Hi orris , I am Mayur Lokhande 23 yr old male , currently studying at pune in final year MBBS , native place Nagpur, i have a chief complaints of profuse hair fall since 1-1.5 months , which was started 2 years back , and I showed it to doctors , they prescribed me investigation like serum levels of all vit and minerals which came normal , prescribed me Root gain hair serum to use topically and keraglow tab to take once a day daily , and adviced me PRP but it was costly for me, so i decided to continue with serum and tablets,they dx me as Androgen male pattern hair baldness, I have a family history of baldness from grandfather old ancestry . The hair fall stopped after that , everything was normal but then started having practice of vollyball which i play daily in red soil , so have to take bath twice a days , then before 1 month i started to have a hairfall again which was more produce from parito- occipital and parito - temporal juction, which led to bald patch on perito- occipital area , i think like 4a type , so again visited clinician they added minoxidil 5% in routine, now i shaved my hair again for better application of minoxidil+ fenestride 5% , i have no idea what shampoo to use as i wash my hair daily, and root gain serum is too expensive so i stopped it now , insted having hairline -F product containing 5% minoxidil + fenestride, so tell me about everything that is happening with me , what should I do now to recover fully , and give me routine like a best and suggestion of products to use for my healthy scalp , like whoch shampoo to use whoch oil to use when to apply this hairline F what to do with other things like hell of a routine, and also i have been mastrubating a lot so tell me about that how to overcome and how it effect overall health and hairfall, tell me one snap solution for it , simple , easily understandable medical language, and stepwise and detailed fashion
minoxidil finasteride combination hair loss routine shampoo oil daily use 2024 2025
masturbation DHT testosterone hair loss scientific evidence myth 2024
best shampoo for androgenetic alopecia minoxidil users ketoconazole caffeine rosemary 2025
Your Complete Hair Loss Guide - Mayur Lokhande, 23M, AGA
PART 1: WHAT IS HAPPENING TO YOU - THE FULL PICTURE
Understanding Your Diagnosis: Androgenetic Alopecia (AGA)
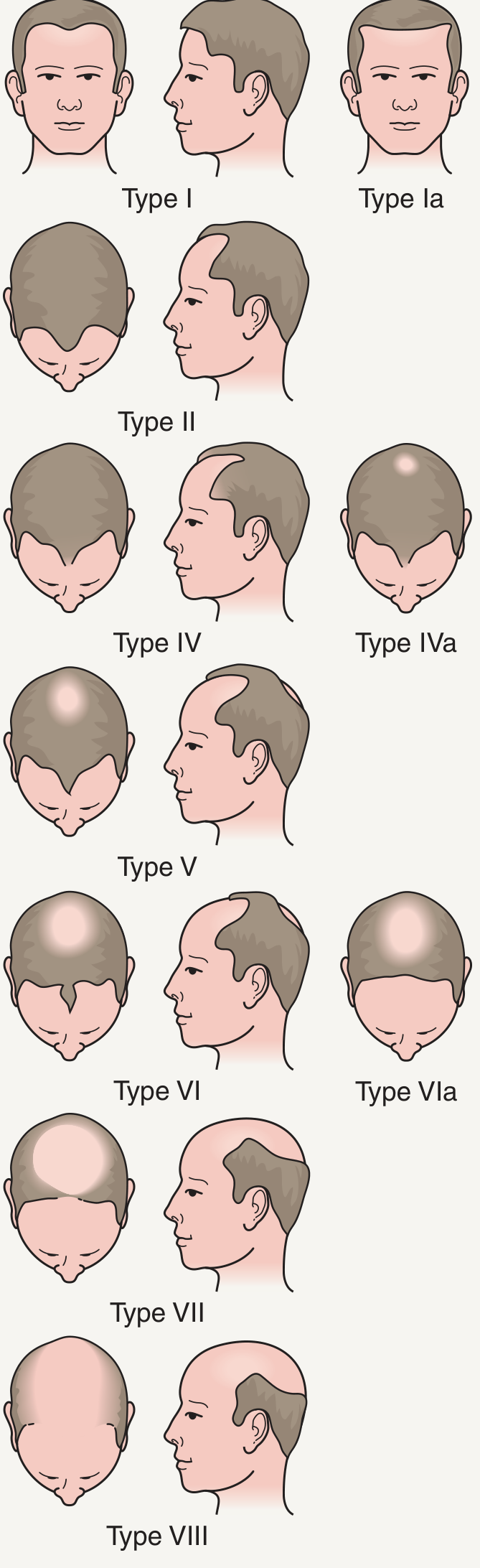
Why Did the Hair Fall Re-Start 1 Month Ago?
PART 2: YOUR MEDICINES - WHAT THEY DO AND HOW TO USE THEM
Hairline-F (5% Minoxidil + 0.1% Finasteride Topical)
- Vasodilating blood vessels around follicles (more blood = more nutrients)
- Prolonging the anagen (growth) phase
- Opening potassium channels in follicle cells
- Blocking 5-alpha reductase type II directly at the scalp
- Reducing local DHT without the systemic DHT reduction you get from oral finasteride 1mg
- This means lower risk of the sexual side effects that occur with oral finasteride
PART 3: YOUR COMPLETE DAILY ROUTINE
Morning Routine
| Time | Action |
|---|---|
| After shower | Dry scalp gently by patting (no rough rubbing with towel) |
| Scalp fully dry | Apply Hairline-F to affected areas (parieto-occipital + frontotemporal zones) |
| Wait 30-60 min | Let it absorb before any other hair product |
- Part your hair in sections (even if shaved, use a finger to feel zones)
- Apply 1 mL (roughly 10-12 drops or as per product instruction) directly to scalp - not hair
- Spread with fingertips in gentle circular motion
- Wash your hands after
Evening / Night Routine
- No second application of Hairline-F unless your product label specifically says BD (twice daily). Most topical combo products are once daily.
- If you play volleyball and come back dusty/sweaty: rinse with plain water only - do NOT shampoo twice daily (explained below)
PART 4: SHAMPOO GUIDE - MOST IMPORTANT SECTION FOR YOU
Which Shampoo to Use?
- Ketoconazole is a proven antifungal that also has a mild anti-androgenic effect at the scalp level
- It reduces Malassezia (scalp yeast), which causes inflammation that worsens AGA
- Multiple studies show ketoconazole shampoo reduces hair shedding in AGA patients
- Safe for frequent use in diluted application
- SLS (Sodium Lauryl Sulfate) - strips scalp of protective oils, causes irritation
- Heavy silicones (dimethicone, cyclopentasiloxane) - builds up on scalp, blocks follicles
- Parabens if you have sensitive scalp
- Nizral 2% shampoo (ketoconazole) - use 2-3x per week
- Biotique Bhringraj or Himalaya Anti-Hairfall - for off-days when just rinsing
Washing Frequency - CRITICAL
- Washing twice daily strips natural sebum (scalp oil), making the scalp dry, inflamed, and more susceptible to hair loss
- After volleyball: rinse with plain, cool water only - no shampoo
- Proper shampoo use: 2-3 times per week only
- On other days: plain water rinse after volleyball, pat dry
PART 5: HAIR OIL - WHAT TO USE AND WHEN
Which Oil?
- Mix 2-3 drops of rosemary essential oil in 1 tablespoon of coconut oil or castor oil
- Apply to scalp the night BEFORE you plan to shampoo (not every day)
- Massage gently for 5 minutes with fingertips
- Leave overnight, wash off with ketoconazole shampoo next morning
- Parachute Coconut Oil (base carrier) - very affordable
- Kama Ayurveda Bringha Oil (contains bhringraj + brahmi + rosemary) - effective, mid-range
- Indulekha Bringha Hair Oil - contains light mineral oil + bhringraj - decent
PART 6: COMPLETE WEEKLY SCHEDULE
| Day | Morning | Evening/Night |
|---|---|---|
| Monday | Wash hair with Nizral (ketoconazole) shampoo, dry, apply Hairline-F | Volleyball - water rinse only |
| Tuesday | Apply Hairline-F (no shampoo) | Volleyball - water rinse only |
| Wednesday | Wash with ketoconazole/zinc shampoo, dry, apply Hairline-F | Apply rosemary+coconut oil to scalp |
| Thursday | Wash hair (shampoo), dry, apply Hairline-F | Volleyball - water rinse only |
| Friday | Apply Hairline-F (no shampoo) | Apply rosemary+coconut oil |
| Saturday | Wash hair (shampoo), dry, apply Hairline-F | Volleyball - water rinse |
| Sunday | Apply Hairline-F (no shampoo) | Rest - no oil |
PART 7: DIET AND SUPPLEMENTS FOR HAIR
- Protein: 1.2-1.5g per kg body weight daily - eggs (biotin + protein), chicken, dal, paneer, curd. Hair is made of keratin, a protein.
- Iron-rich foods - spinach, jaggery, rajma, chana - iron deficiency is a common hidden cause of hair fall in young men (even if serum levels borderline normal)
- Zinc - pumpkin seeds, nuts, eggs - zinc is directly involved in hair follicle cycling
- Vitamin D - get 15-20 minutes of sunlight daily (you likely have enough with outdoor volleyball)
- Omega-3 - flaxseeds, walnuts, fish - anti-inflammatory, improves scalp health
PART 8: MASTURBATION AND HAIR LOSS - STRAIGHT ANSWER
- Studies comparing men with normal sexual activity vs. those who abstained found no significant difference in testosterone, free testosterone, or LH levels
- One study actually showed testosterone levels increased after 3 weeks of abstinence - the opposite of what the myth claims
- DHT levels at the scalp are determined by 5-alpha reductase enzyme concentration and genetic follicle sensitivity - not by how often you ejaculate
- It is disrupting your study schedule or sleep
- You feel guilt/shame afterward that lowers your mood
- You are using it as a stress escape mechanism during exam pressure
- Redirect the urge trigger - When the urge comes, do 10-15 push-ups or go for a 5-minute walk. This spikes dopamine through a different pathway and the urge usually passes.
- Fill the time gap - Most urges strike during idle/boredom moments. Keep a study schedule or a sport activity in those slots.
- No guilt spiral - The psychological damage comes from the shame-guilt cycle, not the act itself. One incident is not a problem.
- Sleep hygiene - Many urges happen at night before sleep. Sleep at a fixed time, leave your phone away from bed.
PART 9: RECOVERY TIMELINE - WHAT TO EXPECT
| Timeframe | What Happens |
|---|---|
| Week 1-6 | Possible initial shedding increase from minoxidil - NORMAL, keep going |
| Month 2-3 | Shedding stabilizes, hair fall reduces |
| Month 4-6 | New thin vellus hairs start appearing at treated areas |
| Month 6-12 | Thicker, terminal hairs growing back in the bald patch |
| 1-2 years | Maximum regrowth achieved |
PART 10: SIGNS YOU NEED TO SEE A DOCTOR AGAIN
- Scalp inflammation, redness, or pus (sign of folliculitis - common in red soil players)
- Patchy hair loss in a completely round shape (could be Alopecia Areata - different condition)
- Hair loss spreading to eyebrows/beard
- Side effects from Hairline-F: scalp itching, rash, or unwanted facial hair
- No improvement after 12 months of consistent use - then PRP should be reconsidered
QUICK REFERENCE CARD
DAILY: Hairline-F to scalp (after shower, dry scalp)
SHAMPOO: Nizral 2% ketoconazole - 3x per week only
OIL: Rosemary + coconut oil - 2x/week, night before shampoo day
VOLLEYBALL: Plain water rinse after, NO shampoo
FOOD: High protein + iron + zinc daily
TABLET: Continue Keraglow once daily
MASTURBATION → Hair loss: FALSE. No scientific link exists.
Create a printable daily hair care checklist I can follow as a routine
ls -la /home/daytona/workspace/
mkdir -p /home/daytona/workspace/mayur-haircare
~/mayur-haircare/generate_checklist.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.graphics.shapes import Drawing, Rect, String, Circle
from reportlab.graphics import renderPDF
OUTPUT = "/home/daytona/workspace/mayur-haircare/Mayur_HairCare_Checklist.pdf"
# ── colour palette ──────────────────────────────────────────────────────────
TEAL = colors.HexColor("#1A7A6E")
TEAL_LIGHT = colors.HexColor("#E8F5F3")
TEAL_MID = colors.HexColor("#2DA89A")
ORANGE = colors.HexColor("#E8832A")
ORANGE_LT = colors.HexColor("#FEF3E9")
DARK = colors.HexColor("#1C2833")
GREY_LIGHT = colors.HexColor("#F4F6F7")
GREY_MID = colors.HexColor("#AAB7B8")
WHITE = colors.white
RED_SOFT = colors.HexColor("#E74C3C")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=18*mm,
rightMargin=18*mm,
topMargin=14*mm,
bottomMargin=14*mm,
)
W = A4[0] - 36*mm # usable width
# ── styles ───────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
def style(name, **kw):
s = ParagraphStyle(name, **kw)
return s
S_TITLE = style("title", fontName="Helvetica-Bold", fontSize=20, textColor=WHITE, alignment=TA_CENTER, leading=26)
S_SUB = style("sub", fontName="Helvetica", fontSize=10, textColor=TEAL_LIGHT, alignment=TA_CENTER, leading=14)
S_HEAD = style("head", fontName="Helvetica-Bold", fontSize=11, textColor=TEAL, spaceAfter=2, leading=15)
S_ITEM = style("item", fontName="Helvetica", fontSize=9, textColor=DARK, leading=13, leftIndent=4)
S_SMALL = style("small", fontName="Helvetica", fontSize=8, textColor=GREY_MID, leading=11)
S_TIP = style("tip", fontName="Helvetica-Oblique",fontSize=8, textColor=ORANGE, leading=12, leftIndent=4)
S_WARN = style("warn", fontName="Helvetica-BoldOblique", fontSize=8, textColor=RED_SOFT, leading=12, leftIndent=4)
S_CENTER = style("center", fontName="Helvetica", fontSize=9, textColor=DARK, alignment=TA_CENTER, leading=13)
S_BOLD = style("bold", fontName="Helvetica-Bold", fontSize=9, textColor=DARK, leading=13, leftIndent=4)
S_DAY = style("day", fontName="Helvetica-Bold", fontSize=8, textColor=WHITE, alignment=TA_CENTER, leading=12)
S_CELL = style("cell", fontName="Helvetica", fontSize=7.5,textColor=DARK, leading=11)
S_FOOTER = style("footer", fontName="Helvetica", fontSize=7.5,textColor=GREY_MID, alignment=TA_CENTER, leading=11)
def checkbox_row(label, note="", bold=False):
"""Returns a 1-row table with a checkbox square + label + optional note."""
box = Table([[""]], colWidths=[4.5*mm], rowHeights=[4.5*mm])
box.setStyle(TableStyle([
("BOX", (0,0),(0,0), 1, TEAL_MID),
("BACKGROUND", (0,0),(0,0), TEAL_LIGHT),
("VALIGN", (0,0),(0,0), "MIDDLE"),
]))
st = S_BOLD if bold else S_ITEM
txt = Paragraph(label, st)
note_cell = Paragraph(note, S_TIP) if note else Paragraph("", S_SMALL)
row = Table([[box, txt, note_cell]], colWidths=[7*mm, W*0.54, W*0.38])
row.setStyle(TableStyle([
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("LEFTPADDING",(0,0),(-1,-1), 0),
("RIGHTPADDING",(0,0),(-1,-1), 2),
("TOPPADDING", (0,0),(-1,-1), 1),
("BOTTOMPADDING",(0,0),(-1,-1), 1),
]))
return row
def section_header(title, emoji=""):
bg = Table([[Paragraph(f"{emoji} {title}", S_HEAD)]], colWidths=[W])
bg.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), TEAL_LIGHT),
("LEFTPADDING", (0,0),(0,0), 6),
("RIGHTPADDING",(0,0),(0,0), 6),
("TOPPADDING", (0,0),(0,0), 4),
("BOTTOMPADDING",(0,0),(0,0), 4),
("ROUNDEDCORNERS", (0,0),(0,0), [3,3,3,3]),
]))
return bg
def divider():
return HRFlowable(width=W, thickness=0.5, color=TEAL_LIGHT, spaceAfter=4, spaceBefore=4)
# ── BANNER ───────────────────────────────────────────────────────────────────
banner = Table(
[[Paragraph("MAYUR'S DAILY HAIR CARE CHECKLIST", S_TITLE)],
[Paragraph("Androgenetic Alopecia (AGA) Management | Norwood Type IVa | Personalised Routine", S_SUB)]],
colWidths=[W]
)
banner.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,1), TEAL),
("LEFTPADDING", (0,0),(0,1), 10),
("RIGHTPADDING", (0,0),(0,1), 10),
("TOPPADDING", (0,0),(0,0), 10),
("BOTTOMPADDING",(0,0),(0,0), 2),
("TOPPADDING", (0,1),(0,1), 2),
("BOTTOMPADDING",(0,1),(0,1), 10),
]))
# ── DATE BAR ─────────────────────────────────────────────────────────────────
date_bar = Table(
[[Paragraph("Date: ___________________", S_CENTER),
Paragraph("Week No.: ______", S_CENTER),
Paragraph("Day: Mon / Tue / Wed / Thu / Fri / Sat / Sun", S_CENTER)]],
colWidths=[W*0.35, W*0.2, W*0.45]
)
date_bar.setStyle(TableStyle([
("BOX", (0,0),(-1,-1), 0.5, GREY_MID),
("INNERGRID", (0,0),(-1,-1), 0.5, GREY_MID),
("BACKGROUND", (0,0),(-1,-1), GREY_LIGHT),
("LEFTPADDING", (0,0),(-1,-1), 6),
("RIGHTPADDING", (0,0),(-1,-1), 6),
("TOPPADDING", (0,0),(-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
]))
# ── SHAMPOO DAY? ─────────────────────────────────────────────────────────────
shampoo_bar = Table(
[[Paragraph("Is today a SHAMPOO day?", S_BOLD),
Paragraph(" YES (Mon / Wed / Fri)", S_ITEM),
Paragraph(" NO (Tue / Thu / Sat / Sun)", S_ITEM)]],
colWidths=[W*0.3, W*0.33, W*0.37]
)
shampoo_bar.setStyle(TableStyle([
("BOX", (0,0),(-1,-1), 0.8, ORANGE),
("INNERGRID", (0,0),(-1,-1), 0.5, ORANGE),
("BACKGROUND", (0,0),(0,0), ORANGE_LT),
("LEFTPADDING", (0,0),(-1,-1), 6),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
]))
# ── MORNING ROUTINE ──────────────────────────────────────────────────────────
morning_items = [
("Wake up & drink 1 glass of water (250 mL)", "Hydration = scalp health"),
("Take Keraglow tablet with breakfast", "Once daily, after food"),
("— IF SHAMPOO DAY —", "", True),
("Wet scalp with lukewarm (not hot) water", "Hot water damages follicles"),
("Apply Nizral / ketoconazole 2% shampoo to scalp", "Leave 2-3 min, then rinse"),
("Rinse thoroughly — no residue left behind", "Residue blocks follicles"),
("Pat dry with a soft towel — NO rubbing", "Rubbing breaks fragile hairs"),
("— ALL DAYS (after shower / after drying) —", "", True),
("Ensure scalp is fully dry before applying Hairline-F", "Wet scalp = poor absorption"),
("Apply Hairline-F (1 mL) to parieto-occipital bald patch", "Use fingertip / dropper"),
("Apply Hairline-F to parieto-temporal recession zones", "Spread gently, don't rub hard"),
("Massage lightly for 1-2 min with fingertips", "Improves blood flow"),
("Wash hands immediately after application", "Prevent accidental eye contact"),
("Wait 30-60 minutes before any styling / going out", "Allow full absorption"),
]
# ── AFTERNOON / VOLLEYBALL ───────────────────────────────────────────────────
afternoon_items = [
("Drink water every 30 min during volleyball (≥ 500 mL/game)", "Dehydration stresses follicles"),
("Wear a light cotton bandana / cap if playing in strong sun", "UV + heat = scalp damage"),
("After volleyball: rinse scalp with plain COOL water only", "NO shampoo — water only"),
("Pat dry with clean towel — do NOT scratch/rub scalp", "Red soil particles irritate scalp"),
("Check scalp for any redness, boils, or tenderness", "Early sign of folliculitis — see doctor if present"),
]
# ── EVENING / NIGHT ──────────────────────────────────────────────────────────
evening_items = [
("Eat a protein-rich dinner (eggs / dal / paneer / chicken)", "≥ 1.2g protein per kg body weight"),
("— IF OIL NIGHT (Wed night & Fri night) —", "", True),
("Mix 2-3 drops rosemary essential oil in 1 tbsp coconut oil", "In palm, mix well"),
("Apply oil blend to scalp (NOT to hair length)", "Target follicle roots only"),
("Massage for 5 min in circular motions with fingertips", "Improves dermal papilla blood flow"),
("Leave overnight — wash off with ketoconazole shampoo next morning", "DO NOT apply Hairline-F on oil night"),
("— ALL EVENINGS —", "", True),
("Drink 1 more glass of water before sleep", "Total target: 3 L/day"),
("Sleep for 7-8 hours at a fixed time", "Growth hormone (hair regrowth) peaks during sleep"),
("Keep phone away from bed to avoid late-night urge triggers", "Sleep hygiene = hormone regulation"),
]
# ── WEEKLY SUMMARY TABLE ──────────────────────────────────────────────────────
days = ["Mon", "Tue", "Wed", "Thu", "Fri", "Sat", "Sun"]
shampoo = ["YES", "No", "YES", "YES", "No", "YES", "No"]
hairlinef= ["YES","YES", "YES", "YES", "YES","YES","YES"]
oil = ["No", "No", "Night","No","Night","No","No"]
kera = ["YES","YES", "YES", "YES", "YES","YES","YES"]
header_row = [Paragraph(d, S_DAY) for d in ["", "Mon","Tue","Wed","Thu","Fri","Sat","Sun"]]
row1 = [Paragraph("Shampoo\n(Nizral)", S_CELL)] + [Paragraph(v, S_CELL) for v in shampoo]
row2 = [Paragraph("Hairline-F", S_CELL)] + [Paragraph(v, S_CELL) for v in hairlinef]
row3 = [Paragraph("Scalp Oil\n(Night)", S_CELL)] + [Paragraph(v, S_CELL) for v in oil]
row4 = [Paragraph("Keraglow\nTablet", S_CELL)] + [Paragraph(v, S_CELL) for v in kera]
col_w = [W*0.165] + [W*0.119]*7
weekly = Table([header_row, row1, row2, row3, row4], colWidths=col_w)
cell_style = [
("BACKGROUND", (0,0),(-1,0), TEAL),
("TEXTCOLOR", (0,0),(-1,0), WHITE),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0),(-1,-1), 8),
("ALIGN", (0,0),(-1,-1), "CENTER"),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("GRID", (0,0),(-1,-1), 0.5, GREY_MID),
("BACKGROUND", (0,1),(0,-1), GREY_LIGHT),
("TOPPADDING", (0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
]
# colour YES cells green, No cells grey, Night cells orange
for r in range(1, 5):
for c in range(1, 8):
val = [shampoo, hairlinef, oil, kera][r-1][c-1]
if val == "YES":
cell_style.append(("BACKGROUND", (c,r),(c,r), colors.HexColor("#D5F5E3")))
cell_style.append(("TEXTCOLOR", (c,r),(c,r), colors.HexColor("#1E8449")))
cell_style.append(("FONTNAME", (c,r),(c,r), "Helvetica-Bold"))
elif val == "Night":
cell_style.append(("BACKGROUND", (c,r),(c,r), ORANGE_LT))
cell_style.append(("TEXTCOLOR", (c,r),(c,r), ORANGE))
cell_style.append(("FONTNAME", (c,r),(c,r), "Helvetica-Bold"))
elif val == "No":
cell_style.append(("TEXTCOLOR", (c,r),(c,r), GREY_MID))
weekly.setStyle(TableStyle(cell_style))
# ── IMPORTANT REMINDERS BOX ──────────────────────────────────────────────────
reminders = [
("NEVER shampoo twice daily — strips scalp oils", RED_SOFT),
("Initial shedding with Hairline-F (weeks 1-6) is NORMAL — keep going", ORANGE),
("On oil nights — skip Hairline-F application", ORANGE),
("Masturbation does NOT cause hair loss — confirmed by science", TEAL_MID),
("AGA treatment is lifelong — stopping = hair loss returns in ~12 months", RED_SOFT),
("If scalp shows redness / pus / pain — see a dermatologist immediately", RED_SOFT),
]
reminder_rows = []
for text, col in reminders:
s = ParagraphStyle("rem", fontName="Helvetica-Bold" if col==RED_SOFT else "Helvetica",
fontSize=8, textColor=col, leading=12, leftIndent=6)
reminder_rows.append([Paragraph(f"⚑ {text}", s)])
rem_table = Table(reminder_rows, colWidths=[W])
rem_table.setStyle(TableStyle([
("BOX", (0,0),(0,-1), 0.8, TEAL),
("LEFTPADDING", (0,0),(0,-1), 6),
("RIGHTPADDING", (0,0),(0,-1), 6),
("TOPPADDING", (0,0),(0,-1), 3),
("BOTTOMPADDING",(0,0),(0,-1), 3),
("BACKGROUND", (0,0),(0,-1), GREY_LIGHT),
("LINEBELOW", (0,0),(0,-2), 0.3, GREY_MID),
]))
# ── PROGRESS TRACKER ─────────────────────────────────────────────────────────
weeks = [f"Week {i}" for i in range(1, 13)]
prog_headers = [Paragraph(w, S_DAY) for w in ["Month/Week"] + weeks]
prog_row1 = [Paragraph("Hair fall\n(1=less, 5=heavy)", S_CELL)] + [Paragraph("___", S_CELL)] * 12
prog_row2 = [Paragraph("New growth\n(Yes/No)", S_CELL)] + [Paragraph("___", S_CELL)] * 12
prog_row3 = [Paragraph("Scalp\nhealth (1-5)", S_CELL)] + [Paragraph("___", S_CELL)] * 12
col_w2 = [W*0.165] + [W*(0.835/12)]*12
tracker = Table([prog_headers, prog_row1, prog_row2, prog_row3], colWidths=col_w2)
tracker.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,0), TEAL_MID),
("TEXTCOLOR", (0,0),(-1,0), WHITE),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0),(-1,-1), 7),
("ALIGN", (0,0),(-1,-1), "CENTER"),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("GRID", (0,0),(-1,-1), 0.4, GREY_MID),
("BACKGROUND", (0,1),(0,-1), GREY_LIGHT),
("TOPPADDING", (0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
]))
# ── FOOTER ───────────────────────────────────────────────────────────────────
footer = Paragraph(
"Prepared by Orris AI | Based on: Dermatology 2-Vol Set 5e (Elsevier), Fitzpatrick's Dermatology, Andrews' Diseases of Skin | "
"For: Mayur Lokhande, 23M, AGA Norwood IVa | Print & laminate for daily use",
S_FOOTER
)
# ── ASSEMBLE DOCUMENT ─────────────────────────────────────────────────────────
def build_section(title, emoji, items):
elems = [section_header(title, emoji), Spacer(1, 3)]
for item in items:
if len(item) == 3 and item[2]: # sub-header row
row = Table(
[[Paragraph(item[0], ParagraphStyle("sh", fontName="Helvetica-BoldOblique",
fontSize=8.5, textColor=ORANGE, leading=12, leftIndent=4))]],
colWidths=[W]
)
row.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), ORANGE_LT),
("LEFTPADDING", (0,0),(0,0), 6),
("TOPPADDING", (0,0),(0,0), 2),
("BOTTOMPADDING",(0,0),(0,0), 2),
]))
elems.append(row)
else:
elems.append(checkbox_row(item[0], item[1] if len(item) > 1 else ""))
return elems
story = []
story.append(banner)
story.append(Spacer(1, 5))
story.append(date_bar)
story.append(Spacer(1, 4))
story.append(shampoo_bar)
story.append(Spacer(1, 6))
# Morning
story += build_section("MORNING ROUTINE", "☀", morning_items)
story.append(Spacer(1, 6))
# Afternoon
story += build_section("AFTERNOON / VOLLEYBALL", "🏐", afternoon_items)
story.append(Spacer(1, 6))
# Evening
story += build_section("EVENING & NIGHT ROUTINE", "🌙", evening_items)
story.append(Spacer(1, 6))
# Weekly schedule
story.append(section_header("WEEKLY SCHEDULE AT A GLANCE", "📅"))
story.append(Spacer(1, 3))
story.append(weekly)
story.append(Spacer(1, 6))
# Reminders
story.append(section_header("IMPORTANT REMINDERS", "⚠"))
story.append(Spacer(1, 3))
story.append(rem_table)
story.append(Spacer(1, 6))
# Progress tracker
story.append(section_header("12-WEEK PROGRESS TRACKER", "📈"))
story.append(Spacer(1, 3))
story.append(tracker)
story.append(Spacer(1, 8))
story.append(divider())
story.append(footer)
doc.build(story)
print(f"PDF generated: {OUTPUT}")
cd /home/daytona/workspace/mayur-haircare && python generate_checklist.py 2>&1
ls -lh /home/daytona/workspace/mayur-haircare/
Mayur HairCare Checklist
PDF Document · PDF
- Morning Routine - Keraglow tablet, shampoo (if applicable), drying technique, Hairline-F application steps
- Afternoon / Volleyball - Hydration, sun protection, post-play water rinse, scalp inspection
- Evening & Night - Protein meal reminder, oil application routine (Wed & Fri nights), sleep hygiene