Explain me 10 common heart disease and with ecg changes with ecg images those diseases
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Searching Images
atrial fibrillation ECG electrocardiogram
Finding Sources
Searching Images
heart block complete AV block ECG third degree
Searching Images
ventricular tachycardia ECG wide complex
Searching Images
left bundle branch block ECG LBBB
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG WPW
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
long QT syndrome Torsades de Pointes ECG
Here is a comprehensive guide to 10 common heart diseases with their ECG changes and real ECG images:
10 Common Heart Diseases: ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery → transmural ischemia → necrosis.
ECG Changes:
| Phase | Changes |
|---|---|
| Hyperacute (minutes) | Peaked, tall "hyperacute" T-waves |
| Acute (hours) | Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous leads |
| Evolving | Q-wave formation, T-wave inversion |
| Old/Chronic | Pathological Q-waves, T-wave normalization |
- Anterior STEMI (LAD): ST elevation in V1–V6, reciprocal depression in II, III, aVF
- Inferior STEMI (RCA/LCx): ST elevation in II, III, aVF; reciprocal depression in I, aVL
- Lateral STEMI: ST elevation in I, aVL, V5–V6
- Posterior STEMI: Tall R wave + ST depression in V1–V3 (mirror image)
ECG Image — Acute Anterolateral STEMI (LAD occlusion):

ECG Image — Acute Inferior + Posterior STEMI (RCA/LCx):
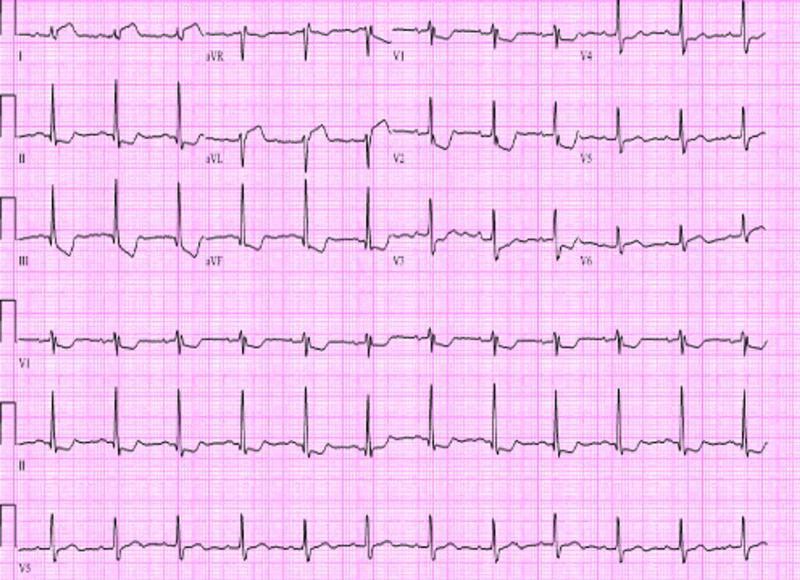
2. 💓 Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity from multiple re-entrant circuits → loss of organized atrial contraction.
ECG Changes:
- Absent P waves — replaced by irregular fibrillatory (f) waves, best seen in V1 and lead II
- Irregularly irregular R-R intervals — hallmark finding
- Narrow QRS (unless aberrant conduction/WPW)
- Ventricular rate 100–180 bpm if uncontrolled (tachycardic AF) or <100 bpm if rate-controlled
- No consistent PR interval
ECG Image — Atrial Fibrillation with Rapid Ventricular Response:

3. 🔴 Complete (Third-Degree) AV Heart Block
Pathophysiology: Total failure of impulse conduction from atria to ventricles through the AV node → complete AV dissociation. Requires pacemaker.
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes fire independently
- P waves: Regular at faster atrial rate (e.g., 70–80 bpm)
- QRS complexes: Slow escape rhythm (20–50 bpm)
- Wide QRS (>120 ms) if ventricular escape focus; narrow if junctional escape
- Fixed, slow ventricular rate — bradycardia
- P waves "march through" QRS complexes and T-waves
ECG Image — Complete (Third-Degree) AV Block:

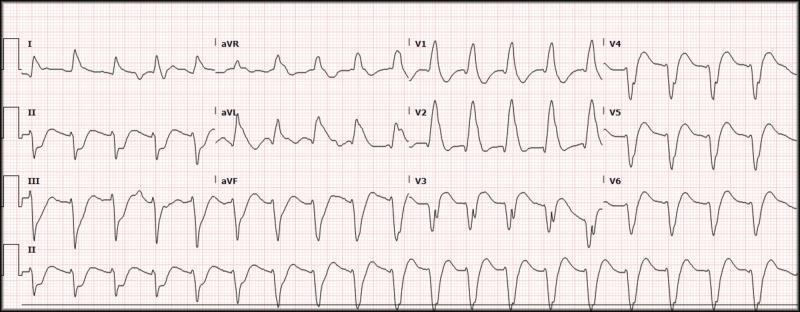
4. ⚡ Ventricular Tachycardia (VT)
Pathophysiology: Rapid ventricular depolarization from an ectopic ventricular focus, often in the setting of structural heart disease (post-MI scar, cardiomyopathy).
ECG Changes:
- Wide QRS tachycardia (QRS ≥120 ms) at rate >100 bpm (usually 150–250 bpm)
- AV dissociation — P waves independent of QRS (diagnostic if seen)
- Fusion beats and capture beats — pathognomonic when present
- Positive or negative concordance across precordial leads
- Brugada criteria / Vereckei algorithm used to differentiate from SVT with aberrancy
- Regular, monomorphic rhythm (monomorphic VT) or twisting morphology (polymorphic VT / Torsades)
ECG Image — Monomorphic Ventricular Tachycardia:

Note: If image above doesn't render, see below alternate:
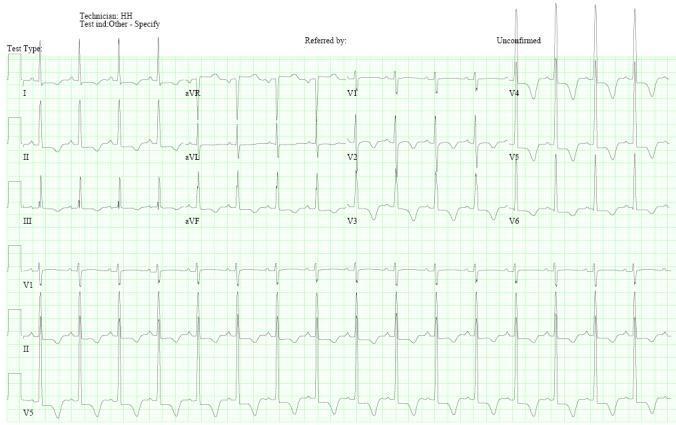
5. 🌊 Left Bundle Branch Block (LBBB)
Pathophysiology: Failure of conduction through the left bundle branch → right-to-left ventricular depolarization → widened QRS with characteristic morphology. Associated with cardiomyopathy, CAD, hypertension.
ECG Changes (William Morrow mnemonic: WiLLiaM):
- QRS ≥120 ms (broad)
- Lead V1: Deep, broad S-wave (QS or rS pattern) — negative deflection
- Lead V6/I/aVL: Broad, monophasic R-wave (often notched/slurred "M" shape)
- No septal Q waves in V5–V6 (loss of septal activation)
- Discordant ST-T changes — ST/T opposite to QRS direction (secondary changes)
- New LBBB in acute chest pain = treat as STEMI equivalent (Sgarbossa criteria)
ECG Image — Left Bundle Branch Block:
6. ✨ Wolff-Parkinson-White Syndrome (WPW)
Pathophysiology: Accessory conduction pathway (Bundle of Kent) bypasses the AV node → ventricular pre-excitation. Risk of sudden death if AF conducts rapidly via accessory pathway.
ECG Changes (Classic Triad):
| Feature | Finding |
|---|---|
| Short PR interval | <120 ms (bypasses AV node delay) |
| Delta wave | Slurred upstroke at beginning of QRS |
| Wide QRS | >120 ms (fusion of normal + pre-excitation) |
- Secondary ST-T changes (discordant to delta wave direction)
- Pseudo-infarct patterns (negative delta waves can mimic Q waves)
- Pathway localization by delta wave polarity across leads
- Paroxysmal SVT / AVRT common clinical presentation
ECG Image — Wolff-Parkinson-White Syndrome (Classic Delta Waves):

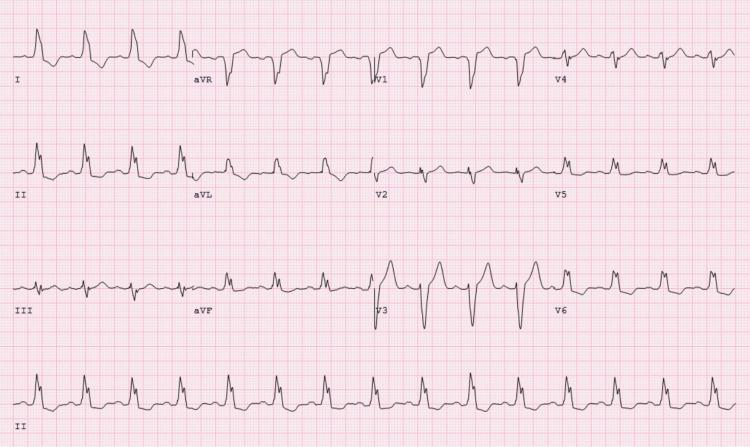
7. 💪 Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Sarcomere gene mutations → asymmetric septal hypertrophy → LV outflow obstruction, diastolic dysfunction, myofiber disarray → risk of sudden cardiac death (especially in young athletes).
ECG Changes:
- Left ventricular hypertrophy (LVH) — high voltage QRS (Sokolow-Lyon: S V1 + R V5/V6 ≥35 mm)
- Deep "giant" T-wave inversions — especially V2–V5 in apical HCM (Yamaguchi syndrome); deep symmetric
- Strain pattern — ST depression + T inversion in lateral leads (I, aVL, V5–V6)
- Absent septal Q waves in lateral leads (due to septal hypertrophy reversing normal septal activation)
- Left axis deviation
- Wide QRS if significant hypertrophy with conduction delay
- Abnormal ECG found in >95% of HCM patients
ECG Image — HCM with Giant T-wave Inversions (Apical Variant):
ECG Image — HCM comparison (Concentric vs Septal vs Apical):
8. 🔥 Acute Pericarditis
Pathophysiology: Inflammation of the pericardium → epicardial injury currents → diffuse ST changes (unlike STEMI which is territorial). Causes: viral (most common), autoimmune, post-MI (Dressler's), uremia.
ECG Changes (4 Classic Stages):
| Stage | Timing | ECG Findings |
|---|---|---|
| Stage 1 | Days 1–2 | Diffuse concave ("saddle-shaped") ST elevation in all leads except aVR + V1; PR depression |
| Stage 2 | Week 1 | ST normalizes, PR depression persists |
| Stage 3 | Week 2 | Diffuse T-wave inversion |
| Stage 4 | Weeks–months | ECG normalizes |
Key differentiating features from STEMI:
- Diffuse (not territorial) ST elevation
- PR segment depression (most specific sign) — best in II, most leads; aVR shows reciprocal PR elevation
- Spodick's sign — downsloping TP segment
- No reciprocal ST depression (except in aVR/V1)
- No Q-waves
ECG Image — Acute Pericarditis (Saddle-shaped ST elevation + PR depression):

9. 🫁 Pulmonary Embolism (PE)
Pathophysiology: Thrombus in pulmonary vasculature → acute right ventricular pressure overload → RV strain → specific ECG pattern. Most common ECG finding is simply sinus tachycardia.
ECG Changes:
| Finding | Significance |
|---|---|
| Sinus tachycardia | Most common finding (70%) |
| S1Q3T3 pattern | S wave in I + Q wave in III + T inversion in III — classic but only 20% sensitive |
| Right axis deviation | RV strain |
| RBBB (complete or incomplete) | Acute RV dilation stretches right bundle |
| T-wave inversions V1–V4 | Anterior RV strain pattern |
| P pulmonale | Peaked P waves — right atrial enlargement |
| AF / atrial flutter | Occasionally seen |
ECG Image — Pulmonary Embolism (S1Q3T3 pattern):

ECG Image — PE with RBBB + S1Q3T3:

10. ⏱️ Long QT Syndrome (LQTS) / Torsades de Pointes
Pathophysiology: Prolonged ventricular repolarization (genetic channelopathies — KCNQ1, KCNH2, SCN5A; or acquired via drugs, electrolytes) → increased dispersion of refractoriness → risk of Torsades de Pointes (TdP) → VF → sudden cardiac death.
ECG Changes:
| Feature | Details |
|---|---|
| Prolonged QTc | >440 ms (men) / >460 ms (women); critical risk >500 ms |
| T-wave abnormalities | Broad-based, notched, or biphasic T-waves (subtype-specific morphology) |
| U waves | Prominent U waves (LQT2) — can fuse with T-wave |
| T-wave alternans | Beat-to-beat variation in T-wave amplitude/polarity — sign of electrical instability |
| Torsades de Pointes | Polymorphic VT with "twisting" QRS complexes around isoelectric line, initiated by short-long-short sequence |
- LQT1: Broad smooth T-wave
- LQT2: Notched/bifid T-wave, prominent U-waves
- LQT3: Late-appearing, narrow T-wave with long isoelectric ST segment
ECG Image — Long QT Syndrome → Torsades de Pointes:
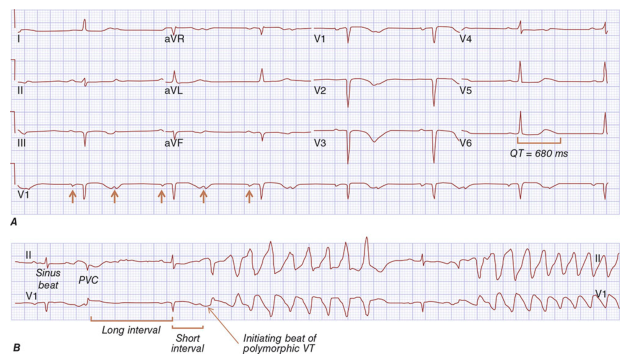
ECG Image — Torsades de Pointes initiation:

Quick Reference Summary Table
| # | Disease | Key ECG Feature |
|---|---|---|
| 1 | STEMI | Convex ST elevation (territorial) + reciprocal changes + Q waves |
| 2 | Atrial Fibrillation | Absent P waves + irregularly irregular rhythm |
| 3 | Complete AV Block | AV dissociation — P waves ≠ QRS, slow escape rhythm |
| 4 | Ventricular Tachycardia | Wide QRS tachycardia + AV dissociation |
| 5 | LBBB | Wide QRS + deep S in V1 + broad R in V6, discordant ST-T |
| 6 | WPW Syndrome | Short PR + delta wave + wide QRS (pre-excitation triad) |
| 7 | Hypertrophic CM | LVH + giant T inversions + absent lateral Q waves |
| 8 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| 9 | Pulmonary Embolism | Sinus tachycardia + S1Q3T3 + RV strain pattern |
| 10 | Long QT / TdP | Prolonged QTc + T-wave abnormalities → Torsades de Pointes |
Clinical Pearl: The ECG is always interpreted in clinical context. A single finding rarely makes a diagnosis — combine rhythm, morphology, intervals, and lead distribution with the patient's presentation for accurate interpretation.
ECG images sourced from peer-reviewed clinical literature (PMC) and Harrison's Principles of Internal Medicine, 21st Edition.
This is a shared conversation. Sign in to Orris to start your own chat.