Pneumonia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"community-acquired pneumonia" AND management
Searching the Web
pneumonia clinical overview types diagnosis management 2025
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, clinician-level content from multiple authoritative textbooks plus the 2026 ATS guideline reference. Here is the full clinical overview:
Pneumonia: A Clinician's Overview
Definition
Pneumonia is an acute infection of the lung parenchyma associated with at least one respiratory symptom (cough, dyspnea, chest pain) and new opacities on lung imaging, with or without fever, in the absence of an alternative diagnosis. - Goldman-Cecil Medicine, Ch. 85
Classification
| Type | Definition | Key Pathogens |
|---|---|---|
| CAP (Community-Acquired) | Acquired outside hospital / within 48h of admission | S. pneumoniae, H. influenzae, Mycoplasma, Chlamydia, Legionella, respiratory viruses |
| HAP (Hospital-Acquired) | Develops ≥48h after admission | S. aureus (including MRSA), gram-negative bacilli (Pseudomonas, Klebsiella, Acinetobacter) |
| VAP (Ventilator-Associated) | Develops ≥48-72h after endotracheal intubation | Same gram-negatives + MRSA |
| Aspiration pneumonia | Aspiration of oropharyngeal/gastric contents | Anaerobes (Peptostreptococcus, Bacteroides, Fusobacterium), gram-negatives |
| Immunocompromised host | HIV, transplant, neutropenia, immunosuppressants | All of the above + PCP (P. jiroveci), Cryptococcus, Aspergillus, CMV, NTM |
Typical vs. Atypical Presentation
| Feature | Typical | Atypical |
|---|---|---|
| Onset | Sudden | Gradual |
| Cough | Productive | Dry |
| CXR | Lobar consolidation | Diffuse bilateral / interstitial infiltrates |
| Leukocytosis | Prominent | Often modest |
| Pathogens | S. pneumoniae, H. influenzae | Mycoplasma, Chlamydia, Legionella, viruses |
Pathology (Lobar Pneumococcal Pattern)
Four stages: edema (proteinaceous exudate + bacteria in alveoli) → red hepatization (erythrocytes fill alveoli) → gray hepatization (neutrophil predominance, fibrin deposition, bacterial clearance) → resolution (macrophages clear debris). - Harrison's 22e
Epidemiology
CAP is the most common infectious cause of hospitalization and death in the US. Hospitalization rates increase exponentially with age: ~1-2/1000 in young adults vs. ~40/1000 in adults ≥85. Mortality is ~6% during hospitalization and ~15% at 1 month for hospitalized patients. Acute cardiac events (new AF, heart failure, MI) occur in 20-25% of hospitalized CAP patients. Empyema complicates 3-5% of cases. - Goldman-Cecil Medicine
Etiology by Setting
| Setting | Key Pathogens |
|---|---|
| Outpatient | S. pneumoniae, Mycoplasma, H. influenzae, Chlamydia pneumoniae, respiratory viruses |
| Inpatient (non-ICU) | S. pneumoniae, Mycoplasma, C. pneumoniae, H. influenzae, Legionella, viruses |
| ICU | S. pneumoniae, S. aureus, Legionella spp., gram-negative bacilli, H. influenzae |
In >50% of cases, no clear pathogen is confirmed. Respiratory viruses account for 20-30% of CAP; this rose significantly during the COVID-19 pandemic. - Goldman-Cecil, Harrison's
Epidemiological Clues to Pathogen (Selected)
| Exposure / Condition | Suspect Pathogen |
|---|---|
| Aspiration / poor dentition | Anaerobes, Candida |
| SW United States travel | Coccidioides immitis |
| Mississippi River basin / bats | Histoplasma capsulatum |
| Farm animals | Coxiella burnetii (Q fever) |
| Psittacine bird exposure | Chlamydia psittaci |
| Rabbit exposure | Francisella tularensis |
| Active influenza in community | Influenza, S. aureus, S. pneumoniae |
| Bronchiectasis / CF | Pseudomonas, MRSA, Aspergillus |
| HIV early | S. pneumoniae, H. influenzae, TB |
| HIV/AIDS (CD4 low) | All above + PCP, Cryptococcus, MAI, CMV |
Clinical Features & Diagnosis
Symptoms: Fever, cough (productive in typical; dry in atypical), purulent sputum, pleuritic chest pain, dyspnea, rigors.
Signs: Tachypnea, tachycardia, fever, dullness to percussion, bronchial breath sounds, crackles, egophony ("e" sounds like "a" over consolidation), whispered pectoriloquy.
Workup:
- Chest imaging - CXR is standard; lung ultrasound now accepted as an alternative (2025 ATS guideline update)
- Sputum gram stain + culture - before antibiotics if possible; sensitivity is limited
- Blood cultures - in all hospitalized patients; yield is low but important for bacteremia detection
- Urinary antigens - Legionella urinary antigen (in severe CAP or local outbreak); Streptococcal urinary antigen (in severe CAP)
- PCR - for SARS-CoV-2 and influenza routinely; MRSA nasal PCR to guide anti-MRSA therapy; respiratory multiplex PCR panels now include Mycoplasma, Chlamydia
- Procalcitonin / CRP - adjunctive; helps distinguish bacterial from viral; guides antibiotic de-escalation
- ABG - to assess severity and oxygenation
Severity Assessment & Site of Care
CURB-65 (Practical Bedside Tool)
| Criterion | Points |
|---|---|
| Confusion | 1 |
| Urea >7 mmol/L (BUN >19 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure - systolic ≤90 or diastolic ≤60 mmHg | 1 |
| Age ≥65 | 1 |
- Score 0: Outpatient (30-day mortality 1.5%)
- Score 1-2: Hospitalize (consider outpatient if score 1 is solely age ≥65)
- Score ≥3: ICU admission may be needed (30-day mortality ~22%)
PSI (Pneumonia Severity Index)
Uses 20 variables. Assigns patients to 5 classes with mortality: Class 1 (0.1%) → Class 5 (29.2%). Better validated than CURB-65 but requires a calculator. PSI is superior for identifying low-risk patients; CURB-65 is faster.
Severe CAP Criteria (IDSA/ATS) - ICU Admission
Major criteria (any 1 = direct ICU):
- Septic shock requiring vasopressors
- Invasive mechanical ventilation
Minor criteria (≥3 = ICU/high monitoring):
-
RR ≥30/min
-
PaO2/FiO2 ≤250
-
Multilobar infiltrates
-
Confusion/disorientation
-
Uremia (BUN ≥20 mg/dL)
-
Leukopenia (WBC <4,000/µL)
-
Thrombocytopenia (<100,000/µL)
-
Hypothermia (<36°C)
-
Hypotension requiring aggressive fluid resuscitation
-
Harrison's 22e
Diagnostic Pathway (CAP)
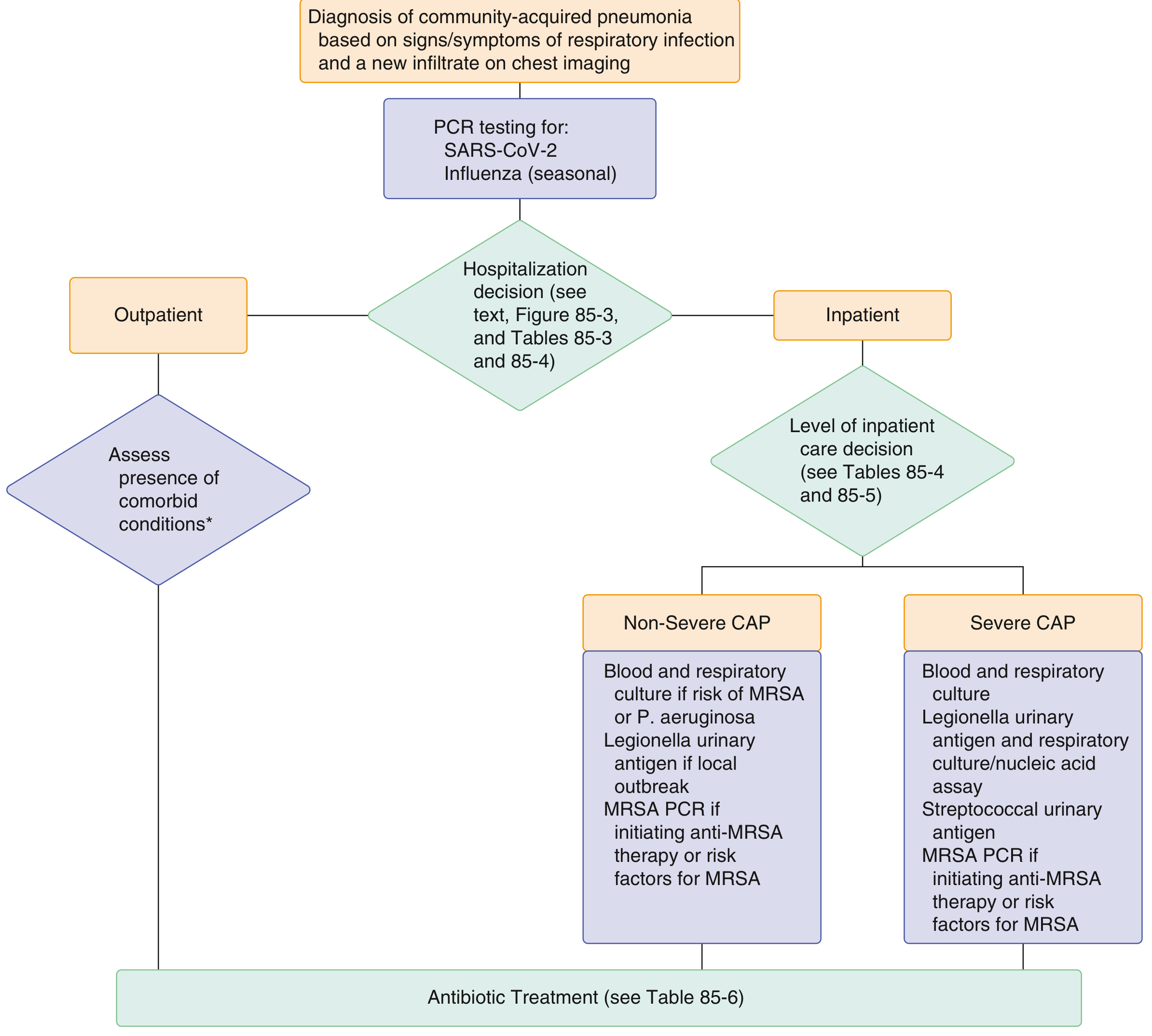
Treatment
Antibiotic Regimens (per Goldman-Cecil / 2025 ATS Guidelines)
Outpatient - No Comorbidities (Healthy Adult):
- Amoxicillin 1 g TID, OR
- Doxycycline 100 mg BID, OR
- Macrolide (azithromycin, clarithromycin) - only if local resistance <25%
Outpatient - With Comorbidities (chronic heart/lung/liver/renal disease, diabetes, alcoholism, malignancy, asplenia):
- Beta-lactam + macrolide combination, OR
- Respiratory fluoroquinolone (levofloxacin 750 mg daily, moxifloxacin 400 mg daily, or gemifloxacin)
Inpatient - Non-Severe CAP, No MRSA/Pseudomonas Risk:
- Beta-lactam (ampicillin, cefotaxime, ceftriaxone) + macrolide (azithromycin or clarithromycin), OR
- Respiratory fluoroquinolone monotherapy (levofloxacin, moxifloxacin), OR
- If macrolide + fluoroquinolone both contraindicated: beta-lactam + doxycycline
Inpatient - Severe CAP, No MRSA/Pseudomonas Risk:
- Beta-lactam + macrolide, OR beta-lactam + respiratory fluoroquinolone
With MRSA Risk/Confirmed:
- Vancomycin 15 mg/kg q12h (adjust by levels), OR linezolid 600 mg q12h (preferred by some for better lung penetration + exotoxin inhibition)
With Pseudomonas Risk:
- Piperacillin-tazobactam 4.5 g q6h, cefepime 2 g q8h, ceftazidime, aztreonam, meropenem, or imipenem
Viral Pneumonia:
- SARS-CoV-2: per current COVID-19 protocols
- Influenza: oseltamivir 75 mg BID x 5 days + cover bacterial coinfection
Newer Agents:
- Omadacycline and lefamulin (pleuromutilins) are options when beta-lactams are contraindicated.
Antibiotic Duration
The 2025/2026 ATS update emphasizes shorter courses: stable patients can be treated for 5 days (vs. traditional 7-10), with de-escalation based on clinical response and procalcitonin trends. A new 2026 ATS Practice Guideline (PMID 40679934) updates recommendations on imaging, antibiotic selection, treatment duration, and corticosteroid use.
Corticosteroids
The 2025 ATS update limits adjunctive corticosteroids to severe inpatient CAP only - not recommended routinely for non-severe disease.
Supportive Care
- Supplemental O2 to target SpO2 ≥92-94%; high-flow nasal cannula or NIV for hypoxic respiratory failure
- IV fluids for dehydration/sepsis
- Antipyretics, DVT prophylaxis, early mobilization
HAP & VAP Management
HAP/VAP is more frequently caused by S. aureus (including MRSA) and gram-negative bacilli. Empirical coverage targets these organisms based on local antibiogram data. De-escalation upon culture results is standard. - Goldman-Cecil Medicine
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | 3-5% of CAP; requires pleural drainage if exudative/loculated |
| Lung abscess | Especially with anaerobes, S. aureus, aspiration |
| Sepsis / Septic shock | Warrants ICU admission |
| ARDS | Most common with Legionella, gram-negatives, viral |
| Acute cardiac events | AF, new HF, myocardial ischemia - 20-25% of hospitalized cases |
| Multi-organ failure | In severe cases |
Prevention
- Pneumococcal vaccine: PCV15 or PCV20 for all adults ≥65 and high-risk adults 19-64 (chronic heart/lung/liver/renal disease, DM, alcohol use disorder, smokers, asplenia, immunocompromised)
- Influenza vaccine: annually for all ≥6 months; especially important in elderly, pregnant women, chronic disease
- COVID-19 vaccine: recommended for all adults and children ≥6 months
- Lifestyle: smoking cessation; caution with opioids, PPIs, and corticosteroids (all increase pneumonia risk); good hand hygiene and masking when symptomatic
2026 ATS Guideline Update (Key Changes)
A new official ATS Clinical Practice Guideline (Jan 2026, PMID 40679934) updates the previous 2019 ATS/IDSA guidelines with four focus areas:
- Imaging: Lung ultrasound is now an accepted alternative to CXR for diagnosis
- Antibiotics: More selective empiric prescribing; antibiotics not needed when viral etiology is confirmed without bacterial coinfection
- Duration: Shorter antibiotic courses for stable patients (5 days)
- Corticosteroids: Adjunctive corticosteroids only for severe inpatient CAP, not routine use
Primary sources: Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22e (2025); Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Frameworks for Internal Medicine. Guidelines: 2026 ATS/IDSA CAP Guideline (PMID 40679934).
For medical student notes purpose
Here are clean, exam-ready medical student notes on pneumonia:
🫁 PNEUMONIA - Medical Student Notes
DEFINITION
Acute infection of the lung parenchyma causing:
- Respiratory symptoms (cough, dyspnea, chest pain)
- New infiltrate on chest imaging
- ± Fever
CLASSIFICATION
By Acquisition
| Type | Definition |
|---|---|
| CAP | Outside hospital OR <48h of admission |
| HAP | ≥48h after hospital admission |
| VAP | ≥48-72h after intubation |
| Aspiration | Inhalation of oropharyngeal/gastric contents |
By Pattern
| Typical | Atypical | |
|---|---|---|
| Onset | Sudden | Gradual |
| Cough | Productive | Dry |
| CXR | Lobar consolidation | Diffuse/interstitial infiltrates |
| WBC | High (neutrophilia) | Normal/mildly elevated |
| Pathogens | S. pneumoniae, H. influenzae | Mycoplasma, Chlamydia, Legionella, viruses |
ETIOLOGY (HIGH YIELD)
CAP - Most Common Organisms
| Setting | Top Pathogens |
|---|---|
| Outpatient | S. pneumoniae #1, Mycoplasma, H. influenzae, Chlamydia, viruses |
| Inpatient (non-ICU) | S. pneumoniae, Mycoplasma, Legionella, H. influenzae |
| ICU | S. pneumoniae, S. aureus, Legionella, gram-negatives |
⚠️ In >50% of CAP cases, no pathogen is ever identified
HAP/VAP
- S. aureus (MRSA), Pseudomonas aeruginosa, Klebsiella, Acinetobacter
Aspiration
- Anaerobes (Peptostreptococcus, Bacteroides, Fusobacterium) → lung abscess, empyema
- Gram-negatives in hospitalized patients → fulminant course
Special Associations (MEMORIZE)
| Clue | Pathogen |
|---|---|
| Birds (parrots/parakeets) | Chlamydia psittaci |
| Farm animals | Coxiella burnetii (Q fever) |
| Bats / Mississippi River basin | Histoplasma capsulatum |
| SW United States desert | Coccidioides immitis |
| Rabbits | Francisella tularensis |
| Post-influenza | S. aureus, S. pneumoniae |
| Bronchiectasis/CF | Pseudomonas, MRSA, Aspergillus |
| HIV (early, CD4 >200) | S. pneumoniae, H. influenzae, TB |
| HIV/AIDS (CD4 <200) | PCP (P. jiroveci), Cryptococcus, Aspergillus, CMV |
PATHOLOGY (Lobar Pneumococcal - 4 Stages)
- Congestion/Edema - Protein exudate + bacteria fill alveoli
- Red Hepatization - RBCs + neutrophils fill alveoli; lung is red, firm, liver-like
- Gray Hepatization - RBCs lysed; neutrophils + fibrin dominate; bacteria cleared
- Resolution - Macrophages clear debris; normal architecture restored
CLINICAL FEATURES
Symptoms
- Fever, rigors, malaise
- Cough (productive or dry)
- Purulent/rust-colored sputum (pneumococcal)
- Pleuritic chest pain
- Dyspnea
Signs
| Sign | Mechanism |
|---|---|
| Dullness to percussion | Alveolar consolidation |
| Bronchial breath sounds | Sound conducted through consolidated lung |
| Crackles (crepitations) | Alveolar fluid |
| Egophony | "E" → "A" over consolidation |
| Whispered pectoriloquy | Whispered sounds heard clearly over consolidation |
| Reduced chest expansion | Ipsilateral side |
INVESTIGATIONS
Bedside / Basic
- CXR - lobar consolidation (typical) vs. interstitial/bilateral (atypical/viral)
- Pulse oximetry - SpO2 <92% = hospitalize
- ABG - assess hypoxia and hypercapnia in severe disease
Bloods
- FBC - leukocytosis (bacterial), lymphopenia (viral)
- U&E - urea used in CURB-65
- CRP / Procalcitonin - guide antibiotic start/stop
- Blood cultures - 2 sets before antibiotics
Microbiology
- Sputum gram stain + culture (before antibiotics)
- Legionella urinary antigen (severe CAP or local outbreak)
- Pneumococcal urinary antigen (severe CAP)
- Influenza + SARS-CoV-2 PCR (routine)
- MRSA nasal PCR (if considering anti-MRSA therapy)
Imaging
- CXR standard; lung ultrasound now accepted as alternative (2026 ATS guideline)
- CT chest: if CXR unclear, suspected complication, or immunocompromised
SEVERITY SCORING
CURB-65 (Quick Bedside Tool)
| Letter | Criterion | Points |
|---|---|---|
| C | Confusion (new) | 1 |
| U | Urea >7 mmol/L | 1 |
| R | Respiratory rate ≥30/min | 1 |
| B | BP - systolic <90 or diastolic <60 mmHg | 1 |
| 65 | Age ≥65 years | 1 |
| Score | Action | 30-day Mortality |
|---|---|---|
| 0 | Outpatient | 1.5% |
| 1-2 | Hospitalize | ~9% |
| ≥3 | Consider ICU | ~22% |
ICU Criteria (IDSA/ATS) - Severe CAP
Major (any 1 = ICU):
- Septic shock requiring vasopressors
- Mechanical ventilation required
Minor (≥3 of 9 = ICU):
- RR ≥30/min
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Confusion
- BUN ≥20 mg/dL
- WBC <4,000/µL
- Platelets <100,000/µL
- Temp <36°C
- Hypotension needing aggressive fluids
TREATMENT
Antibiotic Selection
Outpatient - Healthy, No Comorbidities:
- Amoxicillin 1 g TID, OR
- Doxycycline 100 mg BD, OR
- Macrolide (only if local resistance <25%)
Outpatient - With Comorbidities:
- Beta-lactam + macrolide, OR
- Respiratory fluoroquinolone (levofloxacin, moxifloxacin)
Inpatient - Non-Severe:
- Beta-lactam (ceftriaxone/ampicillin) + macrolide (azithromycin), OR
- Respiratory fluoroquinolone monotherapy
Inpatient - Severe:
- Beta-lactam + macrolide, OR
- Beta-lactam + respiratory fluoroquinolone
Add for MRSA:
- Vancomycin 15 mg/kg q12h, OR
- Linezolid 600 mg q12h (preferred - better lung penetration, inhibits exotoxin)
Add for Pseudomonas:
- Pip-tazo, cefepime, ceftazidime, aztreonam, meropenem, or imipenem
Influenza: Oseltamivir 75 mg BD x 5 days + cover bacterial coinfection
Duration (2026 ATS Update)
- 5 days for stable patients responding to treatment
- Traditional 7-10 days for severe/complicated disease
- De-escalate based on clinical response + procalcitonin
Corticosteroids (2026 ATS Update)
- Adjunctive steroids: severe inpatient CAP only
- NOT recommended routinely for non-severe disease
Supportive
- O2 to SpO2 ≥92-94%
- HFNC or NIV for hypoxic respiratory failure
- IV fluids (sepsis protocol if shocked)
- Antipyretics, DVT prophylaxis, early mobilization
COMPLICATIONS
| Complication | Key Points |
|---|---|
| Parapneumonic effusion / Empyema | 3-5% of CAP; drain if exudative or loculated |
| Lung abscess | Anaerobes, S. aureus, aspiration; prolonged antibiotics |
| Sepsis / Septic shock | ICU; vasopressors |
| ARDS | Legionella, gram-negatives, viral; mechanical ventilation |
| Acute cardiac events | New AF, heart failure, MI - occurs in 20-25% of hospitalised CAP |
| Pleural effusion | Light's criteria to distinguish exudate vs. transudate |
PREVENTION
| Vaccine | Target Population |
|---|---|
| Pneumococcal (PCV15 / PCV20) | All adults ≥65; high-risk adults 19-64 (DM, CLD, CKD, CHD, smokers, asplenia, immunocompromised) |
| Influenza | Annual for all ≥6 months; especially elderly, pregnant, chronic disease |
| COVID-19 | All adults and children ≥6 months |
Other: smoking cessation; avoid unnecessary opioids, PPIs, and steroids (all increase pneumonia risk)
HIGH-YIELD EXAM POINTS ⭐
- Most common cause of CAP: S. pneumoniae
- Most common cause of atypical CAP in young adults: Mycoplasma pneumoniae
- Rust-colored sputum: S. pneumoniae
- "Currant jelly" sputum: Klebsiella pneumoniae (alcoholics, diabetics)
- Pneumatoceles on CXR in infants/young: S. aureus
- "Atypical" CAP + hyponatremia + high fever + GI symptoms + Legionnaire's disease history: Legionella - treat with respiratory fluoroquinolone or azithromycin; urinary antigen test
- Walking pneumonia (mild, treated outpatient): Mycoplasma
- Post-influenza superinfection: S. aureus (MRSA especially)
- Pneumonia + diarrhea + hyponatremia + elevated LFTs + no response to beta-lactams: Legionella
- Egophony: "E" → "A" sound over consolidation (whispered pectoriloquy also positive over consolidation)
- No pathogen found in: >50% of CAP
Sources: Goldman-Cecil Medicine; Harrison's Principles 22e (2025); Murray & Nadel's Respiratory Medicine; 2026 ATS CAP Clinical Practice Guideline (PMID 40679934)
This is a shared conversation. Sign in to Orris to start your own chat.