Vonoprazon
Reading File
Searching PubMed
vonoprazan
Finding Sources
Reading Article
PMID: 38388872
Reading Article
PMID: 39145848
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of vonoprazan drawn from multiple authoritative textbooks and recent literature.
Vonoprazan (Voquezna®)
Class & Chemical Identity
Vonoprazan is a potassium-competitive acid blocker (P-CAB) - a newer class of gastric antisecretory agents distinct from proton pump inhibitors (PPIs). Chemically it is a pyrrole derivative (fumarate salt), shown below alongside the other P-CABs:
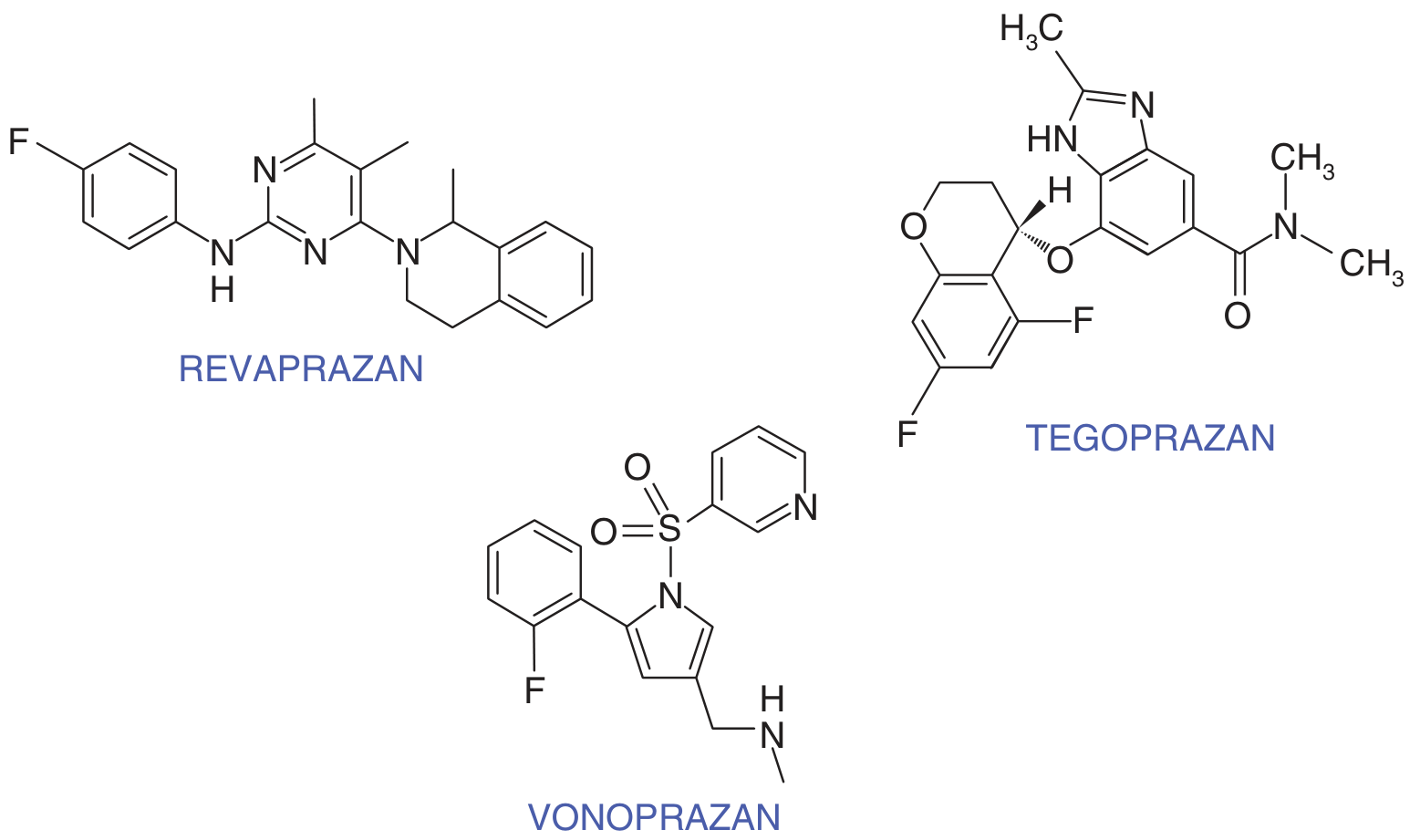
Figure: Chemical structures of potassium-competitive acid blockers - Goodman & Gilman's Pharmacological Basis of Therapeutics
Mechanism of Action
Vonoprazan inhibits the parietal cell H⁺/K⁺-ATPase (proton pump) by competitively blocking the potassium-binding site - hence "K⁺-competitive." This is fundamentally different from PPIs:
| Feature | PPIs | Vonoprazan (P-CAB) |
|---|---|---|
| Activation | Requires acid-catalyzed activation (prodrug) | No acid activation needed - acid stable |
| Food effect | Must be taken before meals | No food restriction |
| Onset | 3-5 days to maximum effect | Day 1 (near-maximal from first dose) |
| Duration | Effect tied to CYP2C19 metabolism | Slow dissociation from pump - 24h effect |
| CYP dependence | Mainly CYP2C19 (genetic polymorphism) | Mainly CYP3A4/5 - less interindividual variability |
| pKa | ~4 | ~9 (highly basic, accumulates in canaliculi) |
Because it does not need acidic activation, vonoprazan works equally well regardless of meal timing and achieves consistent acid suppression even in CYP2C19 rapid metabolizers - a population where PPIs often underperform.
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, p. 892
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1097
Pharmacokinetics (ADME)
- Absorption: Rapidly absorbed; peak plasma concentration ~2 hours; unaffected by food
- Distribution: High pKa (9) promotes accumulation in the acidic secretory canaliculus of the parietal cell
- Metabolism: Primarily hepatic via CYP3A4/5 (unlike PPIs which use CYP2C19)
- Elimination half-life: ~7 hours (range across P-CABs: 2-9 h)
- Duration of effect: Up to 24 hours per dose due to slow dissociation from H⁺/K⁺-ATPase
Approved Indications
Japan (original approval):
- Gastroduodenal ulcers (healing)
- Erosive esophagitis (healing and maintenance)
- Gastric protection in NSAID/low-dose aspirin users
- H. pylori eradication
USA (FDA approval - more recent):
- H. pylori infection in adults - in combination with:
- Vonoprazan + amoxicillin (dual therapy), OR
- Vonoprazan + amoxicillin + clarithromycin (triple therapy)
- Erosive esophagitis (healing and maintenance)
- Dose range: 10-20 mg daily
Harrison's notes that vonoprazan received FDA Fast Track status for H. pylori treatment based on the pivotal PHALCON-HP trial conducted in the USA and Europe.
- Harrison's Principles of Internal Medicine, 22nd Ed.
- Shirley M, Drugs 2024 (PMID 38388872)
Clinical Efficacy
Peptic Ulcer Disease
In two phase 3 RCTs, vonoprazan 20 mg once daily was non-inferior to lansoprazole 30 mg once daily for healing both gastric ulcers (GU, 8 weeks) and duodenal ulcers (DU, 6 weeks). Vonoprazan 10 mg and 20 mg were equally effective as lansoprazole 15 mg for preventing ulcer recurrence in long-term NSAID and low-dose aspirin users.
GERD / Erosive Esophagitis
Vonoprazan was non-inferior to PPIs for healing erosive esophagitis. A 2024 network meta-analysis (PMID 38345252) found P-CABs (including vonoprazan) had superior efficacy over PPIs for severe (Grade C/D) esophagitis.
H. pylori Eradication
This is where vonoprazan may offer the clearest advantage over PPIs. Since sustained acid suppression is critical for antibiotic stability and efficacy, vonoprazan's consistent and potent suppression translates into higher eradication rates - particularly in clarithromycin-resistant strains and CYP2C19 rapid metabolizers.
Adverse Effects
Generally well tolerated, with a short-term safety profile overlapping PPIs. Most frequent adverse effects in clinical trials:
- Diarrhea
- Nasopharyngitis
- Dyspepsia
- Headache
- Abdominal pain
Longer-term concerns (shared with PPIs, potentially amplified):
- Hypergastrinemia: Serum gastrin levels 1.5-2x higher than with PPIs due to more profound acid suppression; ECL cell hyperplasia observed in animals and humans - significance for carcinoid development in humans is not yet established
- Gut microbiome changes and risk of bacterial overgrowth have been reported
- Renal H⁺/K⁺-ATPase inhibition in medullary collecting ducts - clinical significance unknown
- Long-term safety data are still accumulating
Comparison with PPIs: Key Advantages
- No prodrug activation - works immediately on the first dose
- Food-independent absorption and action
- Less CYP2C19 polymorphism effect - more consistent across patients
- Faster and more sustained acid suppression
- Better H. pylori eradication - particularly in drug-resistant cases
Current Landscape (2024-2026)
A 2024 review by Scarpignato & Hunt (PMID 39145848) identifies four P-CABs now available globally: vonoprazan, tegoprazan, fexuprazan, and keverprazan. Of these, only vonoprazan is approved outside Asia for use in the Americas. Two more compounds (linazapran glurate and zestaprazan) are in clinical development. The 2025 Italian GERD guidelines (PMID 40450492) incorporate P-CABs into management algorithms, reflecting growing acceptance in Western practice.
Summary: Vonoprazan represents a genuine advance over PPIs for acid-related disease - offering faster onset, food-independent dosing, reduced metabolic variability, and superior H. pylori eradication. Its long-term safety profile, particularly around hypergastrinemia and microbiome effects, requires continued surveillance.
This is a shared conversation. Sign in to Orris to start your own chat.