Give me a 10marks answer about ERAS Protocol in anaesthesia for AIIMS md anaesthesia exams
Reading File
Finding Sources
Searching PubMed
ERAS enhanced recovery after surgery anaesthesia
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content from Miller's Anesthesia and Schwartz's Principles of Surgery. I have enough to write a thorough 10-mark AIIMS MD Anaesthesia answer. Let me compile it now.
ERAS Protocol in Anaesthesia
Introduction
Enhanced Recovery After Surgery (ERAS) represents a multimodal, multidisciplinary, evidence-based approach to perioperative care aimed at attenuating the surgical stress response, accelerating functional recovery, and reducing postoperative morbidity. The concept was first described in 1995 by Professor Henrik Kehlet (Copenhagen) using early oral nutrition, early mobilization, and epidural analgesia for colonic surgery, with the median length of stay (LOS) reduced to 2 days. The ERAS Society (errassociety.org) was formally founded in 2001 by Professors Fearon and Ljungqvist and now publishes specialty-specific guidelines. The key principle is that individual interventions have modest independent benefit, but their synergistic multimodal application produces significant improvements in outcomes.
Pathophysiology Targeted by ERAS
Surgery triggers a neuroendocrine stress response - increased cortisol, catecholamines, ADH, glucagon - leading to:
- Insulin resistance and hyperglycemia
- Protein catabolism and muscle wasting
- Immunosuppression
- Fluid retention and third-spacing
- Ileus and impaired gut motility
- Pain sensitization
ERAS targets each of these in a structured pre-, intra-, and postoperative framework.
ERAS Pathway Components
A. PREOPERATIVE PHASE
| Intervention | Rationale |
|---|---|
| Patient education and counseling | Sets expectations, reduces anxiety, improves compliance |
| Nutritional optimization | Treat malnutrition/obesity before elective surgery; NRS-2002 screening |
| Prehabilitation | Exercise, physiotherapy, respiratory exercises (esp. for borderline lung function) |
| Smoking/alcohol cessation | At least 4 weeks prior - reduces cardiorespiratory complications |
| Optimization of comorbidities | Anemia correction (oral/IV iron, EPO), glycemic control, cardiac optimization |
| Preoperative fasting | Clear fluids until 2 hours before surgery; solids until 6 hours before (ASA/ERAS guidelines) |
| Oral carbohydrate loading | 12.5% maltodextrin drink 2-3 hours preoperatively (400 mL evening before, 200 mL 2 hours before). Reduces insulin resistance, improves protein balance, decreases LOS (evidence: RCTs in colorectal surgery) |
| Anxiolytic premedication | Avoid long-acting benzodiazepines (delay recovery); short-acting preferred if needed |
| No routine bowel preparation | Mechanical bowel prep increases dehydration and electrolyte disturbance without improving outcomes |
| Antibiotic prophylaxis | Within 60 minutes of incision; evidence: High quality, Strong recommendation |
| VTE prophylaxis | LMWH + compression stockings |
B. INTRAOPERATIVE PHASE
1. Anaesthetic Technique
- Prefer regional/neuraxial anaesthesia (or combined regional-general) over pure general anaesthesia when feasible - reduces opioid requirement, PONV, stress response, and facilitates early mobilization
- Short-acting anaesthetic agents: Propofol (TIVA preferred), desflurane/sevoflurane, remifentanil - allow rapid wake-up
- Avoid nitrous oxide - increases PONV, bowel distension
- BIS monitoring to avoid unnecessarily deep anaesthesia (target BIS 40-60) - reduces volatile agent use and delayed emergence
2. Opioid-Sparing / Multimodal Analgesia
This is the cornerstone of intraoperative ERAS anaesthesia. Opioids worsen ileus, PONV, respiratory depression, and cause hyperalgesia. Alternatives include:
- Paracetamol (1g IV) - routine preoperative/intraoperative dose
- NSAIDs / COX-2 inhibitors (e.g., celecoxib, ketorolac) - caution with anastomotic surgery (COX-2 may increase leak risk)
- Ketamine (0.1-0.5 mg/kg) - NMDA antagonist, prevents central sensitization
- Dexmedetomidine - alpha-2 agonist, opioid-sparing, reduces emergence agitation
- Lidocaine infusion (1.5 mg/kg/hr IV) - reduces pain, ileus, and opioid consumption
- Gabapentinoids (pregabalin/gabapentin) - pre-emptive analgesia
- Magnesium sulfate - NMDA antagonism
- Epidural analgesia - gold standard for open abdominal/thoracic surgery; reduces pulmonary complications, ileus, opioid use
- Paravertebral blocks, TAP blocks, erector spinae plane blocks, quadratus lumborum blocks - procedure-specific
3. Goal-Directed Fluid Therapy (GDFT)
- Avoid both hypovolemia (organ ischemia) and hypervolemia (anastomotic leak, pulmonary edema, ileus, delayed wound healing)
- Targets normovolemia with zero fluid balance
- Uses dynamic parameters: Stroke Volume Variation (SVV), Pulse Pressure Variation (PPV), Pleth Variability Index rather than static CVP/PCWP
- Monitoring devices: FloTrac/Vigileo, LiDCO, esophageal Doppler
- Avoid normal saline in large volumes - hyperchloremic metabolic acidosis associated with increased mortality; prefer balanced crystalloids (Plasmalyte, Hartmann's)
- Colloids (albumin) used selectively for volume replacement
4. Normothermia
- Maintain core temperature >36°C
- Use: Forced-air warming blankets (Bair Hugger), fluid warmers, increased theatre temperature
- Hypothermia causes: coagulopathy, immunosuppression, cardiac arrhythmias, delayed drug metabolism, prolonged neuromuscular blockade, increased infection risk
- Temperature monitoring is a strong recommendation (evidence: High)
5. Lung-Protective Ventilation
- Tidal volume 6-8 mL/kg ideal body weight
- PEEP 5-8 cmH2O
- FiO2 titrated to SpO2 94-98% (avoid hyperoxia)
- Periodic recruitment manoeuvres
- Reduces postoperative pulmonary complications (PPCs)
6. Minimally Invasive Surgery
- Laparoscopic/robotic approach preferred - less surgical stress response, reduced pain, early mobilization
- VATS (Video-Assisted Thoracoscopic Surgery) for lung cancer - strong recommendation
7. Avoid Routine Drains and NGT
- Routine nasogastric decompression delays GI recovery and increases pulmonary complications - not recommended
- Surgical drains removed early when used
8. PONV Prophylaxis
Risk-stratified per Apfel Score (female sex, non-smoker, history of PONV/motion sickness, postoperative opioid use - each scores 1 point):
- 0-1 risk factors: single agent (ondansetron OR dexamethasone)
- 2 risk factors: two agents (ondansetron + dexamethasone)
- 3-4 risk factors: three or more agents + TIVA (avoid volatile agents)
- Agents: ondansetron (4 mg IV), dexamethasone (4-8 mg at induction), scopolamine patch, droperidol, aprepitant (NK-1 antagonist)
C. POSTOPERATIVE PHASE
| Intervention | Details |
|---|---|
| Early oral feeding | Clear fluids within 4-6 hours, light diet within 24 hours. Early enteral nutrition reduces gut mucosal atrophy, bacterial translocation, infections |
| Early mobilization | Out of bed within 6-24 hours; reduces VTE, muscle wasting, insulin resistance, and chest complications. Nurse-led protocols critical |
| Multimodal oral analgesia | Paracetamol + NSAID scheduled doses; avoid routine opioids; PRN weak opioid (tramadol/codeine) only if needed |
| Early Foley removal | Within 24 hours of surgery where possible; reduces UTI and aids mobilization |
| Avoidance of IV fluids | Transition to oral fluids ASAP; excess IV fluids prolong ileus and delay discharge |
| Blood glucose control | Target 6-10 mmol/L; avoid both hypo- and hyperglycemia |
| Alvimopan / laxatives | Peripherally-restricted mu-opioid antagonist (alvimopan) for GI recovery in colorectal surgery |
| Audit and compliance monitoring | Regular review of ERAS compliance metrics and outcomes (LOS, readmission, complications) |
Outcomes and Evidence
- Length of stay reduced by 2-3 days across specialties
- Complication rates reduced 30-50% (respiratory, infectious, GI)
- Readmission rates comparable to or lower than conventional care
- Opioid consumption significantly reduced
- Cost savings substantial - lower hospitalization costs
- Ambulatory surgery facilitated: ERAS in ambulatory oncologic surgery centers showed same-day discharge rates increased from 7.2% to 58.6% (Miller's Anesthesia, 10e)
- For appendectomy (RCT, n=108): ERAS group discharged at mean 9.7 hrs vs 23.2 hrs with conventional care (Miller's Anesthesia, 10e)
Recent meta-analyses (2024-2025) confirm benefit across hip/knee arthroplasty, cardiac surgery, pancreaticoduodenectomy, and craniotomies (PMID: 38134323; 39952836; 39008960; 38651841).
ERAS vs Fast-Track Anaesthesia
| Feature | Fast-Track | ERAS |
|---|---|---|
| Focus | Speed of discharge | Quality of recovery |
| Scope | Primarily anaesthetic | Multidisciplinary (surgery, anaesthesia, nursing, physiotherapy, dietetics) |
| Endpoint | Discharge criteria met | Return to presurgical functional state |
| Evidence | Lower quality | Protocol-driven, high-quality |
Barriers to ERAS Implementation
- Resistance from surgeons/nurses to change from traditional practices
- Conflicting team recommendations
- Poor patient compliance (especially early feeding/mobilization)
- Resource limitations in low/middle-income countries
- Need for dedicated ERAS coordinators, audit infrastructure
Setting Up an ERAS Program
- Multidisciplinary team formation (anaesthesiologist, surgeon, nurse coordinator, dietitian, physiotherapist)
- Baseline audit of current practice
- Identification of evidence-based protocol elements for specialty
- Staff education and training
- Patient education materials
- Prospective data collection and compliance monitoring
- Regular feedback and iterative protocol refinement
Key Points for AIIMS Exam
- Founder: Henrik Kehlet, 1995; ERAS Society founded 2001
- Preoperative carbohydrate loading: 12.5% maltodextrin, 400 mL night before + 200 mL 2 hours before
- Fasting: Solids 6 hours, clear fluids 2 hours
- Intraoperative anaesthetic: TIVA (propofol), short-acting agents, BIS monitoring
- Opioid-sparing multimodal analgesia: Paracetamol + NSAID + ketamine + regional block + lignocaine infusion
- GDFT: SVV/PPV targets, balanced crystalloids, normovolemia
- PONV: Apfel score-based multimodal prophylaxis; avoid N2O and volatile agents
- Normothermia: Forced-air warming; strong evidence
- Lung-protective ventilation: 6-8 mL/kg TV, PEEP 5-8
- Postoperative: Early feeding within 6-24 hours, early mobilization within 24 hours, early removal of Foley/lines
References: Miller's Anesthesia, 10e (Block 27, p.10041-10042); Schwartz's Principles of Surgery, 11e (Chapter 50, p.2113-2124); Current Surgical Therapy, 14e; Scott-Brown's Otorhinolaryngology (ERAS section); PubMed PMIDs 38134323, 39952836, 39008960, 38651841.
Give me a 10marks answer about Oxygen Flux from standard textbooks for AIIMS md anaesthesia exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Excellent - I now have all the content needed for a complete, textbook-sourced 10-mark AIIMS answer. Let me compile it.
Oxygen Flux (Oxygen Delivery - DO₂) in Anaesthesia
Definition
Oxygen flux is synonymous with oxygen delivery (DO₂) - defined as the total amount of oxygen transported to the peripheral tissues per unit time by the cardiovascular system. It represents the supply side of the oxygen supply-demand equation and is the product of cardiac output and arterial oxygen content.
"Oxygen delivery, the rate at which oxygen is transported to the microcirculation, is the product of cardiac output and CaO₂ and is normally about 1,000 mL/min." - Mulholland & Greenfield's Surgery, 7e
Derivation of the DO₂ Formula
Step 1: Arterial Oxygen Content (CaO₂)
Oxygen is carried in blood in two forms:
- Bound to haemoglobin (Hb) - the dominant form
- Dissolved in plasma - minor but important at high PaO₂
$$\boxed{CaO_2 = (1.34 \times Hb \times SaO_2) + (0.003 \times PaO_2)}$$
Where:
- 1.34 mL/g = Hüfner's constant (oxygen-carrying capacity of 1 g of Hb; some texts use 1.36 or 1.39)
- Hb = haemoglobin concentration (g/dL)
- SaO₂ = arterial oxygen saturation (fraction)
- 0.003 = solubility coefficient of O₂ in plasma (mL/dL/mmHg)
- PaO₂ = partial pressure of O₂ in arterial blood (mmHg)
Normal CaO₂ ≈ 17-20 mL/dL (approximately 20 mL/dL)
Step 2: Oxygen Delivery (DO₂ / Oxygen Flux)
$$\boxed{DO_2 = CO \times CaO_2 \times 10}$$
Or expanded:
$$\boxed{DO_2 = CO \times [(1.34 \times Hb \times SaO_2) + (0.003 \times PaO_2)] \times 10}$$
Where:
- CO = cardiac output (L/min) = HR × SV
- ×10 = unit conversion factor (dL to mL)
Normal DO₂ ≈ 950-1,150 mL/min (conventionally ~1,000 mL/min)
Normal Values Table
(From Mulholland & Greenfield's Surgery, 7e - Table 10.1)
| Parameter | Equation | Normal Range | Units |
|---|---|---|---|
| Oxygen Delivery (DO₂) | CO × CaO₂ × 10 | 950-1,150 | mL/min |
| Arterial O₂ Content (CaO₂) | (SaO₂ × 1.38 × Hb) + (0.003 × PaO₂) | 17-20 | mL/dL |
| Oxygen Consumption (VO₂) | CO × (CaO₂ - CvO₂) × 10 | 200-250 | mL/min |
| Oxygen Extraction Ratio (OER) | VO₂/DO₂ × 100 | 22-30 | % |
| Mixed Venous SaO₂ (SvO₂) | (1 - VO₂/DO₂) × 100 | 60-80 | % |
| Cardiac Output (CO) | HR × SV/1000 | 4-8 | L/min |
Oxygen Consumption (VO₂) - The Demand Side
$$\boxed{VO_2 = CO \times (CaO_2 - CvO_2) \times 10}$$
Or: VO₂ = DO₂ × O₂ Extraction Ratio
- This is the Fick principle - the amount of O₂ consumed equals the difference between O₂ delivered and O₂ returned in venous blood
- Normal VO₂ ≈ 200-250 mL/min at rest
- In children: VO₂ ≈ 175 mL/min/m² (Miller's Anesthesia, 10e)
- Normal arteriovenous O₂ difference (a-vDO₂) = 4-6 mL/100 mL blood
Oxygen Extraction Ratio (OER / O₂ER)
$$\boxed{OER = \frac{VO_2}{DO_2} = \frac{CaO_2 - CvO_2}{CaO_2}}$$
- Normal OER = 22-30% (body normally extracts only ~25% of delivered O₂)
- Myocardium has the highest extraction ratio at ~75% - hence the heart is most vulnerable to reductions in DO₂
- Organs with high supply-to-demand ratios (kidney, skin, intestine) can increase extraction when DO₂ falls
DO₂-VO₂ Relationship: The Biphasic Curve (Critical Concept)
The relationship between oxygen delivery and consumption is biphasic:
1. Flow-Independent Zone (Physiological Range)
- VO₂ remains constant over a wide range of DO₂
- As DO₂ falls, compensatory increase in OER maintains VO₂
- Body uses compensatory mechanisms: increased HR, increased stroke volume, redistribution of blood flow
2. Critical DO₂ (DO₂ crit) - The Inflection Point
- The threshold below which VO₂ becomes dependent on DO₂
- In euvolemic adults with normal cardiac function: Critical DO₂ requires Hb ≥ 3-3.5 g/dL (Barash's Clinical Anaesthesia, 9e)
- Below this point: anaerobic metabolism begins, lactic acidosis develops
- "The level of oxygen delivery at which oxygen consumption begins to decrease is called critical oxygen delivery. At the critical oxygen delivery level, tissues begin to use anaerobic glycolysis, with resultant lactate production and metabolic acidosis." (Creasy & Resnik's Maternal-Fetal Medicine)
3. Flow-Dependent Zone (Pathological)
- VO₂ falls proportionally with DO₂
- Seen in: hemorrhagic shock, cardiogenic shock, severe anemia
- Lactic acidosis is the biochemical hallmark
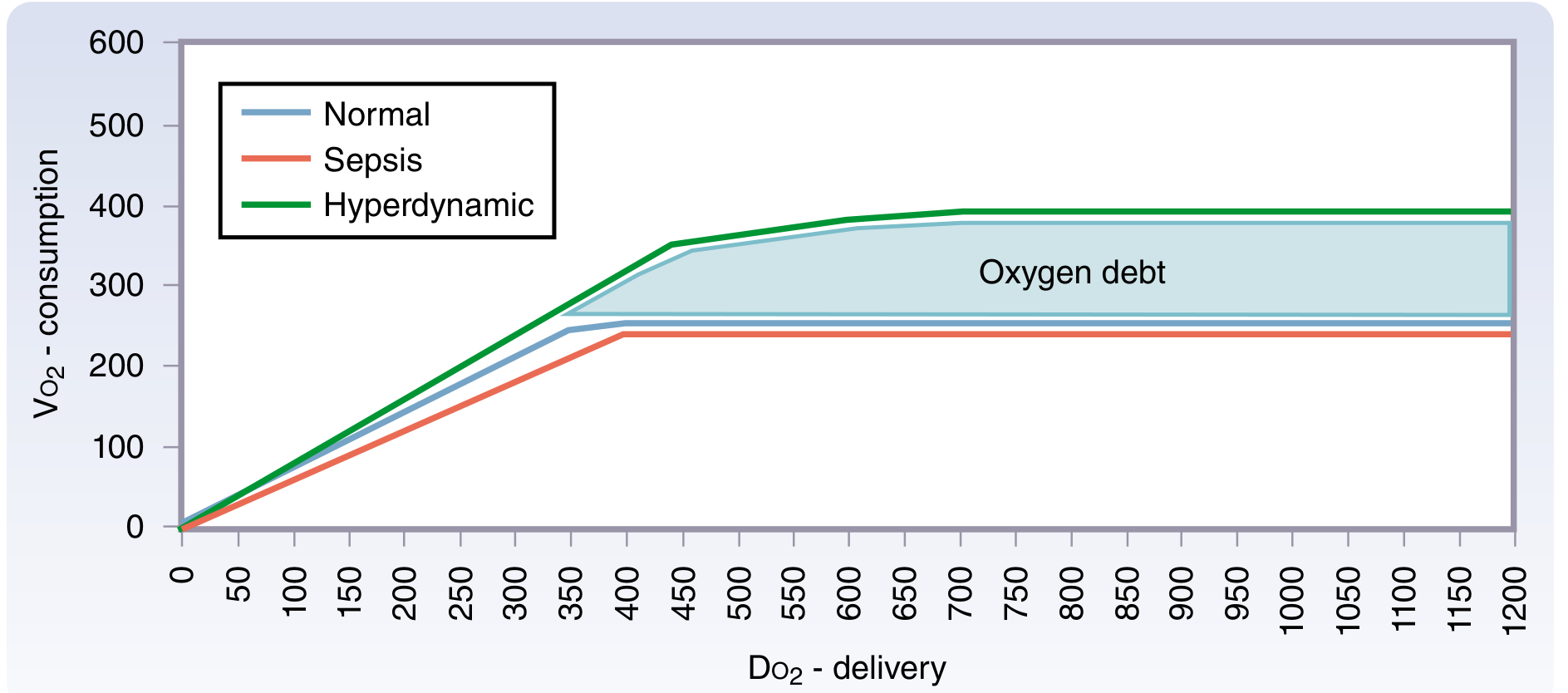
State-Specific Changes (from Sabiston, Fig. 33.9):
| State | DO₂-VO₂ Relationship |
|---|---|
| Normal | VO₂ independent over wide range; plateau at ~250 mL/min |
| Sepsis | VO₂ appears supply-dependent at higher DO₂ levels (pathological O₂ supply dependency) |
| Hyperdynamic (recovery) | Elevated VO₂ - paying back "oxygen debt" incurred during ischemia |
Mixed Venous Oxygen Saturation (SvO₂)
Rearranging the Fick equation (Miller's Anesthesia, 10e):
$$\boxed{SvO_2 = SaO_2 - \frac{VO_2}{CO \times 1.36 \times Hb}}$$
- Measured from pulmonary artery via PA catheter (true mixed venous sample from SVC + IVC + coronary sinus)
- Normal SvO₂: 60-80% (pulmonary artery)
- Normal ScvO₂: 65-85% (central venous - superior vena cava; slightly higher than SvO₂)
- Monitored continuously via reflectance oximetry (fiberoptic PAC)
Four Causes of Low SvO₂ (Fick Equation Analysis):
| Cause | Mechanism | Examples |
|---|---|---|
| ↓ SaO₂ | Reduced arterial saturation | Hypoxemia, V/Q mismatch |
| ↓ Hb | Reduced O₂-carrying capacity | Anemia, hemorrhage |
| ↓ CO | Reduced cardiac output | Cardiogenic shock, hypovolemia |
| ↑ VO₂ | Increased O₂ consumption | Fever, shivering, seizures, hyperthyroidism |
High SvO₂ (>80%):
- Septic shock (shunting of blood past tissues - reduced extraction)
- Cyanide/carbon monoxide poisoning (inability to utilize O₂)
- Hypothermia (reduced metabolic demand)
- Cirrhosis, hyperdynamic states
Determinants of DO₂ and How to Optimize Each
$$DO_2 = \underbrace{HR \times SV}{\text{CO}} \times \underbrace{[(1.34 \times Hb \times SaO_2) + (0.003 \times PaO_2)]}{\text{CaO}_2} \times 10$$
| Determinant | Way to Increase |
|---|---|
| Heart Rate | Treat bradycardia (atropine, pacing) |
| Stroke Volume | Optimize preload (fluids), reduce afterload (vasodilators), improve contractility (inotropes) |
| Haemoglobin | Blood transfusion, erythropoietin |
| SaO₂ | Supplemental O₂, PEEP, treat respiratory disease |
| PaO₂ | FiO₂ increase (minor contributor at normal Hb) |
"DO2 = CO × CaO₂; CO = HR × SV; CaO₂ = (Hb × 1.34 × SaO₂) + (0.003 × PaO₂). Commonly used ways of assessing both inadequate oxygen delivery and the response to treatment include SvO₂." - Scott-Brown's Otorhinolaryngology, Vol 1
Index Values (per m² Body Surface Area)
For comparison between patients of different sizes:
| Parameter | Indexed Value | Normal |
|---|---|---|
| DO₂I | DO₂/BSA | 520-570 mL/min/m² |
| VO₂I | VO₂/BSA | 110-160 mL/min/m² |
| Cardiac Index (CI) | CO/BSA | 2.5-4.0 L/min/m² |
Anaesthetic Implications
Intraoperative Effects on DO₂:
- General anaesthesia reduces CO by 10-20% (reduced preload, myocardial depression, vasodilation) → reduced DO₂
- Positive pressure ventilation reduces venous return and CO → reduces DO₂
- Volatile anaesthetics (halothane > isoflurane) reduce myocardial contractility → reduces CO
- Haemorrhage / blood loss → reduces Hb and CO → critical reduction in DO₂
- Hypothermia → reduces VO₂ (protective in cardiac/neuro surgery) but also reduces CO
- Vasopressors (noradrenaline) → increase afterload and MAP but may reduce CO at high doses
Clinical Monitoring of DO₂ Adequacy:
- SvO₂ monitoring via PAC (target >70%) - used in goal-directed therapy protocols (ERAS)
- ScvO₂ via central venous catheter (target >70%)
- Lactate - best surrogate for anaerobic metabolism (target <2 mmol/L)
- Base deficit on ABG
- NIRS (near-infrared spectroscopy) - regional cerebral/tissue oxygenation
- Urine output (>0.5 mL/kg/hr)
Transfusion Trigger (Barash's Clinical Anaesthesia, 9e):
- Stable, non-bleeding, euvolemic patients may tolerate Hb 6.0 g/dL
- Transfusion of some benefit between Hb 6-8 g/dL
- Rarely beneficial above Hb 10 g/dL
- Critical DO₂ requires minimum Hb 3-3.5 g/dL in normal cardiac function
Oxygen Debt and Shoemaker's Supranormalization
In 1980s, William Shoemaker showed that optimizing DO₂ beyond normal (supranormalization) improved outcome in high-risk surgical patients by repaying "oxygen debt" accumulated during shock. The DO₂ target was CO-driven optimization until VO₂ reached the flow-independent plateau (Sabiston Textbook of Surgery, 21e). This concept underpins modern goal-directed fluid therapy (GDFT) used in ERAS protocols.
Summary Points for AIIMS Exam
- DO₂ = CO × CaO₂ × 10 = normal ~1000 mL/min
- CaO₂ = (1.34 × Hb × SaO₂) + (0.003 × PaO₂) = normal ~20 mL/dL
- VO₂ = CO × (CaO₂ - CvO₂) × 10 = normal ~250 mL/min
- OER = VO₂/DO₂ = normal 22-30%; myocardium ~75%
- SvO₂ = 60-80% (PA); ScvO₂ = 65-85% (SVC)
- Critical DO₂ = threshold below which VO₂ becomes delivery-dependent; below Hb 3-3.5 g/dL in normal cardiac function
- Biphasic DO₂-VO₂ curve: flow-independent plateau → critical point → flow-dependent zone
- Low SvO₂ causes: ↓SaO₂, ↓Hb, ↓CO, ↑VO₂
- High SvO₂: sepsis (shunting), cyanide poisoning, hypothermia
- Anaesthesia reduces DO₂ via: ↓CO (myocardial depression, vasodilation), ↓preload (positive pressure ventilation), ↓Hb (blood loss)
References: Miller's Anesthesia 10e (blocks 13, 15, 31); Barash's Clinical Anaesthesia 9e (block 19, 20); Mulholland & Greenfield's Surgery 7e (block 3, Table 10.1); Sabiston Textbook of Surgery 21e (block 6, Fig 33.9); Fischer's Mastery of Surgery 8e (block 1); Scott-Brown's Otorhinolaryngology Vol 1 (Box 33.2)
This is a shared conversation. Sign in to Orris to start your own chat.