Flow chart for pathogenwsis of typhoidal salmonella
A detailed medical flowchart titled "Pathogenesis of Typhoidal Salmonella (Typhoid Fever)" showing the step-by-step disease progression. The flowchart flows top to bottom with labeled boxes and arrows connecting each stage: 1. INGESTION: "Ingestion of contaminated food or water containing S. typhi / S. paratyphi (requires ≥10²–10³ organisms)" 2. GASTRIC BARRIER: "Gastric acid kills many organisms → [Side note: Risk increases with reduced acidity (PPI use, gastrectomy, elderly)]" 3. SMALL INTESTINE: "Salmonellae reach small intestine" 4. EPITHELIAL INVASION: "S. typhi attaches to and penetrates M cells overlying Peyer's patches in terminal ileum → [SPI-1 type III secretion system injects effector proteins → Rho GTPase activation → actin rearrangement → bacterial uptake into phagosomes]" 5. PEYER'S PATCHES: "Uptake by mononuclear phagocytes (macrophages) in Peyer's patches → Peyer's patch hyperplasia → plateaulike elevations up to 8 cm → Mucosal ulcers oriented along long axis of ileum" 6. INTRACELLULAR SURVIVAL: "Bacteria survive within macrophage phagosomes (SPI-2 type III secretion) → resist oxidative killing → form non-replicating 'persisters' (relapse reservoir)" 7. LYMPHATIC SPREAD: "Spread to mesenteric lymph nodes → Reactive hyperplasia → bacteria-containing phagocytes accumulate" 8. PRIMARY BACTEREMIA (Week 1): "1st bacteremia → Blood culture positive in 90% → Systemic dissemination begins" 9. RETICULOENDOTHELIAL SEEDING: "Seeding of liver (typhoid nodules, focal necrosis), spleen (red pulp expansion, phagocyte hyperplasia), bone marrow, gallbladder → organisms multiply intracellularly" 10. SECONDARY BACTEREMIA (Week 2–3): "2nd sustained bacteremia → Rose spots on chest/abdomen → Sustained high fever 39–40°C plateau → Relative bradycardia, leukopenia" 11. TWO BRANCHES from secondary bacteremia: Left branch - INTESTINAL: "Organisms re-enter gut → Stool cultures positive from week 2 → Peyer's patch necrosis → Oval ulcers (long axis of ileum)" Right branch - COMPLICATIONS: "Intestinal hemorrhage & perforation | Encephalopathy, meningitis | Myocarditis, endocarditis | Cholecystitis | Pneumonia | Bone marrow suppression" 12. CARRIER STATE (bottom): "~1–4% → Chronic gallbladder colonization (associated with gallstones) → Long-term fecal shedding" Use clean professional medical diagram style with white background, blue/teal color scheme for the boxes, red for complications, gray for side notes. Clear readable fonts.
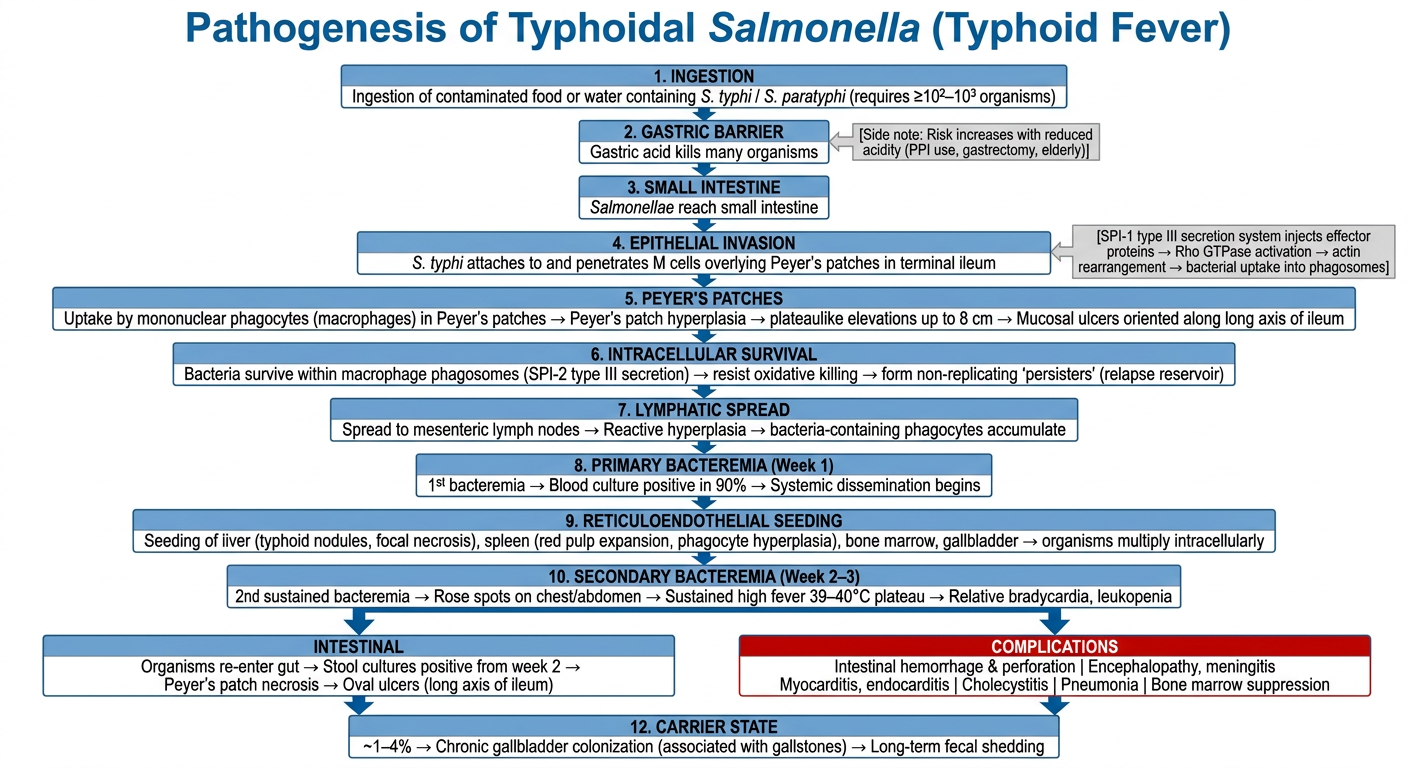
Pathogenesis of Typhoidal Salmonella - Step by Step
Stage 1 - Ingestion
- Contaminated food or water containing S. typhi or S. paratyphi is ingested
- Infective dose: ≥10²-10³ organisms in a normal host
- Risk increases when gastric acid is reduced (PPI use, gastrectomy, elderly, atrophic gastritis) - Goldman-Cecil Medicine
Stage 2 - Epithelial Invasion via M Cells
- Organisms reach the small intestine and attach to M cells overlying Peyer's patches in the terminal ileum
- The SPI-1 type III secretion system injects effector proteins into host cells
- These activate Rho GTPases → actin cytoskeletal rearrangement → bacterial uptake into phagosomes - Robbins Basic Pathology
Stage 3 - Peyer's Patch Involvement
- Bacteria are engulfed by mononuclear phagocytes (macrophages) in the subepithelial lymphoid tissue
- Peyer's patches undergo massive hyperplasia → plateau-like elevations up to 8 cm
- Mucosal shedding creates oval ulcers oriented along the long axis of the ileum - Robbins & Kumar Pathologic Basis of Disease
Stage 4 - Intracellular Survival
- S. typhi (unlike non-typhoidal Salmonella) survives and replicates within macrophage phagosomes using the SPI-2 secretion system
- A subpopulation forms non-replicating "persisters" - a reservoir for relapsing infection - Goldman-Cecil Medicine
Stage 5 - Lymphatic Spread
- Bacteria spread to mesenteric lymph nodes → reactive hyperplasia with accumulation of bacteria-laden phagocytes
- This is the key distinguishing step from non-typhoidal salmonellosis (which is blocked at the lamina propria by PMNs) - Goldman-Cecil Medicine
Stage 6 - Primary Bacteremia (Week 1)
- Entry into bloodstream via lymphatics
- Blood cultures positive in ~90% of cases during the febrile phase
- This is the optimal window for antibiotic intervention - Jawetz Medical Microbiology
Stage 7 - Reticuloendothelial Seeding
- Systemic dissemination seeds the liver (typhoid nodules, focal necrosis), spleen (red pulp expansion), bone marrow, and gallbladder
- Bacteria multiply intracellularly within these organs - Robbins Basic Pathology
Stage 8 - Secondary (Sustained) Bacteremia (Weeks 2-3)
- A second wave of bacteremia produces the classic clinical picture:
- Sustained fever at 39-40°C plateau
- Relative bradycardia (Faget's sign)
- Leukopenia (unlike bacterial sepsis)
- Rose spots - small erythematous maculopapular lesions on chest/abdomen (<5% of cases)
- Hepatosplenomegaly
Stage 9 - Complications (if untreated)
| System | Complication |
|---|---|
| GI | Intestinal hemorrhage, perforation (from Peyer's patch necrosis) |
| CNS | Encephalopathy, meningitis, seizures |
| Cardiac | Myocarditis, endocarditis |
| Hepatobiliary | Cholecystitis |
| Pulmonary | Pneumonia |
Stage 10 - Chronic Carrier State
- ~1-4% of patients develop a chronic carrier state
- S. typhi colonizes the gallbladder (facilitated by gallstones)
- Long-term fecal shedding sustains human-to-human transmission
- Humans are the sole reservoir for S. typhi - Jawetz Medical Microbiology
Key Virulence Factors Summary
| Factor | Role |
|---|---|
| SPI-1 T3SS | Invasion of M cells and enterocytes |
| SPI-2 T3SS | Intracellular survival in macrophages |
| Vi capsular antigen | Resistance to complement and phagocytosis |
| Pathogenicity islands | Encode the above secretion systems |