Aeriation pathways of middle ear
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Cummings Otolaryngology. Let me now compile the full answer with the textbook content.
Aeration Pathways of the Middle Ear
The aeration of the middle ear depends on a well-defined system of pathways that carry air from the Eustachian tube through the various middle ear subspaces and ultimately into the mastoid. The key concept governing these pathways is the epitympanic diaphragm.
The Epitympanic Diaphragm
The ligamentous and mucosal fold structures of the epitympanum together form the epitympanic diaphragm - a partial partition that separates the epitympanum from the mesotympanum and determines how air circulates through the middle ear and mastoid. The components include:
| Structure | Role |
|---|---|
| Anterior malleal ligament and fold | Forms anterior wall of diaphragm |
| Lateral malleal fold | Lateral boundary |
| Lateral incudomalleal fold (imlf) | Divides posterior epitympanum into superior/inferior attic |
| Posterior incudal ligament | Posterior anchor |
| Tensor fold (tf) | Separates anterior epitympanic space from mesotympanum; critical gate for aeration |
The blue arrow in the diagram below indicates the tympanic isthmus - the primary aeration pathway:
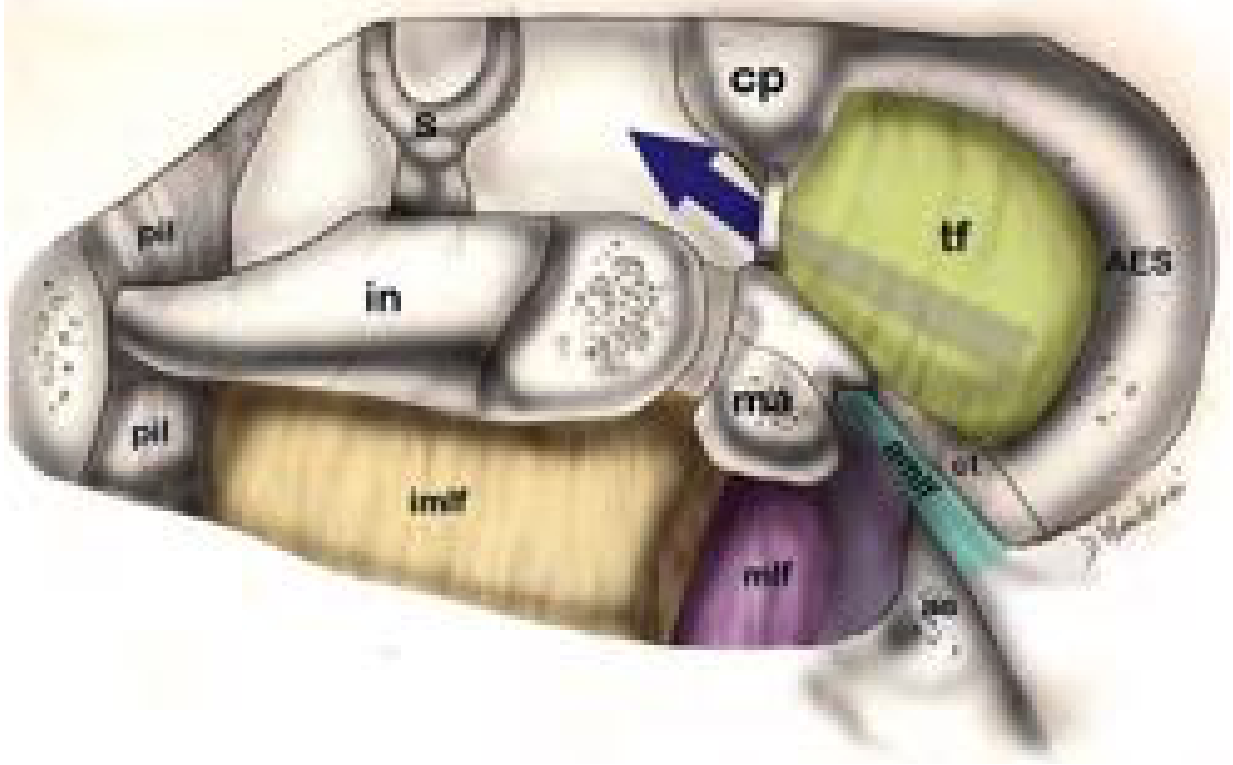
Fig. 144.3 - Schematic of the epitympanic diaphragm (right ear). Blue arrow = tympanic isthmus / aeration route. AES = anterior epitympanic space; tf = tensor fold; imlf = lateral incudomalleal fold; in = incus; s = stapes; cp = cochleariform process; pil = posterior incudal ligament; mlf = lateral malleal fold.
Pathway 1 - The Tympanic Isthmus (Primary Pathway)
This is the main route of middle ear aeration. The pathway:
- Starts at the Eustachian tube (protympanum / bony ET opening)
- Proceeds posteriorly through the mesotympanum, staying medial to the manubrium of the malleus and the long process of the incus
- Passes medial to the lateral incudomalleal fold
- Continues superiorly into the posterior epitympanum (superior lateral attic)
- From there communicates posteriorly via the aditus ad antrum into the mastoid antrum and mastoid air cell system
This channel - the tympanic isthmus - is the narrow bottleneck through which the vast majority of epitympanic and mastoid aeration occurs.
Pathway 2 - Anterior Epitympanic Space (via the Tensor Fold)
The anterior epitympanic space (AES) lies anterior to the cog and is ventilated via a separate route:
- When the tensor fold is absent or incomplete, air can pass from the supratubal recess directly into the anterior epitympanum - this is the "supratubal recess pathway."
- When the tensor fold is present and intact, it acts as a barrier, blocking direct ventilation of the anterior epitympanum from below. In this situation, the AES can only be aerated via a round-about route through the posterior epitympanum.
- Surgically, opening (incising) the tensor fold during chronic ear surgery provides an alternate ventilation route for the anterior epitympanum, which is exploited in procedures for cholesteatoma to prevent recurrence.
The cog (a bony septum from the tegmen, anterior to the malleus head) divides the epitympanum into anterior and posterior halves and influences how air flows between them.
Pathway 3 - Mastoid and Petrous Apex Air Cell Tracts
Beyond the aditus ad antrum, air reaches:
- Mastoid air cells - the largest pneumatized reservoir (normal combined middle ear + mastoid volume ~6 cc)
- Petrous apex air cells - via pneumatization tracts including the subcochlear canaliculi (passing inferior to the cochlea through the retrotympanum/hypotympanum)
- Peritubal cells and perilabyrinthine cells - smaller accessory tracts
Why Aeration Matters - Clinical Consequences
Failure of these pathways (e.g., Eustachian tube dysfunction, adhesive otitis, cholesteatoma blocking the tympanic isthmus) has direct acoustic consequences:
- Normal middle ear + mastoid volume: ~6 cc
- Volume <0.5 cc: progressive conductive hearing loss
- Non-aerated ears: 40-60 dB air-bone gap due to:
- Reduced ossicular coupling
- Restricted round window membrane movement (round window cannot move if middle ear is gas-free/fluid-filled, since cochlear fluids are incompressible)
- Negative middle ear pressure (ET dysfunction): disproportionate hearing loss at frequencies <1,000 Hz, with worse effect when middle ear pressure is negative relative to the ear canal
Summary Table
| Pathway | Route | Destination |
|---|---|---|
| Tympanic isthmus (primary) | ET → mesotympanum (medial to malleus/incus) → posterior epitympanum | Aditus → mastoid antrum → mastoid air cells |
| Supratubal recess | ET → supratubal recess → anterior epitympanum (when tensor fold absent/incomplete) | Anterior epitympanic space |
| Tensor fold opening (surgical/variant) | Mesotympanum → through/around tensor fold → anterior epitympanum | Anterior epitympanic space (AES) |
| Subcochlear canaliculi | Retrotympanum/hypotympanum → subcochlear tract | Petrous apex air cells |
Sources: Cummings Otolaryngology Head and Neck Surgery, Chapter 144 (Endoscopic Ear Surgery - Middle Ear Anatomy), p. 2756-2761; Shambaugh Surgery of the Ear, p. 89 (Aeration of the Middle Ear).
Spread of cholestetaoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile a thorough answer on the spread of cholesteatoma.
Spread of Cholesteatoma
Mechanism of Spread - Bone Erosion
Cholesteatoma spreads primarily through osteolytic bone erosion. The expanding keratinizing squamous epithelial sac erodes adjacent bone by two interacting mechanisms:
- Enzymatic osteolysis - The cholesteatoma matrix and perimatrix produce collagenases, metalloproteinases (MMPs), and other proteolytic enzymes that actively digest bone. Children's cholesteatomas show increased expression of these markers compared to adults, explaining the faster spread often seen in paediatric disease.
- Pressure necrosis - The accumulating keratin debris expands the sac, generating pressure against surrounding bony walls, leading to ischaemic necrosis of bone.
- Osteoclastic resorption - Osteoclast activation by cytokines (IL-1, TNF-α) released from the perimatrix further amplifies bone destruction.
Origin and Initial Spread
Pars Flaccida (Attic/Epitympanic) Cholesteatoma - Most Common (~80%)
Origin: Invagination of the pars flaccida into the Prussak's space (lateral epitympanic space between the neck of the malleus medially and the outer attic wall/scutum laterally).
Sequential spread:
Prussak's Space (lateral epitympanic space)
↓
Erosion of SCUTUM (earliest radiological sign)
↓
Medial displacement of ossicular chain
↓
Posterior epitympanum → Aditus ad antrum
↓
Mastoid antrum → Mastoid air cells
From here, spread can extend in multiple directions:
| Direction | Structure eroded | Consequence |
|---|---|---|
| Superiorly | Tegmen tympani / tegmen antri | Extradural abscess, meningitis, brain abscess |
| Posteriorly | Posterior fossa plate | Sigmoid sinus thrombophlebitis, cerebellar abscess |
| Medially/inferiorly | Ossicular chain | Conductive hearing loss |
| Medially | Lateral semicircular canal | Labyrinthine fistula → sensorineural/mixed hearing loss, vertigo |
| Medially | Cochlea | Profound SNHL |
| Laterally | Mastoid cortex | Post-auricular subperiosteal abscess |
| Inferiorly | Mastoid tip | Bezold's abscess (tracking along sternocleidomastoid) |
Pars Tensa Cholesteatoma - Less Common (~20%)
Origin: Retraction pocket from the pars tensa, typically from the posterosuperior quadrant.
Sequential spread:
Posterosuperior retraction pocket
↓
Medial to ossicular chain (posterior mesotympanum)
↓
Sinus tympani / posterior tympanic sinus / hypotympanum
↓
Round window niche → Cochlea (sensorineural loss)
↓
Retrotympanum → Petrous apex (via subcochlear canaliculi)
- Pars tensa cholesteatomas tend to lie medial to the ossicular chain from the outset, so they erode the long process of the incus and stapes superstructure early.
- They are more likely to invade the inner ear structures and round window, causing SNHL earlier than pars flaccida types.
Ossicular Erosion - Pattern and Frequency
Ossicular chain erosion is far more common with cholesteatoma than mucosal COM:
| Defect | With cholesteatoma (n=692) | Without cholesteatoma (n=519) |
|---|---|---|
| Ossicular chain intact | 27% | 71% |
| Incus alone eroded | 26% | 18% |
| Incus + stapes eroded, malleus intact | 24% | 7% |
| Incus, stapes + malleus eroded | 11% | 2% |
| Incus + malleus eroded, stapes intact | 8% | 2% |
The long process of the incus is the most commonly eroded ossicle because it is supplied by a single nutrient vessel and is most exposed to the expanding sac. A notable clinical paradox: hearing is often preserved even when the ossicular chain is largely destroyed, because the cholesteatoma sac itself bridges the acoustic gap between the tympanic membrane and the stapes/oval window. Surgical removal therefore paradoxically worsens hearing temporarily.
Spread to Critical Structures
Facial Nerve Canal
- Cholesteatoma erodes the horizontal (tympanic) segment of the facial canal most commonly (up to 19% of cases at surgery).
- Spread to the supratubal recess threatens the geniculate ganglion and first genu.
- CT detects dehiscence in only ~66-88% of cases; surgeons must always assume dehiscence.

Labyrinthine Fistula
- Occurs in 10-15% of cholesteatoma cases.
- The lateral semicircular canal is the most commonly affected (>90% of fistulas).
- Presents with vertigo, positive fistula test (pressure-induced nystagmus).
- CT sensitivity for fistula detection is unreliable (38-90% in reported series).
Intracranial Spread
Cholesteatoma may reach the intracranial compartment via:
- Tegmen tympani/antri erosion → extradural abscess, subdural empyema, meningitis
- Posterior fossa plate/sigmoid sinus plate erosion → sigmoid sinus thrombosis, cerebellar abscess
- Petrous apex via subcochlear canaliculi → petrous apicitis (Gradenigo's syndrome)
Petrous Apex
- Pars tensa cholesteatomas in the retrotympanum can track through the subcochlear canaliculi (inferior to the cochlea) into petrous apex air cells.
- Presents as Gradenigo's triad: otorrhoea + ipsilateral abducens palsy (CN VI) + retro-orbital pain (CN V).
Anterior Spread
- Into the supratubal recess and protympanum - threatens the geniculate ganglion of the facial nerve and the Eustachian tube orifice.
- May rarely extend anteriorly to the carotid canal.
Summary - Routes at a Glance
┌─ Tegmen → Intracranial (middle fossa)
│
Prussak's space ────┼─ Posterior epitympanum → Antrum → Mastoid
(attic chol.) │ ├─ Lateral SCC (fistula)
│ ├─ Facial canal (horizontal segment)
│ ├─ Mastoid cortex (subperiosteal abscess)
│ └─ Posterior fossa plate → Sigmoid sinus / cerebellum
│
└─ Inferior mastoid tip → Bezold's abscess
Posterosuperior
retraction pocket ──── Medial to ossicles → Sinus tympani
(pars tensa chol.) └─ Round window → Inner ear (SNHL)
└─ Retrotympanum → Petrous apex (Gradenigo)
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (Chapter 83 - Active Squamous COM; Chapter 85 - Ossicular Chain Defects); Cummings Otolaryngology Head and Neck Surgery (Chapter 144 - Endoscopic Ear Surgery); Scott-Brown's Vol. 2 (Chapter 97 - Imaging).
This is a shared conversation. Sign in to Orris to start your own chat.