Hydrocephalus treatment
Reading File
Finding Sources
Searching PubMed
hydrocephalus treatment shunt endoscopic
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough overview of hydrocephalus treatment based on authoritative surgical and neurology textbooks.
Hydrocephalus: Treatment
1. Goals of Treatment
The primary goal is to restore normal CSF dynamics - either by removing the cause of obstruction, diverting excess CSF, or creating an alternate drainage pathway. Treatment is determined by whether hydrocephalus is acute or chronic, obstructive or communicating, and the patient's age.
2. Emergency Management
Acute obstructive hydrocephalus is a neurosurgical emergency due to the risk of rapid ICP rise, coma, and death (sometimes with sudden "hydrocephalic attacks").
- Address the underlying cause first when possible (e.g., tumour excision causing obstruction).
- Temporary ventricular drainage is needed when waiting for definitive surgery or in a deteriorating patient.
For acute ICP elevation (pediatric or adult): manage with standard ICP protocols (head elevation, osmotherapy, hyperventilation as a bridge).
3. Temporary CSF Diversion
External Ventricular Drain (EVD)
- Inserted through a burr hole at Kocher's point (right of midline, anterior to the coronal suture), perpendicular to the brain surface.
- Catheter tip rests adjacent to the foramen of Monro in the lateral ventricle.
- Can also be used to deliver intrathecal antibiotics.
- Lumbar drains are an alternative for communicating hydrocephalus.
Medical (Temporary)
- Acetazolamide (carbonic anhydrase inhibitor) + furosemide: reduces the rate of CSF production; used for slowly progressive hydrocephalus as a bridge to surgery, particularly in infants/neonates. Clinical effects are limited and not sustained long term.
- Not appropriate as definitive management.
4. Definitive Surgical Treatment
A. Ventriculoperitoneal (VP) Shunt - MAINSTAY
The VP shunt is the standard long-term treatment for most types of hydrocephalus.
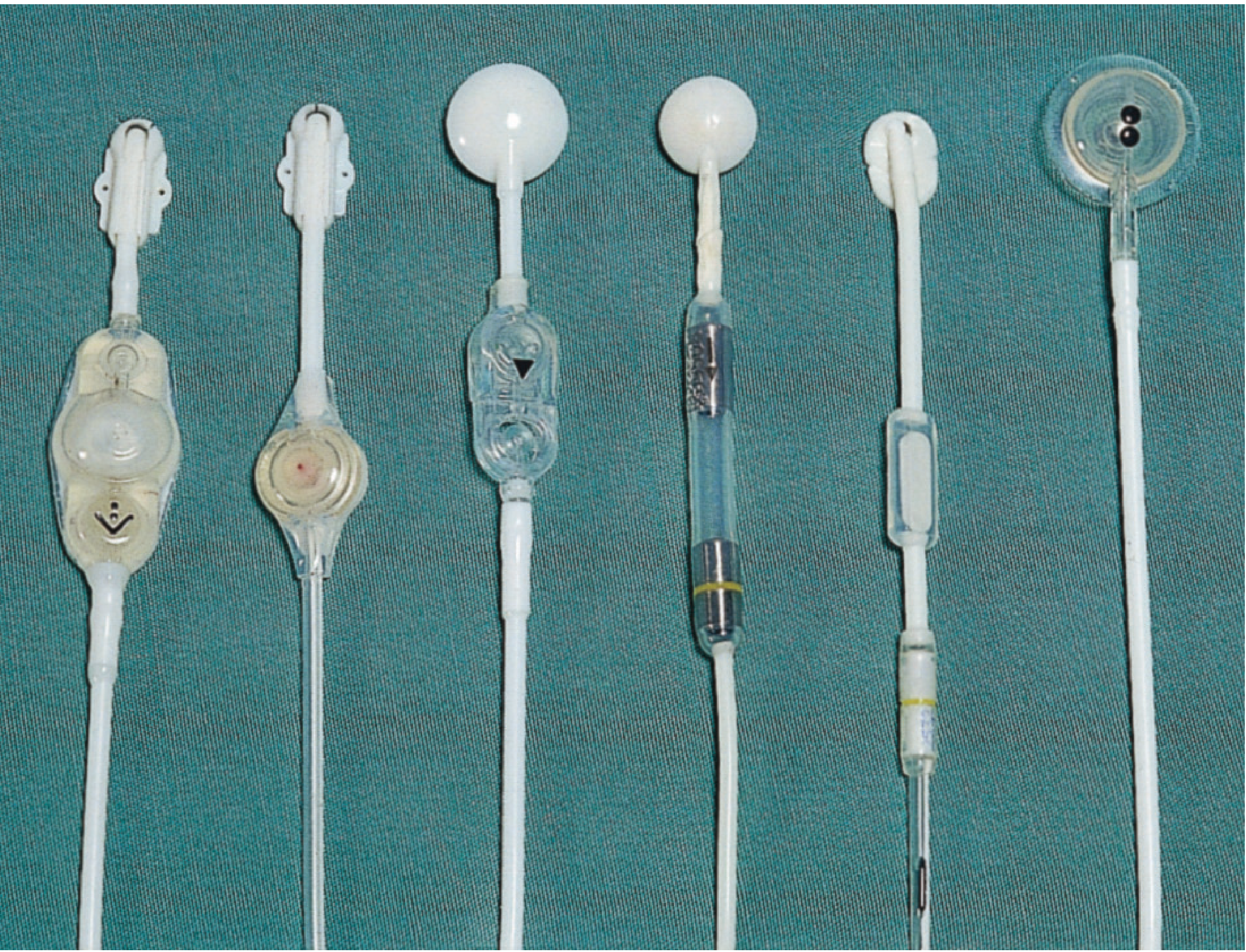
Components:
- Proximal (ventricular) catheter - inserted into the lateral ventricle
- Shunt valve - regulates flow by opening at a preset pressure; usually incorporates a CSF reservoir for percutaneous sampling
- Distal catheter - tunnelled subcutaneously to the peritoneal cavity
- Optional: anti-siphon device to prevent overdrainage in the upright position
- Programmable valves - allow the opening pressure to be adjusted non-invasively using an external magnetic device
Alternative shunt destinations (less common):
- Ventriculoatrial (VA) shunt
- Ventriculopleural shunt
- Lumboperitoneal shunt (for communicating hydrocephalus)
B. Endoscopic Third Ventriculostomy (ETV)
- Especially useful for obstructive hydrocephalus (e.g., aqueduct stenosis).
- A neuroendoscope is passed into the frontal horn of the lateral ventricle, then through the foramen of Monro into the third ventricle.
- The floor of the third ventricle is opened between the mamillary bodies and the pituitary recess.
- Creates a bypass from the third ventricle to the basal subarachnoid cisterns - no implanted hardware, so no infection risk from tubing.
- ETV + Choroid Plexus Cauterization (ETV-CPC): combined procedure shown to be effective in >70% of patients with myelomeningocele, avoiding the need for VP shunting with similar neurocognitive outcomes. - Campbell-Walsh-Wein Urology
- Limitations: reblockage is common; many patients subsequently require a shunt. Long-term results have been disappointing as a primary approach in some series. - Adams and Victor's Principles of Neurology, 12th Ed.
Serious complications of ETV: basilar artery injury, fornix damage (permanent memory impairment).
5. Shunt Complications (15-20% require revision within 3 years)
| Complication | Features | Management |
|---|---|---|
| Infection | Fever, headache, meningism; 75% within 1 month of insertion | Remove shunt + EVD/serial LP + antibiotics; reinsert at new site after CSF normalizes |
| Blockage | Features of raised ICP; reservoir difficult to compress | Urgent - can be emergency in obstructive hydrocephalus; revise shunt |
| Overdrainage | Low-pressure headaches (worse standing), subdural hygroma/haematoma | Replace valve with higher opening pressure; add anti-siphon device |
| Slit ventricle syndrome | Children with underdeveloped ventricles, poor compliance; ICP spikes with coughing/straining | Raise valve opening pressure; place anti-siphon device |
| Disconnection/migration | Signs of raised ICP | Revision |
Shunt blockage causes: cellular/proteinaceous debris, infection, choroid plexus adhesion, blood clot, or valve failure.
6. Special Scenarios
Normal Pressure Hydrocephalus (NPH)
- Classic triad: gait disturbance, urinary incontinence, cognitive decline.
- Treated with VP shunting - ventricular size can normalize within 1-2 weeks.
- Gait disturbance improves more slowly than cognitive symptoms.
- Acetazolamide has minimal clinical effect in NPH, despite some imaging improvement. - Adams and Victor's, 12th Ed.
Idiopathic Intracranial Hypertension (IIH)
- Managed with weight loss, acetazolamide, serial lumbar puncture.
- CSF diversion (VP shunt or lumboperitoneal shunt) is a last resort. - Bailey and Love's, 28th Ed.
Infantile/Congenital Hydrocephalus
- VP shunting is standard; ETV-CPC is an effective shunt-sparing alternative in many cases.
- Risk of slit ventricle syndrome is higher in young children with early shunting.
- Whether to shunt all hydrocephalic infants at birth is controversial given the relatively low proportion surviving with normal mental function in several series. - Adams and Victor's, 12th Ed.
7. Summary
| Method | Type | Indication |
|---|---|---|
| EVD | Temporary | Acute/emergency, pre-op |
| Acetazolamide + furosemide | Medical (temporary) | Slowly progressive; bridge in infants |
| VP Shunt | Definitive | Most types of hydrocephalus |
| ETV | Definitive | Obstructive (especially aqueduct stenosis) |
| ETV + CPC | Definitive | Myelomeningocele, infants |
| Lumboperitoneal shunt | Definitive | Communicating hydrocephalus, IIH |
Sources:
- [Bailey and Love's Short Practice of Surgery, 28th Ed.](Bailey and Love's Short Practice of Surgery, 28th Ed., p. 727)
- [Adams and Victor's Principles of Neurology, 12th Ed.](Adams and Victor's Principles of Neurology, 12th Ed., p. 640)
- [The Harriet Lane Handbook, 23rd Ed.](The Harriet Lane Handbook, 23rd Ed.)
- [Campbell-Walsh-Wein Urology](Campbell-Walsh-Wein Urology, 3-Volume Set)
- Recent PubMed: PMID 41525875 - 2026 systematic review on low/negative pressure hydrocephalus management; PMID 40825578 - 2025 systematic review on fetal hydrocephalus surgical interventions.
This is a shared conversation. Sign in to Orris to start your own chat.