What do you understand by zygosity and chorionicity of twin pregnancy?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive content from Creasy & Resnik's Maternal-Fetal Medicine. Let me compile the full answer.
Zygosity and Chorionicity in Twin Pregnancy
(Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice)
1. Zygosity
Zygosity refers to the type of conception - essentially, how the twins originated.
Dizygotic (DZ) Twins - "Fraternal"
- ~70% of all twins
- Result from polyovulation: two or more oocytes released in the same cycle, each fertilized by a separate sperm cell
- Share ~50% of genes - the same genetic relationship as non-twin siblings
- Can be same or different sex
- Incidence varies geographically: 6 per 1,000 births in Asia to 40 per 1,000 births in sub-Saharan Africa
- Influenced by maternal age, parity, BMI, height, smoking, and genetic predisposition (high FSH levels / polyovulation)
- Relevant genetic variants include GDF9, FSHB subunit, and SMAD3
Monozygotic (MZ) Twins - "Identical"
- ~30% of all twins
- Arise from division of a single zygote (one ovum + one sperm)
- Occur at a constant rate worldwide of ~3-4 per 1,000 births, largely independent of environmental factors
- ART (assisted reproductive technology) increases MZ twinning 2-5 fold - possibly due to micromanipulation, culture media composition, or embryo characteristics
- Although called "identical," MZ twins can show genotypic and phenotypic differences due to:
- Unequal blastomere allocation
- Postzygotic genetic events (nondisjunction, crossing over)
- Epigenetic differences
- X-inactivation differences
- Telomere length discordance
2. Chorionicity
Chorionicity refers to the type of placentation - specifically, whether twins share a chorion (outer placental membrane) or each has their own.
The Relationship Between Zygosity and Chorionicity
The two are closely linked but not perfectly equivalent:
| Zygosity | Typical Chorionicity |
|---|---|
| Dizygotic | Dichorionic-Diamniotic (DCDA) - almost always |
| Monozygotic (early split, <3 days) | Dichorionic-Diamniotic (70% of MZ) |
| Monozygotic (split 3-9 days) | Monochorionic-Diamniotic (25% of MZ) |
| Monozygotic (split 8-12 days) | Monochorionic-Monoamniotic (2% of MZ) |
| Monozygotic (split 13-16 days) | Conjoined twins (1:100,000) |
The traditional fission (splitting) model holds that the timing of zygote division determines placentation type. An alternative fusion model proposes that MZ twinning occurs at the first cleavage division, with chorionicity determined by subsequent fusion of embryonic membranes - both models remain unproven.
Types of Placentation
Dichorionic placenta:
- Each twin has its own chorion, amnion, and fetoplacental circulation
- The two placentas may be separate (distant implantation) or fused as a single placental mass (close implantation) - though circulations remain separate
- Intertwin membrane: thick, 4-layered (2 amnion + 2 chorion layers)
Monochorionic placenta:
- Single chorion shared by both twins
- Nearly always contains intertwin vascular anastomoses (>95%):
- Artery-to-artery (AA) - superficial, bidirectional
- Vein-to-vein (VV) - superficial, bidirectional
- Artery-to-vein (AV) - deep, obligatorily unidirectional
- The presence of these anastomoses underlies complications unique to monochorionic twins
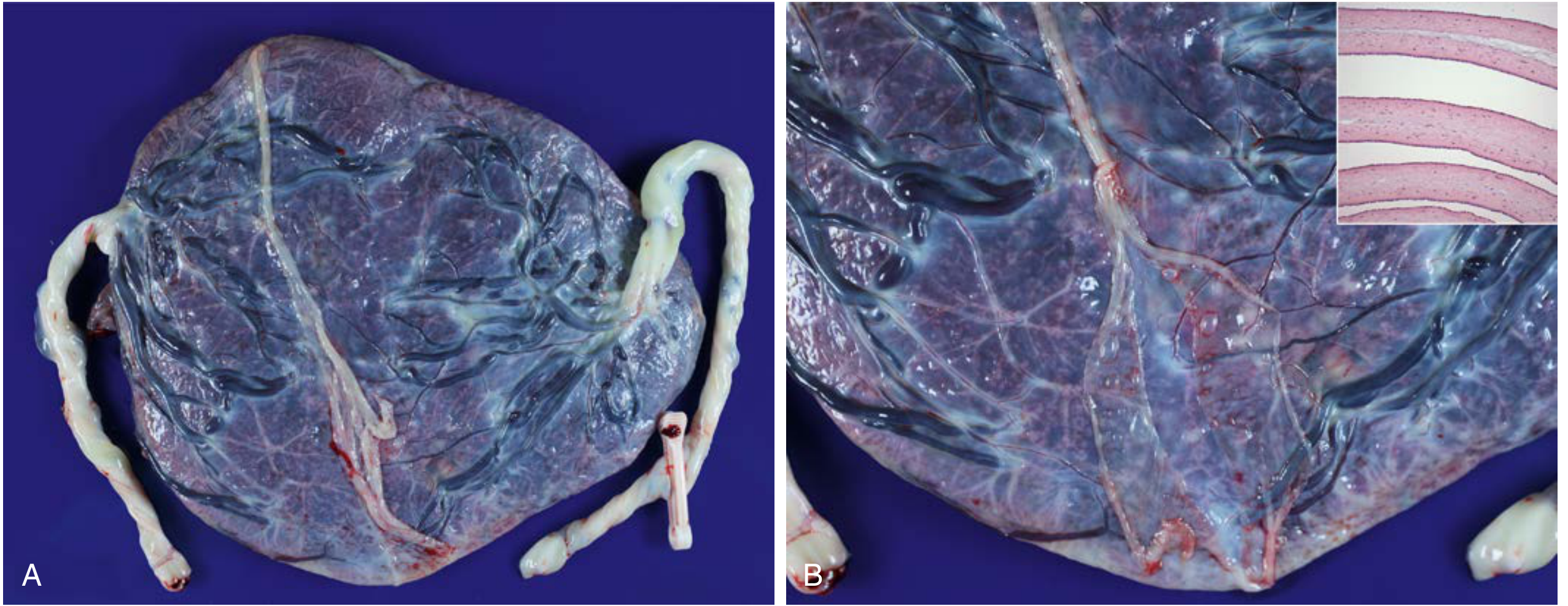
Fig. 5.3 - Diamniotic-monochorionic twin placenta. Note the thin, semitranslucent intertwin membrane, with chorionic vessels crossing it. Histological inset (top right) shows two amnion layers with no interposed chorion.
3. Antenatal Determination of Chorionicity
Chorionicity should be determined as early as possible, ideally at 10-14 weeks' gestation by ultrasound.
First trimester (<8 weeks):
- Separate gestational sacs with thick echogenic rings → dichorionicity
- No separate rings visible → likely monochorionicity
- Number of yolk sacs helps determine amnionicity (2 yolk sacs = diamniotic; 1 yolk sac = likely monoamniotic)
Key ultrasound markers:
| Sign | Indicates |
|---|---|
| Discordant fetal sex | Dichorionic (with near certainty) |
| Two clearly distinct placental sites | Dichorionic |
| Lambda (twin-peak) sign - triangular wedge of placenta projecting between membrane layers | Dichorionic |
| T-sign - thin membrane inserting perpendicularly to placenta | Monochorionic |
| Thick dividing membrane (≥2 mm; 4 layers) | Dichorionic |
| Thin 2-layered membrane | Monochorionic |
A composite approach (single placenta + sex concordance + thin membrane + absent twin-peak sign) yields a positive predictive value for monochorionicity of 92%.
First-trimester transvaginal sonography with this composite approach achieves near-100% accuracy. Sensitivity for monochorionicity is ~90% in both trimesters; specificity falls from 99% (first trimester) to 95% (second trimester).

Fig. 37.1 - Dichorionic twin gestation confirmed by discordant fetal sex (XX on left, XY on right).
4. Postnatal Confirmation
Postnatally, chorionicity is confirmed by placental pathology:
- Monochorionic placenta: thin, 2-layered (amnion only) intertwin membrane, chorionic vessels crossing the membrane
- Dichorionic placenta: thick, 4-layered membrane; no anastomoses
5. Why This Matters Clinically
Chorionicity drives obstetric risk:
- Monochorionic twins carry significantly higher perinatal mortality and face unique complications:
- Twin-twin transfusion syndrome (TTTS) - at least 15% of MC twins
- Twin anemia-polycythemia sequence (TAPS)
- Fetal growth discordance
- Congenital malformations (higher rate)
- Risk of cord entanglement (monoamniotic)
Zygosity matters for long-term health:
- Organ transplantation planning (MZ twins are immunologically compatible)
- Inheritance risk counseling for genetic diseases
- Definitive zygosity determination requires genetic testing - blood group typing (discordant groups = dizygotic) or, preferably, DNA studies (skin biopsy, umbilical cord tissue, or buccal smear)
Important caveat: The classical rule "monochorionic = monozygotic" is not absolute. Rare dizygotic monochorionic twins exist (>20 documented cases), usually in ART pregnancies and often associated with chimerism. Therefore, monochorionic placentation is a screening indicator - not unequivocal proof - of monozygosity.
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapters on Twinning, Chorionicity, Monochorionic Placentation, and Multiple Gestation
This is a shared conversation. Sign in to Orris to start your own chat.