|---|
| Pallor (conjunctiva, palm) | Anemia - very common in gynec/obs ward |
| Jaundice | Obstetric cholestasis, HELLP syndrome, acute fatty liver of pregnancy |
| Striae gravidarum | Normal pregnancy |
| Linea nigra | Pregnancy |
| Chloasma (melasma) | Pregnancy / OCP |
| Acanthosis nigricans | PCOS, insulin resistance |
| Hirsutism / virilization | PCOS, androgen-secreting tumor, CAH |
| Petechiae / purpura | DIC, thrombocytopenia (HELLP) |
| Edema | Preeclampsia, cardiac failure, hypoalbuminemia |
8. Lymph Nodes
| Site | When to Examine |
|---|---|
| Inguinal nodes | Vulvar pathology, vulvar cancer, STIs |
| Supraclavicular (Virchow's) | Ovarian cancer, cervical cancer metastasis |
| Axillary nodes | Part of breast examination |
| General lymphadenopathy | TB, lymphoma presenting with gynec symptoms |
Practical Summary Table
| System | Routine Gynec | Routine Obstetric | Condition-Specific |
|---|---|---|---|
| GPE + Vitals | ✅ Always | ✅ Always | |
| Breast | ✅ Always | ✅ Always | |
| Abdomen | ✅ Always | ✅ Always | |
| Pelvic exam | ✅ Always | ✅ (with caution) | |
| CVS | Only if symptoms/pre-op | ✅ At booking visit | Cardiac disease, preeclampsia, anemia |
| RS | Only if symptoms/pre-op | Only if symptoms | Pulmonary edema, PE, AFE |
| CNS | ❌ Not routine | ❌ Not routine | Eclampsia, Mg toxicity, CVST, prolactinoma |
| Thyroid | ✅ In menstrual/infertility cases | ✅ Booking visit screening | Thyroid disease, hyperemesis |
| Eyes | Only if symptoms | Only if symptoms | Preeclampsia fundoscopy, pituitary tumor visual fields |
| Musculoskeletal | ❌ Not routine | Pelvimetry when indicated | Backache, pelvic girdle pain |
| Lymph nodes | Inguinal (always), others if needed | Rarely | Vulvar/cervical malignancy |
How to Write It in Your Case Sheet
In a typical MBBS case write-up, after General Physical Examination, you write:
SYSTEMIC EXAMINATION
Cardiovascular System:
- Heart rate: 82/min, regular
- BP: 130/90 mmHg
- S1 S2 heard, no murmurs
Respiratory System:
- Respiratory rate: 18/min
- Air entry equal bilaterally, no added sounds
Per Abdomen: (detailed - as discussed)
Per Speculum / Per Vaginum: (detailed)
CNS: Conscious, oriented. No focal neurological deficit.
Deep tendon reflexes - normal bilaterally.
[Add: Patellar reflex present (if on MgSO4 - state this explicitly)]
Even if CNS is normal, always document it - especially in obstetric patients - because eclampsia can develop rapidly and your baseline documentation protects the patient and you.
Bottom Line
| Situation | CNS exam? | CVS? | RS? | Thyroid? |
|---|---|---|---|---|
| Routine gynec (AUB, discharge) | ❌ | Brief | Brief | ✅ if menstrual |
| Infertility | ❌ | Brief | Brief | ✅ Yes |
| Routine ANC | ❌ | ✅ Yes | Brief | ✅ Yes |
| Preeclampsia | ✅ Mandatory | ✅ Yes | ✅ Yes | - |
| Eclampsia / on MgSO4 | ✅ Mandatory | ✅ Yes | ✅ Yes | - |
| Pre-op gynec | ✅ Brief | ✅ Yes | ✅ Yes | - |
| Ovarian/cervical cancer | Brief | Brief | Brief | - |
The CNS exam in obstetrics is never skipped when there is hypertension, headache, visual symptoms, or the patient is on magnesium sulfate. That patellar reflex check before every MgSO4 dose is something your resident will test you on at the bedside.
Tell me all examination in detail with proper understanding with photos including cvs,rs, CNS etc in proper chronology to patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Here is the complete, detailed, chronological examination guide - exactly as you would do it standing next to a patient in the gynec/obs ward.
Complete Physical Examination - Gynecology & Obstetrics
Full Chronological Order with Understanding
Sources: Berek & Novak's Gynecology | Harrison's Principles of Internal Medicine 22e | Murray & Nadel's Respiratory Medicine | Goldman-Cecil Medicine | Textbook of Family Medicine 9e
The Universal Order: GPE → Hands → Pulse → BP → JVP → Eyes/Face → Neck → Breast → CVS → RS → Abdomen → CNS (when indicated) → Pelvic Examination
STEP 1 - PREPARATION (Before You Touch the Patient)
Before starting ANY examination:
- Wash hands / use sanitizer in front of the patient
- Introduce yourself - "I am [name], a medical student/intern"
- Take consent - "May I examine you?"
- Ensure privacy - close curtains/door
- Chaperone - always present for pelvic exam; ideally a female nurse
- Position the patient - supine initially, pillow under head, arms relaxed by side
- Adequate lighting - essential
- Ask patient to empty bladder before abdominal and pelvic exam
STEP 2 - GENERAL PHYSICAL EXAMINATION (GPE)
Patient is sitting or lying. You are standing to her right.
This is your first impression of the patient and gives you enormous clinical information before you even touch her.
A. General Appearance - Observe First
| What to See | What It Tells You |
|---|---|
| Conscious and oriented? | Mental status at a glance |
| Comfortable at rest or in distress? | Severity of illness |
| Appearance of age | Chronic illness if looks older than stated age |
| Built: thin / average / obese | Nutrition, PCOS (obese), malignancy (thin) |
| Skin color | Pallor, jaundice, cyanosis |
| Facial expression | Pain, anxiety, breathlessness |
| Posture | Guarding abdomen = peritonism |
B. Anthropometry
| Parameter | How to Measure | Clinical Relevance |
|---|---|---|
| Height | Stadiometer | BMI calculation |
| Weight | Weighing scale | BMI; weight gain in pregnancy |
| BMI | Weight(kg)/Height(m²) | Obesity → PCOS, GDM, preeclampsia |
C. Vital Signs
1. Pulse
Site: Radial artery (at wrist, lateral to flexor carpi radialis tendon)
Your fingers: Index + middle + ring finger pads on the vessel. Never use your thumb (has its own pulse).
| Parameter | Normal | Abnormal Meaning |
|---|---|---|
| Rate | 60-100/min (pregnancy: up to 100) | Tachycardia (anemia, hemorrhage, sepsis, PPH); Bradycardia |
| Rhythm | Regular | Irregular = arrhythmia |
| Volume | Normal | Low = shock/hemorrhage; High = hyperdynamic states |
| Character | Normal | Collapsing = aortic regurgitation; Plateau = aortic stenosis |
| Radio-radial delay | Simultaneous both sides | Delay = aortic arch pathology |
In obstetrics: Pulse >100 in a laboring patient should alert you to hemorrhage, sepsis, or severe anemia.
2. Blood Pressure
Equipment: Sphygmomanometer + stethoscope (bell on brachial artery)
Position: Patient seated or supine, arm at heart level, no tight clothing
How to take correctly:
- Palpate brachial artery (antecubital fossa, medial side)
- Apply cuff 2-3 cm above antecubital fossa - snugly
- Palpate radial pulse, inflate cuff until pulse disappears, then +30 mmHg
- Deflate slowly at 2 mmHg/second
- Korotkoff sounds: Phase I (first sound) = Systolic; Phase V (disappearance) = Diastolic
| Classification | Systolic | Diastolic |
|---|---|---|
| Normal | <120 | <80 |
| Hypertension in pregnancy | ≥140 | ≥90 |
| Severe hypertension | ≥160 | ≥110 |
Always take BP in both arms if you suspect aortic coarctation or if BP is high. Take it in the left lateral decubitus position in late pregnancy to avoid aortocaval compression.
3. Temperature
- Use digital thermometer (axillary or oral)
- Normal: 36.5°C - 37.5°C
- Fever: >38°C - think PID, chorioamnionitis, postpartum sepsis, UTI
- Record as: "Afebrile" or "Febrile (38.4°C)"
4. Respiratory Rate
- Count chest wall movements for a full minute (or 30 sec × 2) without telling the patient
- Normal: 12-20 breaths/min
- Tachypnea: >20 - pulmonary edema, sepsis, pulmonary embolism, anemia
- Record with the pulse (don't do it separately or patient will breathe abnormally)
D. Peripheral Signs (Hands to Head)
Work systematically from the extremities inward - this is the correct clinical method.
HANDS
| Sign | How to Elicit | Meaning |
|---|---|---|
| Pallor of palm creases | Open hand, look at creases | Anemia (very common in gynec ward) |
| Clubbing | Look at nail at side profile - loss of Lovibond angle | Chronic hypoxia, IBD, malignancy |
| Koilonychia | Spoon-shaped nails | Iron deficiency anemia |
| Leukonychia | White nails | Hypoalbuminemia |
| Tremor | Ask patient to hold hands out, fingers spread | Hyperthyroidism, anxiety |
| Warmth and moisture | Touch the palm | Hyperthyroidism (warm + moist) |
EYES - LOOK AT THESE CAREFULLY
| What to Look For | How | Meaning |
|---|---|---|
| Conjunctival pallor | Gently pull down lower eyelid - look at conjunctiva | Anemia - grade: mild/moderate/severe based on color depth |
| Scleral icterus | Look at sclera in good light | Jaundice - obstetric cholestasis, HELLP, acute fatty liver |
| Lid lag / Lid retraction | Ask patient to follow your finger downward | Hyperthyroidism |
| Exophthalmos | Look from side - does eye protrude beyond orbital rim? | Hyperthyroidism (Graves' disease) |
| Periorbital puffiness | Look at lower eyelids | Hypothyroidism, nephrotic syndrome, preeclampsia |
| Papilledema (use ophthalmoscope) | Direct ophthalmoscopy - look for blurred disc margin | Raised ICP - eclampsia, hypertensive emergency |
How to grade pallor: Pull down lower eyelid gently. Pale pink/white conjunctiva = pallor. Grade: Mild = pale but some color. Moderate = distinctly pale. Severe = white/almost no color.
FACE
| Sign | Meaning |
|---|---|
| Chloasma (butterfly pigmentation on cheeks) | Pregnancy, OCP use |
| Moon face | Cushing's syndrome |
| Acne + hirsutism | PCOS |
| Coarse features | Hypothyroidism |
| Malar flush | Mitral stenosis (cardiac disease in pregnancy) |
TONGUE AND MOUTH
| Sign | Meaning |
|---|---|
| Pale tongue | Anemia |
| Smooth tongue (glossitis) | Iron/B12 deficiency |
| Dry tongue | Dehydration |
| Central cyanosis (tongue blue) | Severe hypoxia |
NECK - THYROID
Inspection: Ask patient to swallow water. Watch the neck - a thyroid swelling moves up on swallowing (because it is attached to trachea). Lymph nodes visible?
Palpation: Stand behind the patient. Place both hands on either side of the trachea in the lower neck. Ask to swallow again. Feel:
- Size: which lobe enlarged?
- Surface: smooth (diffuse) or nodular?
- Consistency: soft / firm / hard
- Tenderness: thyroiditis
- Moves on swallowing? Tethering?
- Tracheal deviation?
- Cervical lymph nodes: pre/post-auricular, submandibular, anterior/posterior cervical chains, supraclavicular
Auscultation: Place bell of stethoscope over the thyroid. Listen for thyroid bruit (hyperthyroidism - increased blood flow).
Why thyroid matters in gynec/obs: Hypothyroidism causes menstrual irregularity, infertility, galactorrhea. Hyperthyroidism causes tachycardia, irregular cycles. Both must be excluded in infertility and AUB workup.
LYMPH NODES (General)
Examine these groups:
- Submandibular (under chin)
- Cervical - anterior and posterior chain
- Supraclavicular - Virchow's node (left side) = ovarian/cervical cancer metastasis
- Axillary - breast cancer
- Inguinal - vulvar cancer, STIs, lower limb infections
For each node: Size, Shape, Surface, Consistency, Tenderness, Mobility, Skin over it
EDEMA
Check for pedal edema: Press your thumb firmly for 5 seconds over the ankle (medial malleolus), dorsum of foot, and pretibial area. Release and see if a pit (depression) remains.
| Grade | Appearance |
|---|---|
| +1 | Barely perceptible, disappears quickly |
| +2 | Obvious pit, disappears in 10-15 seconds |
| +3 | Deep pit, disappears in 1-2 minutes |
| +4 | Very deep pit, persists >2 minutes; anasarca |
In obstetrics: Grade 1+ pedal edema is physiological in pregnancy (from 30 weeks). Facial edema + rapid weight gain + HTN = preeclampsia until proven otherwise.
STEP 3 - BREAST EXAMINATION
Position: Patient sitting initially, then supine.
Why in gynaecology? The gynecologist/obstetrician is often the primary physician for women and is responsible for breast cancer screening.
Inspection (Patient Sitting, Good Lighting)
Ask patient to:
- Arms by sides - baseline
- Arms raised above head - reveals skin dimpling, tethering
- Hands pressed on hips (pectoral contraction) - reveals subtle tethering
- Leaning forward - pendulous breasts: asymmetry, nipple position
Look for:
| Sign | Significance |
|---|---|
| Size and symmetry | Asymmetry may be normal or due to mass |
| Skin: peau d'orange | Lymphatic obstruction (breast cancer) |
| Skin: erythema | Inflammatory carcinoma, mastitis |
| Skin: dimpling/retraction | Tethering to underlying cancer |
| Nipple: retraction | Cancer, benign duct ectasia |
| Nipple: discharge | (Assess: color, blood-stained, unilateral) |
| Nipple: ulceration | Paget's disease of nipple |
| Veins: prominent | Dilated veins over large tumors |
| Scars | Previous surgery |
Palpation (Patient Supine, Arm Behind Head)
Use flat of the finger pads (not fingertips), in small circular movements.
Systematic approach - cover the entire breast:
- Divide into 4 quadrants + axillary tail (Tail of Spence)
- Or use clockwise concentric circles from nipple outward
- Include the nipple-areola complex last (gentle squeeze for discharge)
For any mass found, describe:
- Site (which quadrant, distance from nipple)
- Size (in cm)
- Shape (spherical / irregular)
- Surface (smooth / nodular)
- Consistency (soft / firm / hard / fluctuant)
- Tenderness
- Mobility (freely mobile / attached to skin / attached to muscle)
- Skin over it (normal / peau d'orange / dimpled)
- Margin (well-defined / ill-defined)
Axillary Lymph Node Examination
Support the patient's arm with your hand to relax the pectorals. Use your other hand to palpate:
- Anterior group (pectoral nodes) - under pectoralis major
- Posterior group (subscapular) - along posterior axillary fold
- Central group - central axilla
- Lateral group - medial to humerus
- Apical group - apex of axilla (feel with fingers pointing upward)
- Supraclavicular nodes - above clavicle, medial to sternocleidomastoid
STEP 4 - CARDIOVASCULAR SYSTEM (CVS) EXAMINATION
Position: Patient supine, head end at 45° for JVP. Lower to 0° (flat) for apex beat.
A. Inspection of the Precordium and Neck
| What to Look For | Meaning |
|---|---|
| Precordial bulge | Cardiomegaly in children; old pericardial effusion |
| Visible pulsations | Apex beat visible? RV heave (pulmonary hypertension) |
| Surgical scars | Previous cardiac surgery (e.g., valve replacement - RHD patient in pregnancy) |
| JVP (jugular venous pressure) | Elevation = raised right atrial pressure |
JVP Assessment (Harrison's Principles):
- Patient at 45° angle, head slightly turned left
- Look for internal jugular vein pulsation in the right side of neck (between the two heads of sternocleidomastoid)
- Measure height of venous column above the sternal angle in cm, then add 5 cm (sternal angle is 5 cm above right atrium)
- Normal JVP: ≤3 cm above sternal angle (i.e., ≤8 cm H₂O total)
- Raised JVP: cardiac failure, fluid overload, cardiac tamponade
- JVP vs carotid pulse: JVP is non-palpable, has 2 waves per beat, falls on inspiration, disappears with pressure on the root of the neck
B. Palpation of Precordium
| Step | What to Do | What It Means |
|---|---|---|
| Apex beat | Place right hand flat on precordium first (5 fingers) to locate it, then 2 fingers to characterize it | Normally in 5th intercostal space, midclavicular line. Displaced laterally = cardiomegaly (LV dilatation) |
| Heaves | Place heel of hand on lower left sternal edge | Right ventricular heave = pulmonary hypertension, RV enlargement |
| Thrills | Run fingers over all areas - feel for a vibration/buzz | Palpable murmur = significant valve lesion |
| Palpable P2 | Feel at pulmonary area (2nd ICS, left sternal border) | Pulmonary hypertension |
C. Percussion of the Heart
- Left cardiac border: percuss from axilla medially along each ICS (3rd, 4th, 5th) until dull
- Less commonly done; echocardiography has largely replaced this
- Still useful for bedside assessment of cardiomegaly
D. Auscultation - The Most Important Part
The 4 classic areas + Erb's point:
| Area | Location | Best For |
|---|---|---|
| Mitral area | 5th ICS, left midclavicular line (apex) | Mitral stenosis, MR, S3, S4 |
| Tricuspid area | 4th/5th ICS, left lower sternal border | Tricuspid valve, VSD |
| Pulmonary area | 2nd ICS, left sternal border | Pulmonary stenosis, loud P2 |
| Aortic area | 2nd ICS, right sternal border | Aortic stenosis, AR |
| Erb's point | 3rd ICS, left sternal border | Aortic regurgitation |
How to auscultate:
- Use diaphragm first (high-pitched sounds: S1, S2, systolic murmurs)
- Then bell (low-pitched sounds: S3, S4, mitral stenosis rumble)
- Auscultate each area: listen for S1, S2, added sounds, murmurs
Heart sounds:
| Sound | Timing | Meaning |
|---|---|---|
| S1 | Closure of Mitral + Tricuspid | "Lub" - start of systole |
| S2 | Closure of Aortic + Pulmonary | "Dub" - end of systole |
| S3 (gallop) | Early diastole (after S2) | LV failure, normal in pregnancy (<20 weeks) |
| S4 (gallop) | Late diastole (before S1) | Stiff ventricle, hypertension |
| Loud P2 | Accentuated pulmonic S2 | Pulmonary hypertension |
Murmurs - characterize by:
- Timing: systolic / diastolic / continuous
- Grade: I-VI (I = barely heard, VI = heard without stethoscope)
- Location: where loudest?
- Radiation: to axilla (MR), to carotids (AS), to back (PS)
- Character: harsh, blowing, rumbling
In Obstetrics: Pregnancy produces a physiological ejection systolic murmur (grade 1-2/6) due to increased cardiac output - this is normal. A diastolic murmur is always pathological. Any diastolic murmur in a pregnant woman = echocardiogram urgently.
E. Peripheral Vascular Examination
- All peripheral pulses: radial, brachial, femoral, popliteal, dorsalis pedis, posterior tibial
- Capillary refill time: Press nail bed for 5 seconds, release. Normal refill <2 seconds. >2 seconds = poor perfusion
- Ankle edema: already described above
STEP 5 - RESPIRATORY SYSTEM (RS) EXAMINATION
Position: Patient sitting upright (ideally), or as upright as possible.
Murray & Nadel's Respiratory Medicine: "Physical examination of the chest uses the four classic techniques of inspection, palpation, percussion, and auscultation."
A. Inspection
From the front and back. Clothing removed to waist with appropriate draping.
| What to Look | Normal | Abnormal |
|---|---|---|
| Shape of chest | Elliptical, slightly wider than deep | Barrel chest (COPD), pectus excavatum, kyphoscoliosis |
| Symmetry | Equal both sides | Asymmetry = volume loss (collapse, fibrosis), pleural effusion, pneumothorax |
| Respiratory rate | 12-20/min | Tachypnea >20 (pulmonary edema, PE); Bradypnea <12 |
| Breathing pattern | Regular, quiet | Accessory muscle use (intercostal recession, tracheal tug) = severe airway obstruction |
| Type of breathing | Abdominal-diaphragmatic | Paradoxical = diaphragm palsy |
| Scars | None | Thoracotomy, chest drain scars |
| Intercostal spaces | Symmetrical | Bulging = pleural effusion; Sucked in = lung collapse |
Also inspect for:
- Spine: kyphosis, scoliosis (affects lung function + anesthesia planning)
- Cyanosis: peripheral (blue fingers) vs central (blue tongue)
B. Palpation
Step 1: Tracheal position (do this first)
- Stand in front of patient
- Place index finger in suprasternal notch - feel which side the trachea is on
- Normal = central
- Deviated TOWARD lesion = lung collapse, fibrosis
- Deviated AWAY from lesion = massive pleural effusion, tension pneumothorax
Step 2: Chest expansion
- Place both hands symmetrically on the BACK of the chest (lower zones), thumbs meeting in the midline, fingers spread laterally
- Ask the patient to take a deep breath
- Watch your thumbs: they should move apart equally
- Normal: 5-7 cm expansion
- Reduced on one side: problem on that side
- Reduced bilaterally: COPD, fibrosis, pregnancy
Step 3: Tactile Vocal Fremitus (TVF)
- Place ulnar edge of hand (or palm) on chest wall
- Ask patient to say "99" or "one-two-three"
- Move hand systematically comparing sides
- Normal: moderate vibration felt symmetrically
- Increased TVF: consolidation (sound transmits better through solid lung)
- Decreased TVF: pleural effusion (fluid blocks transmission), pneumothorax, collapse
C. Percussion
Technique (Murray & Nadel):
- Place middle finger of left hand flat on chest wall (pleximeter) parallel to ribs
- Strike the middle phalanx of that finger with the tip of middle finger of right hand (plexor) in a quick wrist-flick motion
- Strike twice and listen carefully
- Move systematically: top to bottom, comparing left and right sides
Percussion notes:
| Note | Sound | Cause |
|---|---|---|
| Resonant | Hollow, medium pitch | Normal lung |
| Hyper-resonant | Drum-like, very hollow | Pneumothorax, emphysema |
| Dull | Thud-like, short | Consolidation (pneumonia), lobar collapse |
| Stony dull | Very dull, woody | Pleural effusion |
| Flat | No resonance | Solid tissue (muscle, liver) |
Percussion map of the chest:
- Front: 3 areas each side (clavicle, 2nd ICS, 4th ICS)
- Back: 5 areas each side (above spine of scapula, interscapular ×2, below scapular ×2)
- Axilla: compare both sides
Special percussion:
- Liver dullness: Percuss down from right side anteriorly - dullness starts at 5th ICS (liver upper border)
- Cardiac dullness: Left side anteriorly
- Stony dullness at base + absent TVF = pleural effusion (very important in preeclampsia and cardiac disease in pregnancy)
D. Auscultation
Technique: Press diaphragm firmly. Ask patient to breathe in and out through open mouth. Compare sides. Listen full inspiration + expiration at each spot.
Normal breath sounds:
| Sound | Location | Character |
|---|---|---|
| Vesicular | Over most of lung fields | Soft, low-pitched, inspiration longer than expiration |
| Bronchial | Over trachea / right upper lobe (near bronchi) | Loud, high-pitched, expiration = inspiration in length |
Abnormal breath sounds:
| Sound | Character | Cause |
|---|---|---|
| Crackles (crepitations) | Fine: late inspiratory, like rubbing hair near ear | Pulmonary edema (basal crackles), fibrosis |
| Coarse: early inspiratory/expiratory | Secretions, bronchiectasis | |
| Wheeze | Musical, expiratory | Bronchospasm (asthma, cardiac asthma in LVF) |
| Rhonchi | Low-pitched, snoring quality | Thick secretions in large airways |
| Pleural rub | Leathery, creaking | Pleuritis, pulmonary embolism |
| Bronchial breathing | Harsh, tubular over a peripheral area | Consolidation, collapse with patent bronchus |
Vocal resonance: Ask patient to say "99" while you auscultate - increased over consolidation (bronchophony), whispered "99" heard clearly over consolidation = whispering pectoriloquy (pathological).
What to specifically look for in gynaec/obs:
- Basal crepitations = pulmonary edema in preeclampsia or cardiac failure
- Absent breath sounds + stony dullness at base = pleural effusion
- Wheeze = asthma (common comorbidity) or cardiac asthma
STEP 6 - ABDOMINAL EXAMINATION
Position: Patient supine, bladder EMPTIED, knees slightly flexed (to relax abdominal muscles), arms by sides, pillow under head.
A. Inspection
Stand at the foot of the bed and look at the whole abdomen:
| What to Look For | Normal | Abnormal / Meaning |
|---|---|---|
| Shape | Flat/mildly rounded | Distended (ascites, large mass, pregnancy, intestinal obstruction); Scaphoid (wasting) |
| Symmetry | Symmetric | Asymmetric mass |
| Umbilicus | Central, inverted | Displaced (mass pushing); Everted (ascites, large mass, obesity) |
| Skin | Smooth | Linea nigra (pregnancy); Striae gravidarum (purple-pink = recent); Striae albicans (white = old); Caput medusae (portal HTN) |
| Scars | None | Midline (laparotomy); Pfannenstiel (LSCS, hysterectomy); RIF (appendix); Right subcostal (cholecystectomy) |
| Visible peristalsis | Not visible | Intestinal obstruction |
| Visible pulsation | Not visible | AAA (elderly/hypertensive) |
| Movement with breathing | Moves freely | Reduced movement = peritonism |
B. Palpation
Golden rule: Always ask "Are you having any pain anywhere?" and examine that area LAST.
Kneel or bend to the patient's level so your hand is flat. Start superficially before going deep.
Superficial Palpation
- All 9 regions systematically (or 4 quadrants)
- Light touch - feel for guarding, rigidity, superficial tenderness
- Watch the patient's face while palpating (they will wince if it hurts)
- Guarding = voluntary muscle contraction when you touch (patient knows it will hurt)
- Rigidity = involuntary board-like hardness (peritonism)
Deep Palpation
- Same 9 regions with deeper pressure
- Feel for organs and masses
Palpating the Liver:
- Start in the RIGHT ILIAC FOSSA, move upward toward the right subcostal margin
- Ask patient to breathe in and out - feel the liver edge come down on inspiration
- Normal liver: not palpable below the costal margin, or barely palpable
- If enlarged: describe in finger-breadths below costal margin, surface, consistency, tenderness
Palpating the Spleen:
- Start in the RIGHT ILIAC FOSSA, move diagonally toward LEFT hypochondrium
- Ask to breathe in - feel the splenic notch
- Cannot get above the spleen (vs kidney)
- Ballottement test for floating kidney
Palpating Pelvic/Uterine Mass:
- Start from the umbilicus and move toward the pubis
- Identify the upper border of the mass
- Measure in cm from pubic symphysis OR describe in relation to umbilicus
- Uterus 12 weeks = pubic symphysis level; 20 weeks = umbilicus; 36-40 weeks = xiphisternum
C. Percussion
- All 9 regions to map any dullness
- Shifting dullness for ascites: percuss from umbilicus laterally until dull. Keep finger there, ask patient to roll toward you. Dullness shifts to resonant = fluid has moved (positive shifting dullness = ascites)
- Fluid thrill: Place patient's or assistant's hand on midline. Flick one flank - feel thrill on other flank (large amounts of ascites)
- Percuss the uterine mass: dull
D. Auscultation (Before Deep Palpation Technically - Do It After Inspection in Practice)
- Listen for bowel sounds for at least 30 seconds
- Normal: gurgling sounds every 5-15 seconds
- Increased/tinkling = intestinal obstruction (early)
- Absent = paralytic ileus, peritonitis, post-operative
For Obstetric Patients - Fundal Height
Measurement after 20 weeks: Use a tape measure. From the upper edge of the pubic symphysis to the top of the uterine fundus in centimeters.
Rule: Fundal height in cm = gestational age in weeks (±2 cm)
If fundal height does NOT match dates, think:
- Larger than dates: Multiple pregnancy, polyhydramnios, LGA baby, fibroids, wrong dates
- Smaller than dates: FGR, oligohydramnios, wrong dates, fetal demise
For Obstetric Patients - Leopold's Maneuvers (from 28-30 weeks)
| Maneuver | Position | Action | You Determine |
|---|---|---|---|
| 1st (Fundal grip) | Face the patient's head. Both hands cup the fundus | Gently palpate what is in the fundus | What is at the fundus? - Head = hard, round, smooth, ballotable - Breech = soft, irregular, not ballotable |
| 2nd (Lateral/Umbilical grip) | Hands slide down both sides of uterus | One hand stabilizes, other palpates each side | Where is the fetal back? - Back = firm, smooth, resistant - Limbs = irregular, knobby, move away |
| 3rd (Pawlick's grip) | One hand grips above pubic symphysis | Gently grasp presenting part | What is the presenting part and is it engaged? - Mobile = not engaged - Fixed/cannot be moved = engaged |
| 4th (Pelvic grip) | Turn to face patient's feet. Both hands on lower uterus pointing downward | Fingers slide into pelvis | Degree of descent and flexion - Cephalic prominence on the same side as limbs = well flexed vertex - Prominent on same side as back = face/brow presentation |
Fetal Heart Auscultation:
- Use Pinard's stethoscope (place directly on abdomen, your ear against it) or Doppler probe
- FHR is best heard through the fetal back
- In LOA (left occiput anterior) = listen in the left lower quadrant
- In ROA = right lower quadrant
- Normal FHR: 110-160 beats/min
- Count for 1 full minute
- Bradycardia (<110) = fetal distress, cord compression
- Tachycardia (>160) = maternal fever, fetal anemia, early hypoxia
STEP 7 - CNS (NEUROLOGICAL) EXAMINATION
Done selectively - but when needed, done in this order.
When to do CNS exam in Gynec/Obs:
- Preeclampsia/Eclampsia
- On MgSO4 therapy (before every dose)
- Postpartum headache (rule out CVST)
- Prolactinoma/pituitary tumor (infertility workup)
- Any altered consciousness
A. Mental Status
Start by simply observing and speaking to the patient:
| Parameter | What to Assess |
|---|---|
| Consciousness | AVPU: Alert / Responds to Voice / Pain / Unresponsive |
| GCS | Eye (1-4) + Verbal (1-5) + Motor (1-6) = Total /15 |
| Orientation | Time, Place, Person ("What is today's date?" "Where are you?") |
| Behaviour | Agitated, restless, confused |
B. Cranial Nerve Screening (Relevant in Gynec/Obs)
You don't do all 12 cranial nerves routinely. Focus on:
| CN | Test | When Relevant |
|---|---|---|
| CN II (Optic) | Visual acuity (read newspaper), Visual fields by confrontation, Fundoscopy (papilledema) | Preeclampsia, pituitary tumor, headache |
| CN III, IV, VI (Eye movements) | "Follow my finger" - test all 6 directions | Wernicke's (hyperemesis), pituitary tumor, raised ICP |
| CN VII (Facial) | "Show me your teeth" / "Raise your eyebrows" | Rule out Bell's palsy (more common in pregnancy) |
Visual Field Testing by Confrontation (for pituitary tumor/prolactinoma):
- Sit directly facing the patient at arm's length
- Both cover one eye each (you cover your opposite eye)
- Bring a finger in from the periphery in all quadrants
- Pituitary tumor pressing on optic chiasm → Bitemporal hemianopia = loss of peripheral (temporal) vision in both eyes
C. Motor System
| Test | Method | Normal |
|---|---|---|
| Tone | Passively flex/extend limbs | Smooth, slight resistance |
| Power | Test 5 muscle groups each limb, grade 0-5 | Grade 5 (normal) all limbs |
| Coordination | Finger-nose test (point to your nose, then examiner's finger, alternating) | Smooth, accurate |
| Gait | Ask to walk normally | Steady, symmetrical |
Power grading:
- 5 = Normal power
- 4 = Movement against gravity + some resistance
- 3 = Movement against gravity only
- 2 = Movement with gravity eliminated
- 1 = Flicker of movement
- 0 = No movement
D. Sensory System (Brief Screen)
- Light touch: cotton wool on both sides simultaneously (compare)
- Pain: pin-prick (compare both sides)
- If asymmetry is found, map the level
E. Deep Tendon Reflexes - THE MOST IMPORTANT IN OBSTETRICS
This is the single most critical CNS exam in the obs ward.
| Reflex | Tendon Struck | Root | Patient Position |
|---|---|---|---|
| Biceps | Biceps tendon in antecubital fossa | C5, C6 | Arm semi-flexed, resting on examiner's arm |
| Triceps | Triceps tendon above olecranon | C7, C8 | Arm semi-flexed, hanging or supported |
| Supinator (Brachioradialis) | Distal radius, 5 cm above wrist | C5, C6 | Same as biceps |
| Knee (Patellar) | Patellar tendon below kneecap | L3, L4 | Knee flexed at 90° (legs hanging off bed OR knee supported on your arm) |
| Ankle (Achilles) | Achilles tendon at heel | S1, S2 | Foot slightly dorsiflexed, relaxed |
Grading of reflexes (0 to 4+):
| Grade | Meaning |
|---|---|
| 0 | Absent (even with reinforcement) |
| 1+ | Diminished |
| 2+ | Normal |
| 3+ | Exaggerated (brisk) |
| 4+ | Clonus (unsustained) |
Ankle Clonus Test (THE MOST IMPORTANT IN ECLAMPSIA):
- Hold the patient's foot
- Sharply and firmly dorsiflex the foot (push toes upward)
- Maintain the dorsiflexion
- Feel for rhythmic beats of the ankle
- Normal: 0-2 beats
- Pathological: 3 or more sustained beats = clonus = upper motor neuron lesion / CNS irritability
- In preeclampsia/eclampsia: clonus indicates severe CNS irritability, imminent seizure risk
THE RULE: Before every dose of MgSO4:
- Patellar reflex must be PRESENT (absence = MgSO4 toxicity → stop the infusion)
- Respiratory rate must be >16/min
- Urine output must be >25 mL/hour
F. Plantar Reflex (Babinski's Sign)
- Run a blunt key or orange stick along the outer border of the sole, from heel to little toe, then curving medially
- Normal (flexor): toes flex downward
- Abnormal (extensor/Babinski positive): big toe extends upward + other toes fan out
- Babinski positive = upper motor neuron lesion (stroke, severe metabolic encephalopathy, post-ictal state after eclampsia)
STEP 8 - PELVIC EXAMINATION
The patient must have emptied her bladder. Chaperone must be present.
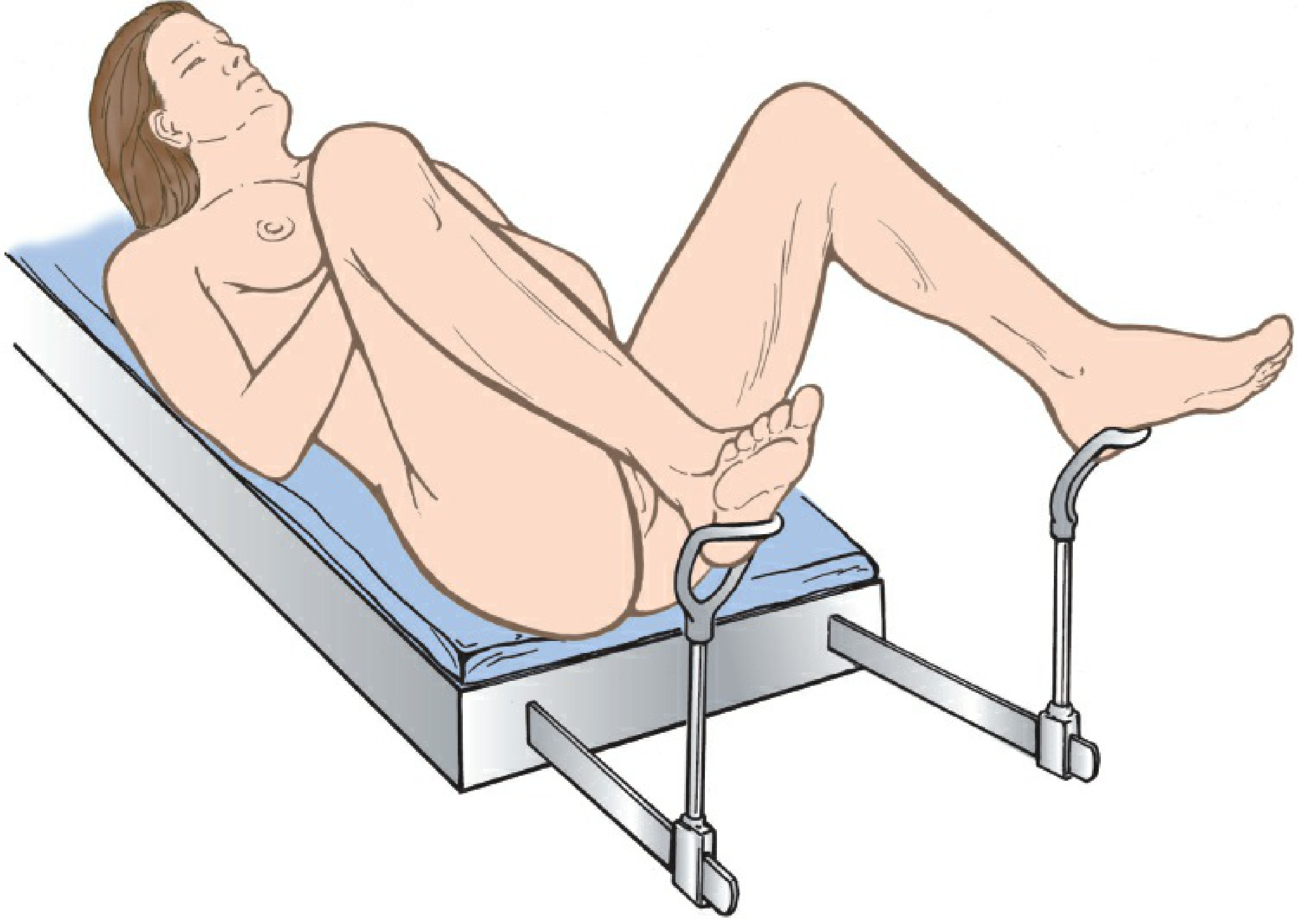
Position
Patient in dorsal lithotomy position:
- Lying on back
- Buttocks at the edge of the examination table
- Feet in stirrups, hips and knees flexed
- Good lighting directed at perineum
Before examining, tell the patient what you are going to do at each step.
A. External Genitalia - Inspection
Inspect systematically (Berek & Novak, Table 1-6):
- Mons pubis - distribution of pubic hair (sparse = hormonal; escutcheon pattern)
- Labia majora - swelling, ulcers, discoloration, varicosities (common in pregnancy)
- Labia minora - color, lesions, hypertrophy
- Clitoris - size (enlargement = virilization, androgen excess)
- Urethral orifice - urethral caruncle, discharge, prolapse
- Vaginal introitus - patency, hymen remnants, discharge
- Perineal body - scars (old tear / episiotomy), fistula
- Anus - hemorrhoids, fissure, skin tags, fistula, warts
Ask patient to bear down (Valsalva):
- Anterior vaginal wall bulge = Cystocele (bladder prolapse)
- Posterior wall bulge = Rectocele (rectum prolapse)
- Cervix/uterus descending = Uterine prolapse
Check Bartholin's gland: Feel between thumb (on labia majora) and index finger (in vaginal orifice) at the 5 o'clock and 7 o'clock positions. Swelling or tenderness = Bartholin's cyst or abscess.
B. Speculum Examination
Types of specula:
- Cusco's (bivalve) - most common, self-retaining
- Sims' - L-shaped, for prolapse examination
- Pederson's - narrow, for slender/adolescent patients
- Graves' - larger, for obese or parous women
Technique:
- Warm the speculum (warm water or speculum warmer - never lubricant before Pap smear)
- Insert at oblique angle into posterior introitus with downward pressure (away from urethra)
- Rotate to horizontal as you advance
- Open blades gently and identify the cervix
Inspect the Vagina (as you insert and withdraw):
- Color (pink = normal; blue = Chadwick's sign of pregnancy; pale = atrophy)
- Rugosity (present in reproductive age; absent postmenopause)
- Discharge: describe amount, color, consistency, odor, lesions
Inspect the Cervix:
| Feature | Normal | Abnormal |
|---|---|---|
| Os | Nulliparous = pinpoint; Multiparous = transverse slit | Dilated os (incompetent cervix, labor) |
| Color | Pink | Blue (Chadwick's sign, pregnancy); Red (cervicitis) |
| Ectopy/Ectropion | Fine red area around os | Present in OCP users, pregnant women, adolescents |
| Surface | Smooth | Polyps, ulcers, warty lesions, contact bleeding |
| Discharge from os | Mucoid/clear | Purulent (cervicitis, PID); Blood-stained (cancer) |
Take cervical samples if indicated:
- Pap smear: Use Ayre's spatula + endocervical brush
- High vaginal swab (HVS): from posterior fornix
- Endocervical swab: for chlamydia, gonorrhea
C. Bimanual Palpation
Technique: Index + middle fingers of dominant hand inserted into vagina. Other hand on lower abdomen, pressing down toward the vaginal fingers.
1. Vagina
- Feel along the vaginal walls - any tenderness, masses, nodules
- Check the fornices (anterior, posterior, lateral)
2. Cervix (vaginal fingers only)
- Position: anterior (normal) / posterior (retroflexed uterus)
- Consistency: firm (normal) / soft (Hegar's sign of early pregnancy - soft isthmus)
- Os: closed / open
- Cervical Motion Tenderness (CMT): Gently move cervix side to side - sharp pain = cervical excitation = PID, ectopic pregnancy (the "chandelier sign" - patient jumps up)
3. Uterus (bimanual - COORDINATE BOTH HANDS)
- Position: anteverted/anteflexed (normal) or retroverted/retroflexed
- Size: normal (7-8 cm, pear-shaped) / enlarged (in weeks equivalent)
- Shape: regular (normal) / irregular (fibroids - lobulated masses distorting shape)
- Consistency: firm (normal) / soft (pregnancy) / hard (calcified fibroid)
- Mobility: freely mobile (normal) / fixed (adhesions, endometriosis, malignancy)
- Tenderness: none (normal) / tender (PID, endometritis)
4. Adnexa (lateral fornix + lower abdominal hand on each iliac fossa)
- Normal tube: NOT palpable
- Normal ovary: 4×2×3 cm, slightly tender, mobile (sometimes palpable)
- Any adnexal mass: size, consistency, tenderness, mobility, relation to uterus
- Fullness in Pouch of Douglas (posterior fornix): fluid (ruptured ectopic, pelvic abscess), nodularity (endometriosis)
D. Recto-vaginal Examination
- Index finger in vagina, middle finger in rectum
- Allows examination higher in the pelvis
- Check uterosacral ligaments for nodularity (endometriosis)
- Check rectal mucosa (normal = smooth)
- Essential for staging of cervical cancer and endometriosis
E. Per Vaginum (PV) in Labor
Only when indicated. Done with sterile gloves.
| What to Assess | Details |
|---|---|
| Cervical dilatation | 0 (closed) → 10 cm (fully dilated) |
| Cervical effacement | 0% (no effacement) → 100% (fully effaced) |
| Cervical consistency | Firm / soft / medium |
| Cervical position | Posterior / mid / anterior |
| Presenting part | Vertex (head) / breech / shoulder |
| Station | -3 (above ischial spines) to +3 (at introitus), 0 = at ischial spines |
| Membrane status | Intact / ruptured (note liquor color - clear/meconium-stained) |
| Moulding | 0 = no moulding; + = bones touching; ++ = overlapping but reducible; +++ = fixed overlap |
COMPLETE EXAMINATION ORDER - QUICK REFERENCE CARD
STAND AT THE RIGHT SIDE OF THE PATIENT
1. PREPARATION
- Wash hands, consent, privacy, chaperone, empty bladder
2. GENERAL APPEARANCE
- Conscious? Distressed? Built? Pallor?
3. VITAL SIGNS
- Pulse → BP → Temp → RR → SpO2
4. PERIPHERAL EXAM (Hands → Head)
- Hands: pallor, clubbing, koilonychia, tremor
- Eyes: conjunctival pallor, icterus, exophthalmos, lid lag
- Face: chloasma, acne, coarse features
- Tongue: pallor, glossitis, cyanosis
- Neck: thyroid, lymph nodes, JVP
- Ankles: pitting edema
5. BREAST EXAM
- Inspection (sitting) → Palpation (supine) → Axillary nodes
6. CVS EXAM
- Inspect precordium + JVP
- Palpate: apex beat, heaves, thrills
- Percuss: cardiac borders
- Auscultate: 5 areas with diaphragm + bell
7. RS EXAM
- Inspect: shape, symmetry, RR, breathing pattern
- Palpate: trachea, expansion, TVF
- Percuss: all zones front + back (compare both sides)
- Auscultate: breath sounds, added sounds, vocal resonance
8. ABDOMINAL EXAM
- Inspect: shape, scars, umbilicus, skin signs
- Palpate: superficial → deep → liver → spleen → uterus/mass
- Fundal height (obstetric)
- Leopold's maneuvers (obstetric, >28 weeks)
- Percuss: dullness, shifting dullness
- Auscultate: bowel sounds, FHR (obstetric)
9. CNS EXAM (when indicated)
- Mental status + GCS
- Cranial nerves (II, III-VI, VII)
- Power + tone
- Deep tendon reflexes (especially patellar + ankle)
- Ankle clonus (ESSENTIAL in preeclampsia/MgSO4 monitoring)
- Plantar reflex (Babinski)
10. PELVIC EXAM (lithotomy position, chaperone present)
- External genitalia inspection + Valsalva
- Speculum: vagina + cervix (Pap smear if indicated)
- Bimanual: cervix + uterus + adnexa + POD
- Recto-vaginal (if indicated)
- PV in labor (if indicated)
11. COMPLETE
- Help patient dress
- Wash hands
- Thank and explain findings
"The goal of a complete examination is not to check every box - it is to understand the patient as a whole person, and to let the clinical findings guide you to a diagnosis." - Berek & Novak's Gynecology
Metabolic syndrome in medicine final year MBBS in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive content from Harrison's 22e (2025) and Basic Medical Biochemistry. I have everything needed to write a thorough, exam-quality answer for final year MBBS. Let me compile it.
Metabolic Syndrome - Final Year MBBS
Primary Source: Harrison's Principles of Internal Medicine 22e (2025), Chapter 420 - Robert H. Eckel; Basic Medical Biochemistry 6e
1. DEFINITION
The metabolic syndrome (also called Syndrome X or Insulin Resistance Syndrome) is a constellation of interrelated metabolic abnormalities that collectively confer increased risk of:
- Cardiovascular disease (CVD)
- Type 2 Diabetes Mellitus
The major features are: central obesity + hypertriglyceridemia + low HDL + hyperglycemia + hypertension - all driven by the central defect of insulin resistance.
"The metabolic syndrome consists of a constellation of metabolic abnormalities that confer increased risk of cardiovascular disease and diabetes mellitus." - Harrison's 22e (2025)
2. HISTORICAL EVOLUTION
| Year | Organization | Contribution |
|---|---|---|
| 1988 | Reaven | First described as "Syndrome X" - insulin resistance + dyslipidemia + HTN (but WITHOUT obesity) |
| 1998 | WHO | First formal definition - included microalbuminuria |
| 2001 | NCEP ATP III | Clinical criteria widely adopted (most used in practice) |
| 2005 | IDF | Emphasized waist circumference as the mandatory central criterion with ethnic-specific cutoffs |
| 2009 | Joint Statement (IDF + AHA + WHO + etc.) | Harmonized criteria - eliminated mandatory central obesity; requires any 3 of 5 |
3. DIAGNOSTIC CRITERIA
NCEP ATP III Criteria (Most Commonly Used in Clinical Practice)
Diagnosis requires: ANY 3 of the following 5 criteria (Harrison's 22e, Table 420-1):
| Criterion | Threshold |
|---|---|
| 1. Abdominal obesity (waist circumference) | Men: >102 cm (>40 inches) / Women: >88 cm (>35 inches) |
| 2. Hypertriglyceridemia | Fasting TG ≥150 mg/dL OR on specific medication |
| 3. Low HDL cholesterol | Men: <40 mg/dL / Women: <50 mg/dL OR on specific medication |
| 4. Hypertension | BP ≥130/85 mmHg OR on antihypertensive medication |
| 5. Hyperglycemia | Fasting plasma glucose ≥100 mg/dL OR on antidiabetic medication OR previously diagnosed T2DM |
IDF Criteria (2005) - Used in South Asian/Asian Populations
Central obesity is MANDATORY + any 2 of the remaining 4:
| Population | Waist Circumference Cutoff (Men/Women) |
|---|---|
| Europids, Middle East, African | ≥94 cm / ≥80 cm |
| South Asians, Chinese, South/Central Americans | ≥90 cm / ≥80 cm |
| Japanese | ≥85 cm / ≥90 cm |
For Indian patients (most important for your exam): Use IDF criteria. Waist ≥90 cm in men, ≥80 cm in women + any 2 of the other 4 criteria.
4. EPIDEMIOLOGY
- Prevalence in US adults: ~33-35% (NHANES data)
- Increases dramatically with age - affects nearly 50% of Americans >60 years
- Prevalence is 12-30% in obese/overweight children
- South Asians (Indians) have higher prevalence at lower BMI due to greater visceral fat deposition at any given waist circumference
- Rising globally with industrialization and sedentary lifestyles
- Women >60 years are more often affected than men of same age
5. ETIOLOGY / RISK FACTORS
A. Overweight/Obesity
- Central/visceral adiposity is the key driver
- Even normal-weight individuals can have metabolic syndrome if they have increased visceral fat (common in Indians, Southeast Asians)
B. Sedentary Lifestyle (Harrison's 22e)
- Physical inactivity reduces cardiorespiratory fitness → increases adipose tissue, raises TG, lowers HDL, raises BP and glucose
- Watching TV/screens >4 hours/day → 2-fold increased risk of metabolic syndrome
C. Aging
- Prevalence approaches 50% in adults >60 years
D. Genetic Factors
- Heritability of each metabolic trait exceeds 50%
- Multiple genes involved (no single gene) - body weight, insulin resistance, lipid metabolism
E. Gut Microbiome
- Increased Firmicutes/Bacteroidetes ratio associated with metabolic syndrome
- Bile acid metabolism and gut-derived inflammatory signals contribute
F. Other Conditions Associated
- Polycystic ovarian syndrome (PCOS)
- Non-alcoholic fatty liver disease (NAFLD/MASLD)
- Lipodystrophy
- Chronic kidney disease
- Hypothyroidism
- Obstructive sleep apnea
- Certain drugs: antipsychotics (clozapine, olanzapine), corticosteroids, antiretrovirals
6. PATHOPHYSIOLOGY
This is the most important section for final year - understand the mechanism thoroughly.
Central Defect: INSULIN RESISTANCE
Excess visceral adipose tissue
↓
↑ Free Fatty Acids (FFA) released into portal circulation
↓
Reach liver → ↑ VLDL synthesis → Hypertriglyceridemia
→ ↑ apoB, ↑ Small Dense LDL (atherogenic)
↓
Muscle: Fat oxidation predominates → Reduced glucose uptake → Insulin resistance
↓
Pancreatic β-cells: Compensatory ↑ insulin secretion → eventually β-cell failure → T2DM
A. Adipose Tissue Dysfunction (Harrison's 22e)
- Visceral fat releases FFA directly into the portal vein → liver receives high FFA load
- Large adipocytes in obesity have excess substrate → enhanced basal lipolysis even without hormonal activation
- Decreased perilipins (adipocyte phosphoproteins that normally protect stored TG) → enhanced unregulated lipolysis
- Adipose tissue becomes infiltrated with macrophages → chronic low-grade inflammation → cytokines (TNF-α, IL-6) worsen insulin resistance
B. Dyslipidemia Mechanism (Harrison's 22e)
- Step 1: Insulin resistance → impaired suppression of hepatic VLDL production
- Step 2: Excess FFA from visceral fat → ↑ apo B-containing VLDL production → Hypertriglyceridemia
- Step 3: Elevated apoC-III on VLDLs → inhibits lipoprotein lipase → impairs VLDL clearance → worsens hypertriglyceridemia
- Step 4: Elevated TG + CETP (cholesteryl ester transfer protein) → exchanges TG for cholesterol in HDL → makes HDL small, dense, protein-rich → rapidly cleared from circulation → Low HDL
- Step 5: With TG >2.0 mM (180 mg/dL) → Small Dense LDL predominates → more atherogenic (penetrate endothelium more easily, more oxidizable)
C. Glucose Intolerance Mechanism (Harrison's 22e)
- Defects in insulin action → impaired suppression of hepatic glucose production
- Reduced glucose uptake in muscle and adipose tissue
- Compensatory ↑ insulin secretion maintains euglycemia initially
- Eventually β-cell secretory capacity fails → IFG → IGT → T2DM
- High FFA levels in β-cells interfere with NADPH generation → impair insulin secretion (Basic Medical Biochemistry 6e)
D. Hypertension Mechanism
- Insulin resistance → ↑ Na⁺ retention by kidney (insulin normally promotes natriuresis)
- Sympathetic nervous system activation (FFA, leptin)
- ↑ Angiotensinogen from adipose tissue → ↑ Angiotensin II → vasoconstriction + Na⁺ retention
- Endothelial dysfunction → reduced NO → impaired vasodilation
E. Pro-inflammatory and Pro-thrombotic State
- ↑ CRP (C-reactive protein) - a marker of systemic inflammation
- ↑ IL-6, TNF-α from visceral adipocytes
- ↑ Fibrinogen, PAI-1 (plasminogen activator inhibitor-1) → impaired fibrinolysis → thrombotic tendency
- ↑ Uric acid (insulin resistance → impaired uric acid clearance)
F. Adipokines (Hormones from Fat)
| Adipokine | Change in MetS | Effect |
|---|---|---|
| Leptin | ↑ (but leptin resistance) | Normally suppresses appetite; resistance → hyperphagia |
| Adiponectin | ↓ (key finding) | Normally increases insulin sensitivity, anti-inflammatory; low adiponectin = worse IR |
| TNF-α | ↑ | Impairs insulin signaling (inhibits IRS-1) |
| IL-6 | ↑ | Induces CRP production, promotes insulin resistance |
| Resistin | ↑ | Promotes insulin resistance |
7. CLINICAL FEATURES
Metabolic syndrome is largely asymptomatic - it is detected on screening. However clinical features include:
History
- Overweight/obese, especially central obesity
- Family history of T2DM, CVD, hypertension
- Sedentary lifestyle, high-calorie diet
- In women: PCOS (menstrual irregularity, hirsutism, acne)
- Symptoms of associated conditions: snoring/sleep apnea, fatty liver (fatigue, right upper quadrant discomfort)
Physical Examination
| Finding | Significance |
|---|---|
| Central obesity | Increased waist circumference - measure at midpoint between lower rib and iliac crest |
| Elevated BP | ≥130/85 mmHg |
| Acanthosis nigricans | Velvety, dark hyperpigmentation at nape of neck, axillae, groins - marker of insulin resistance |
| Skin tags (acrochordons) | Associated with insulin resistance and obesity |
| Xanthelasma / xanthomas | Lipid deposits (eyelids = xanthelasma; tendons = xanthoma) |
| Hepatomegaly | NAFLD/MASLD |
| Hirsutism / acne | In women - PCOS (common association) |
| Fundoscopy | Hypertensive retinopathy, diabetic retinopathy (if progressed to T2DM) |
8. INVESTIGATIONS
Routine Screening (ATP III)
| Test | What to Look For | Threshold |
|---|---|---|
| Waist circumference | Central obesity | >102/88 cm (NCEP); >90/80 cm (IDF South Asian) |
| Fasting blood glucose (FBG) | Hyperglycemia | ≥100 mg/dL |
| Fasting lipid profile | TG, HDL, LDL | TG ≥150; HDL <40/<50 |
| Blood pressure | Hypertension | ≥130/85 mmHg |
| BMI | Obesity classification | Overweight ≥23 (Asian), ≥25 (Western) |
Additional Investigations
| Test | Purpose |
|---|---|
| HbA1c | Better glycemic assessment; ≥6.5% = diabetes; 5.7-6.4% = prediabetes |
| OGTT (75g oral glucose) | Detects IGT (2-hour glucose 140-199 mg/dL) - more sensitive than FBG alone |
| Fasting insulin + HOMA-IR | Quantifies insulin resistance. HOMA-IR = (fasting insulin × fasting glucose)/405; >2.5 = IR |
| Serum uric acid | Often elevated; marker of IR and cardiovascular risk |
| LFT + Liver ultrasound | Screen for NAFLD/MASLD |
| Urine microalbumin:creatinine ratio | Renal involvement; early nephropathy |
| ECG | Baseline cardiac assessment |
| hsCRP | Systemic inflammation marker |
| TSH | Exclude hypothyroidism (worsens dyslipidemia) |
| Serum testosterone / LH:FSH (women) | If PCOS suspected |
9. ASSOCIATED CONDITIONS AND COMPLICATIONS
| System | Complication |
|---|---|
| Cardiovascular | Coronary artery disease, stroke, heart failure - 2-3x increased CVD risk |
| Endocrine | Type 2 diabetes mellitus (5x increased risk), prediabetes |
| Liver | NAFLD → NASH → cirrhosis → hepatocellular carcinoma |
| Kidney | Chronic kidney disease, diabetic nephropathy |
| CNS | Cognitive decline, increased dementia risk |
| Malignancy | ↑ risk of colorectal cancer, breast cancer, endometrial cancer |
| Reproductive | PCOS, erectile dysfunction, male hypogonadism |
| Sleep | Obstructive sleep apnea (bidirectional relationship) |
| Skin | Acanthosis nigricans, skin tags |
10. TREATMENT (Harrison's 22e, Chapter 420)
Step 1 - Lifestyle Modification (CORNERSTONE OF TREATMENT)
Weight loss is the single most important intervention:
- Even 5-10% weight loss significantly improves all components
- Target: 0.5-1 kg per week
Diet
- Caloric restriction: 500-1000 kcal/day deficit
- Mediterranean diet or DASH diet - preferred
- Reduce: saturated fats, trans fats, refined carbohydrates, simple sugars (↑ VLDL production)
- Increase: fiber, whole grains, vegetables, monounsaturated fats (olive oil)
- Restrict alcohol: alcohol dramatically raises TG
- For hypertriglyceridemia: restrict dietary fat to ≤15% of calories
Physical Activity
- ≥150 min/week of moderate-intensity aerobic exercise (brisk walking, swimming, cycling)
- Aerobic exercise improves insulin sensitivity, reduces TG, raises HDL, lowers BP
- Even reducing sedentary time (screen time) has measurable benefit
- Resistance training adds benefit for insulin sensitivity
Step 2 - Treat Individual Components
A. Dyslipidemia
| Drug | Mechanism | Use |
|---|---|---|
| Statins (atorvastatin, rosuvastatin) | HMG-CoA reductase inhibitor → ↓ LDL | First-line for ASCVD risk reduction; also ↓ TG modestly, ↑ HDL slightly |
| Fibrates (fenofibrate, gemfibrozil) | PPARα agonist → ↑ LPL activity, ↓ apoC-III, ↑ β-oxidation | First-line for TG >500 mg/dL (pancreatitis prevention); ↓ TG ~30-50%; caution with statins (myopathy) |
| Omega-3 fatty acids (fish oil) | Reduce hepatic VLDL synthesis | TG >500 mg/dL; adjunct; IPE (icosapentaenoic acid) - CV benefit |
| Ezetimibe | Blocks NPC1L1 intestinal cholesterol absorption | Add-on to statin if LDL not at goal; ↓ LDL ~18% |
| PCSK9 inhibitors (evolocumab, alirocumab) | Block PCSK9 → more LDL receptors on hepatocytes | High ASCVD risk not controlled on statin + ezetimibe; ↓ LDL ~60% |
HDL: No specific drug currently approved just to raise HDL. Exercise and smoking cessation are most effective.
B. Hypertension
- Target BP: <130/80 mmHg (ACC/AHA 2017 guidelines)
- Preferred agents in MetS:
- ACE inhibitors / ARBs - first choice (reduce insulin resistance, protect kidney)
- Calcium channel blockers - metabolically neutral
- Avoid (or use cautiously):
- Beta-blockers - worsen insulin resistance, mask hypoglycemic symptoms, worsen TG, lower HDL (unless compelling indication e.g. post-MI, heart failure)
- Thiazide diuretics (at high dose) - raise glucose, TG, uric acid; lower K⁺
C. Hyperglycemia / Prevention of T2DM
- Lifestyle is the most effective T2DM prevention (>50% reduction in progression from prediabetes)
- Metformin - drug of choice if lifestyle is insufficient:
- Improves insulin sensitivity
- Reduces hepatic glucose output
- Does NOT cause weight gain (slight weight neutral or loss)
- Reduces progression from prediabetes to T2DM by ~31%
- GLP-1 Receptor Agonists (semaglutide, liraglutide, tirzepatide): major advance in MetS
- Promote weight loss, reduce TG, improve glycemia, reduce CV events
- Semaglutide 2.4 mg/week → average 14.9% weight loss over 68 weeks
- Tirzepatide (GIP + GLP-1 dual agonist) → up to 20.9% weight loss
D. Obesity Treatment (Harrison's 22e)
| Approach | Details |
|---|---|
| Behavioral/Lifestyle | Structured weight management programs; dietitian referral |
| Phentermine/topiramate ER | ~8% weight loss vs placebo; short-term use |
| Naltrexone/bupropion ER | ~10% weight loss in ~20% patients; avoid in seizure disorders, uncontrolled HTN |
| Liraglutide 3.0 mg | GLP-1 RA; ~6% weight loss vs placebo |
| Semaglutide 2.4 mg | GLP-1 RA; ~14.9% weight loss; currently best-in-class |
| Tirzepatide 15 mg | GIP+GLP-1 dual agonist; ~20.9% weight loss |
| Orlistat | Lipase inhibitor; ~30% fat absorption blocked; ~4% more weight loss; oily rectal leakage (poor adherence) |
| Bariatric surgery | BMI ≥40 OR ≥35 with comorbidities; gastric bypass/sleeve → dramatic improvement in ALL MetS components; survival benefit demonstrated |
Step 3 - Address Cardiovascular Risk
- ASCVD risk calculator (Pooled Cohort Equation) - calculate 10-year risk
- Aspirin: Low-dose (75-100 mg) in secondary prevention or high-risk primary prevention (discuss risk-benefit)
- Statins: High-intensity statin (atorvastatin 40-80 mg OR rosuvastatin 20-40 mg) for:
- LDL ≥190 mg/dL at any age
- T2DM aged 40-75 years with 10-year ASCVD risk ≥7.5%
- Established ASCVD
11. MONITORING
| Parameter | Frequency |
|---|---|
| Weight + waist circumference | Every visit |
| BP | Every visit |
| FBG / HbA1c | 3-6 monthly |
| Fasting lipid profile | 6-12 monthly initially, then annually |
| LFT (if on statins + NAFLD) | Baseline, then as needed |
| Urine microalbumin | Annually |
| ECG | Annually or when indicated |
| Ophthalmic review | Annually if T2DM develops |
12. EXAM SUMMARY TABLE - HIGH YIELD POINTS
| Point | Detail |
|---|---|
| Original name | Syndrome X (Reaven, 1988) |
| Central defect | Insulin resistance |
| Mandatory criterion (IDF) | Central obesity (waist >90/80 cm in Indians) |
| NCEP ATP III diagnosis | Any 3 of 5 criteria |
| Most atherogenic lipoprotein | Small dense LDL (formed when TG >180 mg/dL) |
| Best adipokine marker | Low adiponectin |
| Best drug to prevent T2DM | Lifestyle (>50% reduction); Metformin (31%) |
| Best drug for weight loss in MetS | Semaglutide (14.9% weight loss) |
| Preferred antihypertensive | ACE inhibitor / ARB |
| Antihypertensive to AVOID | Nonselective beta-blockers (worsen IR) |
| Best TG drug | Fibrates (TG >500 mg/dL - pancreatitis risk) |
| Marker of IR on skin | Acanthosis nigricans |
| Complication to screen | CVD, T2DM, NAFLD, CKD |
| Bariatric surgery threshold | BMI ≥40 OR ≥35 + comorbidities |
13. FREQUENTLY ASKED EXAM QUESTIONS
Q: What is the difference between MetS by WHO vs NCEP ATP III?
- WHO: Mandatory = insulin resistance/hyperglycemia + 2 others (including microalbuminuria)
- NCEP ATP III: Any 3 of 5 (no mandatory criterion; most clinical)
- IDF: Mandatory = central obesity (ethnic-specific cutoffs) + 2 others
Q: Why do Asians get MetS at lower BMI?
- Asians deposit more visceral fat at any given waist circumference compared to Caucasians
- Relative visceral:subcutaneous fat ratio is higher
- Therefore lower waist cutoffs are used (90 cm men, 80 cm women in Indians)
Q: What is HOMA-IR?
- Homeostatic Model Assessment of Insulin Resistance
- HOMA-IR = (Fasting Insulin in µIU/mL × Fasting Glucose in mg/dL) / 405
- Normal: <2.5; IR: >2.5
Q: Why is low HDL harmful in MetS?
- HDL normally performs reverse cholesterol transport (removes cholesterol from peripheral tissues to liver)
- In MetS: CETP exchanges HDL cholesterol for VLDL triglycerides → HDL becomes small, dense, protein-rich → rapidly cleared → low HDL → reduced reverse cholesterol transport → atherosclerosis
Q: Name the drugs used in metabolic syndrome.
- For TG: Fibrates, Omega-3 FA
- For LDL: Statins (first-line), Ezetimibe, PCSK9 inhibitors
- For HTN: ACE inhibitors / ARBs preferred
- For hyperglycemia/prevention: Metformin, GLP-1 RA
- For weight: GLP-1 RA (semaglutide, liraglutide), Orlistat, Bariatric surgery
Sources: Harrison's Principles of Internal Medicine 22e (2025), Chapter 420 - "The Metabolic Syndrome"; Basic Medical Biochemistry: A Clinical Approach 6e, Chapter 31
Generate a lecture presentation on metabolic syndrome pathophysiology and management
Reading File
Reading File
Reading File
Reading File
Running Command
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Generate a detailed study guide PDF for metabolic syndrome
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.