Sciatic nerve short note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information to write a thorough short note on the sciatic nerve. Let me compile everything.
Sciatic Nerve - Short Note
Overview
The sciatic nerve is the largest nerve in the body. It is a branch of the lumbosacral plexus, formed from the anterior rami of spinal cord segments L4, L5, S1, S2, and S3. It is structurally composed of two distinct nerves - the tibial nerve (anterior divisions of L4-S3) and the common fibular (peroneal) nerve (posterior divisions of L4-S2) - sharing a common epineural sheath from the pelvis to the popliteal fossa.
(Gray's Anatomy for Students, p. 668)
Course
1. In the Pelvis
The sciatic nerve is formed from the sacral plexus on the posterior pelvic wall and exits the pelvis through the greater sciatic foramen, inferior to the piriformis muscle.
Variant: Occasionally, the common fibular division (or the entire nerve) passes through or above the piriformis muscle - clinically relevant in piriformis syndrome.
2. In the Gluteal Region
- Passes deep to the gluteus maximus
- Descends in the plane between the superficial and deep muscle groups, crossing the posterior surfaces of the obturator internus, gemelli, and quadratus femoris
- Lies at the midpoint between the ischial tuberosity and the greater trochanter (the classic intramuscular injection landmark to avoid)
3. In the Posterior Thigh
- Lies on the adductor magnus, crossed by the long head of biceps femoris
- Gives off branches to all posterior thigh muscles before dividing
4. Division
The sciatic nerve divides into its two terminal branches proximal to the knee (upper popliteal fossa, or sometimes within the pelvis itself):
- Tibial nerve - descends vertically through the popliteal fossa
- Common fibular (peroneal) nerve - winds around the neck of the fibula
(Gray's Anatomy for Students, pp. 668, 682, 688)
Cross-sectional anatomy (Imaging Anatomy Atlas)
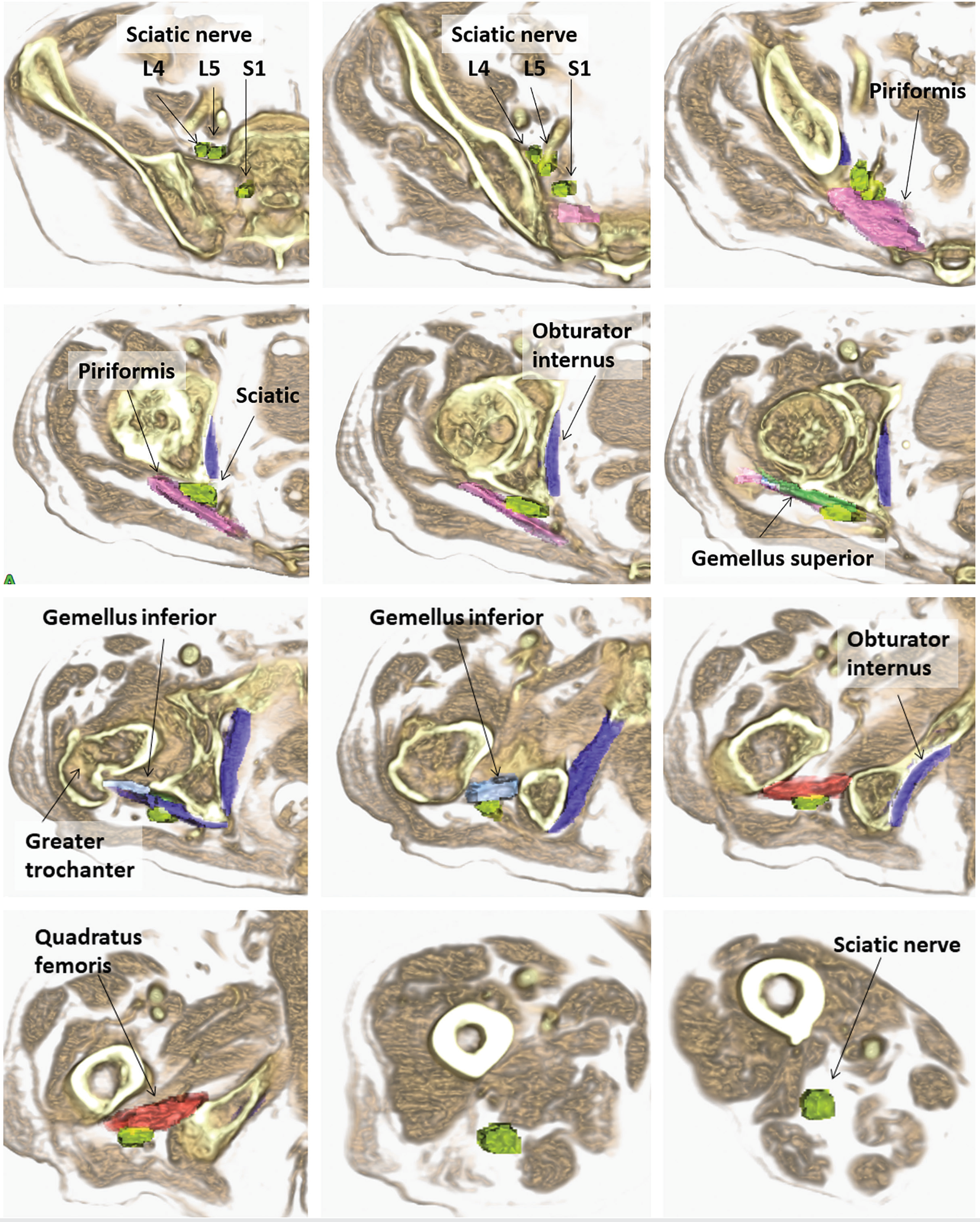
Serial cross-sections showing the sciatic nerve (green) as it descends from the sciatic notch (with L4, L5, S1 roots) through the gluteal region past the piriformis, obturator internus, gemelli, quadratus femoris, and into the posterior thigh.
Motor Supply
| Region | Muscles Supplied | Division |
|---|---|---|
| Posterior thigh (hamstrings) | Biceps femoris (long head), semitendinosus, semimembranosus | Tibial division |
| Posterior thigh | Biceps femoris (short head) | Common fibular division |
| Ischial part of adductor magnus | Adductor magnus (hamstring part) | Tibial division |
| All leg muscles | Anterior, posterior, lateral compartments | Via tibial and common fibular branches |
| All foot muscles | Intrinsic foot muscles | Via plantar nerves (tibial) |
(Gray's Anatomy for Students, p. 668; Bradley's Neurology in Clinical Practice)
Sensory Supply
- Lateral side of the leg
- Lateral side and entire sole of the foot
- Whole of the foot (except medial leg/foot supplied by the saphenous nerve)
Applied Anatomy / Clinical Importance
1. Intramuscular Injection
- Misplaced injections into the buttock (especially in thin/elderly patients with reduced gluteal muscle mass) can injure the sciatic nerve
- Safe injection site: upper outer quadrant of the gluteal region
- (Andrews' Diseases of the Skin)
2. Complete Sciatic Nerve Lesion
Causes:
- Weakness of knee flexors (hamstrings)
- Complete paralysis of all muscles below the knee
- Sensory loss over the entire foot and leg below the knee (except medial leg - saphenous nerve territory)
- Loss of ankle jerk and plantar reflexes
3. Partial Sciatic Nerve Lesion (Common Pattern)
The common fibular division is more commonly injured than the tibial division in proximal lesions because:
- Fewer fascicles with less supportive connective tissue
- More taut and secured at the sciatic notch and fibular neck
This can mimic a distal common fibular neuropathy. EMG evidence of denervation in the short head of biceps femoris (innervated by the fibular division of the sciatic nerve) localizes the lesion proximal to the knee, distinguishing sciatic nerve injury from common fibular nerve injury at the fibular head.
(Bradley and Daroff's Neurology in Clinical Practice)
4. Causes of Sciatic Nerve Injury
- Hip surgery - most common cause (hip replacement)
- Posterior dislocation of the hip
- Subtrochanteric femur fracture
- Bullet/stab wounds
- Hematoma in the posterior thigh
- Prolonged sitting on hard surface ("toilet seat palsy")
- Baker cyst compression in popliteal fossa
- Endometriosis involving the nerve (causes recurrent sciatic mononeuropathy)
5. Piriformis Syndrome
A controversial entrapment syndrome where the piriformis muscle compresses the sciatic nerve. Classic features:
- History of buttock trauma
- Pain maximal during prolonged sitting (driving, biking)
- Pain reproduced by hip adduction, internal rotation, and flexion (AIF maneuver)
- Usually normal neurological and nerve conduction studies
- MRI may show hypertrophied piriformis
(Bradley and Daroff's Neurology, p. 2531-2533)
6. Terminal Branch Injuries
| Nerve | Injury site | Deformity | Motor loss | Sensory loss |
|---|---|---|---|---|
| Common fibular | Neck of fibula | Foot drop + talipes equinovarus | Dorsiflexors, evertors | Anterior/lateral leg, dorsum of foot |
| Tibial | Popliteal fossa / posterior leg | Talipes calcaneovalgus + claw foot | Plantar flexors, intrinsic foot muscles | Entire sole |
(S Das Manual on Clinical Surgery, 13th Ed, pp. 135-146)
Summary Table
| Feature | Detail |
|---|---|
| Root value | L4, L5, S1, S2, S3 |
| Type | Mixed (motor + sensory) |
| Size | Largest nerve in the body |
| Exit from pelvis | Greater sciatic foramen, below piriformis |
| Division point | Upper popliteal fossa (or sometimes in pelvis) |
| Terminal branches | Tibial nerve + Common fibular nerve |
| Key landmark | Midpoint of ischial tuberosity to greater trochanter |
| Key clinical test | Straight leg raise (SLR) for sciatic stretch |
Sources: Gray's Anatomy for Students (4th Ed) | Bradley and Daroff's Neurology in Clinical Practice | S Das Manual on Clinical Surgery (13th Ed) | Imaging Anatomy: Bones, Joints, Vessels and Nerves
Branches
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed. Here is the comprehensive short note on branches of the sciatic nerve:
Branches of the Sciatic Nerve
The sciatic nerve gives branches at three levels: in the thigh (before dividing), then via its two terminal divisions.
A. Branches in the Thigh (Before Division)
These arise from the tibial part of the sciatic nerve while it still shares a common sheath:
| Muscle | Division supplying it |
|---|---|
| Semitendinosus | Tibial |
| Semimembranosus | Tibial |
| Biceps femoris - long head | Tibial |
| Adductor magnus (ischial/hamstring part) | Tibial |
| Biceps femoris - short head | Common fibular |
The short head of biceps femoris is the only posterior thigh muscle supplied by the common fibular division - this is the key EMG landmark for localizing proximal sciatic lesions.
(Gray's Anatomy for Students, p. 688; Bradley & Daroff's Neurology, p. 2523)
B. Terminal Divisions
The sciatic nerve divides in the upper popliteal fossa (or sometimes within the pelvis) into:
- Tibial nerve (L4-S3, anterior divisions)
- Common fibular (peroneal) nerve (L4-S2, posterior divisions)
I. TIBIAL NERVE
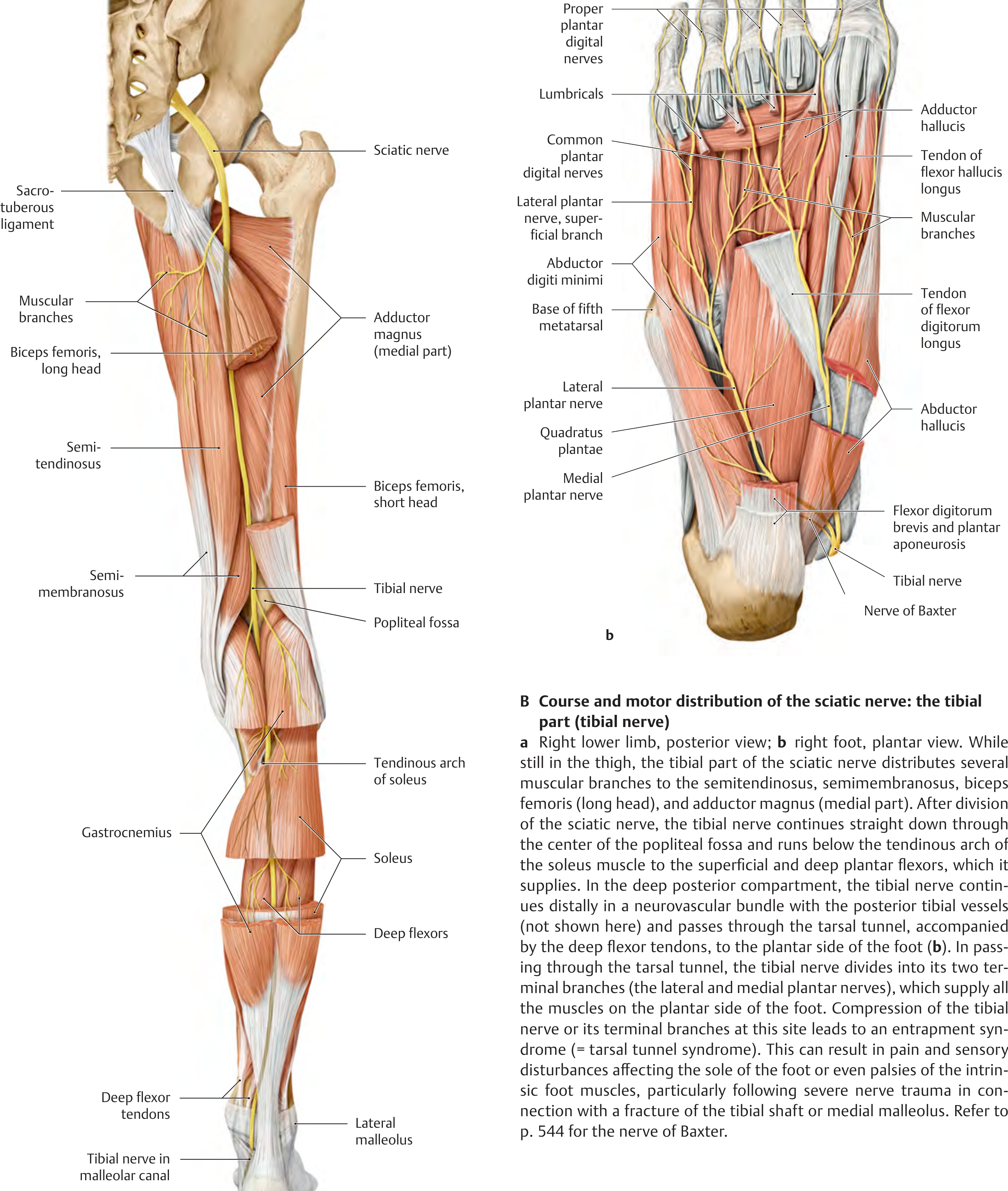
1. In the Popliteal Fossa
- Muscular branches to superficial posterior leg muscles:
- Gastrocnemius (both heads)
- Plantaris
- Soleus
- Popliteus
- Sural nerve (cutaneous) - arises high between the two heads of gastrocnemius, descends superficially, is joined by the sural communicating branch of the common fibular nerve, then supplies skin of the lower posterolateral leg, lateral ankle, lateral foot, and little toe
2. In the Posterior Leg (Deep to Soleus)
- Muscular branches to deep posterior compartment:
- Tibialis posterior
- Flexor digitorum longus
- Flexor hallucis longus
- Medial calcaneal nerve - pierces the flexor retinaculum to supply skin of the heel
3. In the Foot (via Tarsal Tunnel, Behind Medial Malleolus)
The tibial nerve passes through the tarsal tunnel and divides midway between the medial malleolus and heel into two terminal branches:
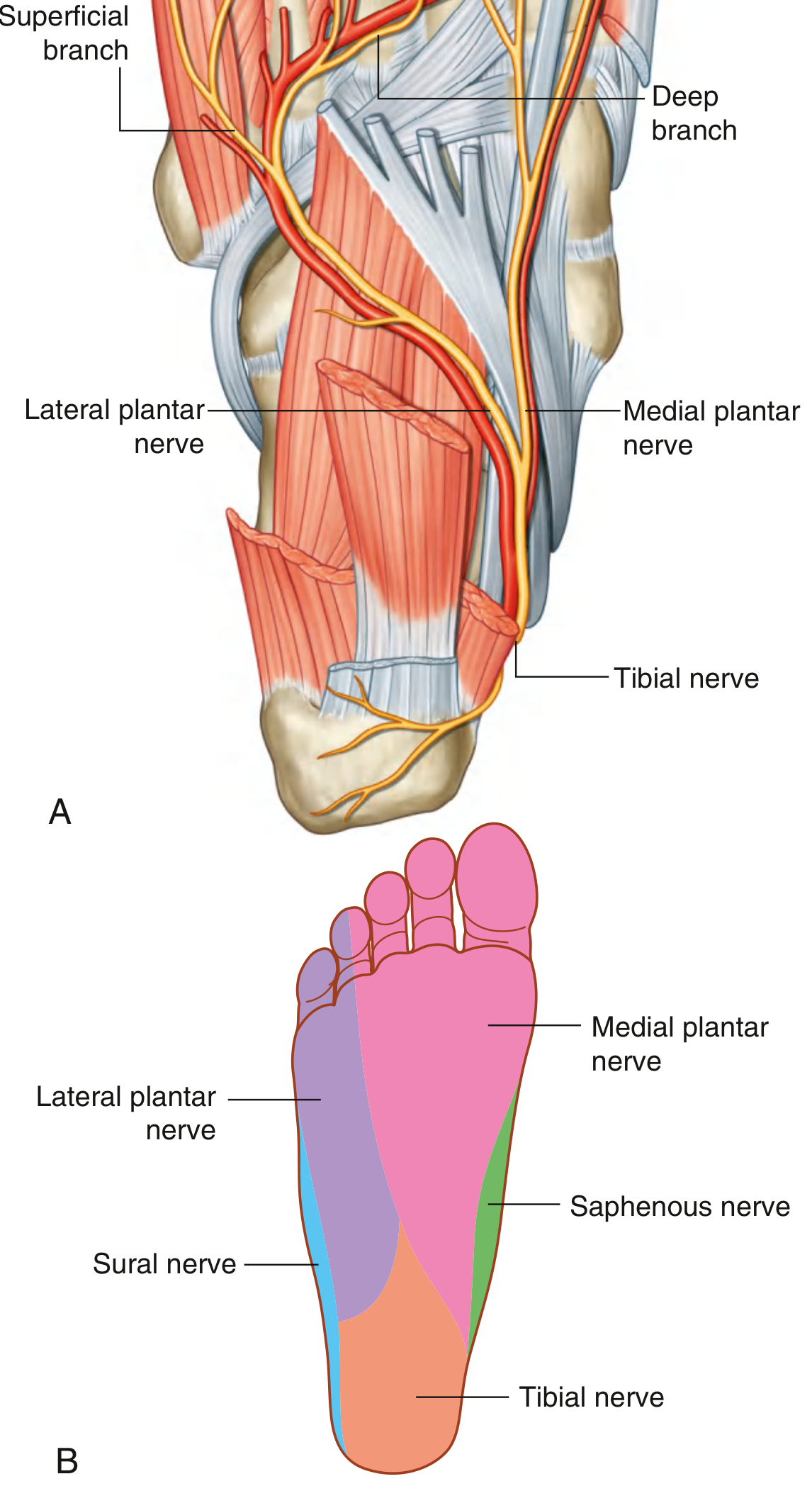
a) Medial Plantar Nerve (larger - analogous to median nerve in hand)
- Motor: Abductor hallucis, flexor digitorum brevis, flexor hallucis brevis, 1st lumbrical
- Sensory: Medial two-thirds of the sole + plantar surfaces of medial 3½ toes (including great toe)
b) Lateral Plantar Nerve (smaller - analogous to ulnar nerve in hand)
- Motor: All remaining intrinsic foot muscles - quadratus plantae, abductor digiti minimi, flexor digiti minimi, lumbricals 2-4, all interossei, adductor hallucis
- Sensory: Lateral one-third of sole + plantar surfaces of lateral 1½ toes
- Divides into deep branch (motor to interossei) and superficial branch (digital nerves to little toe)
(Gray's Anatomy for Students, pp. 732, 767)
II. COMMON FIBULAR (PERONEAL) NERVE
Winds around the neck of the fibula, passes through the origin of fibularis longus ("fibular tunnel"), then divides into two terminal branches.
Branches Before Division (at fibular neck)
- Lateral cutaneous nerve of the calf - skin over upper third of lateral leg
- Fibular (peroneal) communicating nerve - joins the sural nerve
Terminal Branches
a) Deep Fibular (Anterior Tibial) Nerve
- Pierces the anterior intermuscular septum into the anterior compartment
- Motor: Tibialis anterior, extensor hallucis longus, extensor digitorum longus, fibularis (peroneus) tertius, extensor digitorum brevis (on dorsum of foot)
- Sensory: First web space between great toe and 2nd toe only (very small area)
- Runs with the anterior tibial vessels on the interosseous membrane
b) Superficial Fibular (Musculocutaneous) Nerve
- Remains in the lateral compartment
- Motor: Fibularis (peroneus) longus and brevis
- Sensory: Lower two-thirds of lateral leg + entire dorsum of foot and toes (except 1st web space and lateral border supplied by sural nerve)
Accessory deep fibular nerve: present in up to 28% of individuals - arises from the superficial fibular nerve, passes behind the lateral malleolus to supply the lateral part of extensor digitorum brevis.
(Bradley & Daroff's Neurology, p. 2547; THIEME General Anatomy & Musculoskeletal System)
Summary Tree
SCIATIC NERVE (L4-S3)
│
├── Muscular branches in thigh (tibial division)
│ ├── Semitendinosus
│ ├── Semimembranosus
│ ├── Biceps femoris (long head)
│ └── Adductor magnus (ischial part)
├── Short head of biceps femoris (fibular division)
│
├── TIBIAL NERVE
│ ├── Popliteal fossa: gastrocnemius, plantaris, soleus, popliteus
│ ├── Sural nerve (cutaneous - lateral leg & foot)
│ ├── Leg: tibialis posterior, FDL, FHL
│ ├── Medial calcaneal nerve (heel skin)
│ └── Tarsal tunnel → Medial plantar nerve + Lateral plantar nerve
│
└── COMMON FIBULAR NERVE
├── Lateral cutaneous nerve of calf
├── Fibular communicating nerve (→ sural)
├── Deep fibular nerve (anterior compartment + 1st web space)
└── Superficial fibular nerve (lateral compartment + dorsum of foot)
Sources: Gray's Anatomy for Students (4th Ed) | Bradley and Daroff's Neurology in Clinical Practice | THIEME Atlas of Anatomy: General Anatomy & Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.