SSPE , detail from standees textbook and article
Reading File
Finding Sources
Searching PubMed
subacute sclerosing panencephalitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. The user likely meant Adams and Victor's Principles of Neurology (often abbreviated "Adams & Victor" — commonly called a "standee" style classic reference). Let me compile the full answer.
Subacute Sclerosing Panencephalitis (SSPE)
Overview & Historical Background
SSPE was first described by Dawson in 1934 as "inclusion body encephalitis" and later renamed by Van Bogaert. It is now established as a chronic measles virus infection of the CNS — a rare late complication occurring in immunocompetent individuals. The condition is a rare, chronic, progressive demyelinating disease caused by persistent non-permissive (non-productive) measles virus infection of neurons and glia.
Adams and Victor's Principles of Neurology, 12th Ed. | Bradley and Daroff's Neurology in Clinical Practice | Harrison's 22E
Epidemiology
| Parameter | Detail |
|---|---|
| Incidence | ~1 per 1,000,000 children/year (vaccinated populations); up to 5–6/million in unimmunized |
| Frequency | 1 in 100,000–500,000 measles cases |
| Age | 85% aged 5–15 years at diagnosis |
| Sex | Male:Female ratio 3:1 |
| Latent period | Median 8 years (range 2–12 years) after primary measles |
| Trigger | Primary measles infection typically before age 2 years |
SSPE has practically disappeared in vaccinated populations, though vaccine hesitancy and rising measles cases threaten a resurgence. — Harrison's 22E
Pathogenesis
The virus is defective: aberrant Matrix (M) protein, along with other envelope proteins, interferes with viral assembly and budding. As a result:
- The virus cannot form infectious particles and remains intracellular
- It spreads cell-to-cell rather than by free virions
- This conceals it from immune clearance despite high antibody titers
This explains why SSPE develops in immunocompetent children — the virus is not killed because it is never fully exposed to humoral or cellular immunity. Early infection before age 2, when immune responses are immature, may facilitate initial viral persistence.
— Bradley and Daroff's Neurology in Clinical Practice
Clinical Stages
Stage I — Behavioural/Cognitive
- Declining school performance
- Personality and mood changes, temper outbursts
- Language difficulties, loss of interest in activities
Stage II — Neurological Deterioration
- Severe progressive intellectual deterioration
- Myoclonus (often "slow" — characteristic of SSPE)
- Focal or generalized seizures
- Ataxia
- Chorioretinitis / visual disturbances
- Choreoathetoid or ballistic movements
Stage III — Terminal
- Rigidity, hyperactive reflexes, Babinski signs
- Optic atrophy, quadriparesis
- Autonomic instability
- Akinetic mutism, progressive unresponsiveness
- Ultimately: decorticate state, coma
Course: Steadily progressive; death within 1–3 years in most cases. Spontaneous remissions occur in ~5%.
Diagnostic Studies
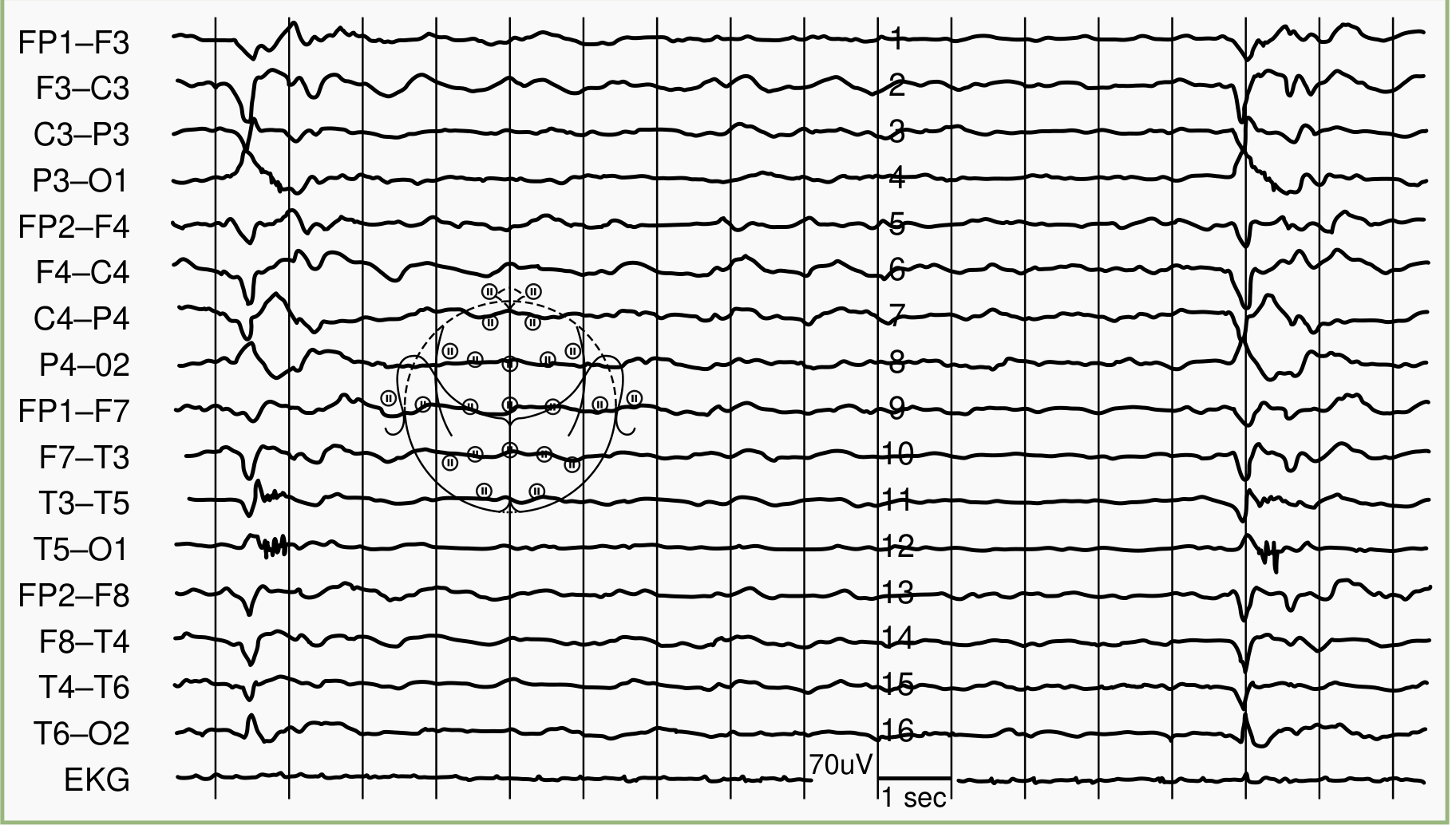
EEG
Pathognomonic pattern: Periodic bursts of 2–3 Hz high-voltage sharp/slow waves occurring at regular intervals of every 3–8 seconds (up to 4–14 seconds apart), against a background of attenuated ("flat") activity. The bursts may last up to 3 seconds.
CSF
- Acellular (no pleocytosis)
- Glucose: normal
- Total protein: normal or mildly elevated
- Gamma globulin markedly elevated (>20% of total CSF protein)
- Oligoclonal IgG bands on gel electrophoresis — measles-virus-specific antibody
- Elevated CSF antimeasles antibody — invariably present; consistent with high intrathecal synthesis
- CSF/serum antibody ratio confirms intrathecal synthesis
MRI
- Early: often normal
- As disease progresses: high T2 signal intensity in posterior gray and subcortical white matter
- Spreads to periventricular white matter in later stages
Serology
- Elevated serum antimeasles antibody titers in all cases
Virology
- Measles virus can be cultured from brain by cocultivation techniques
- Viral antigen detectable immunocytochemically
- Viral genome detectable by in situ hybridization or PCR
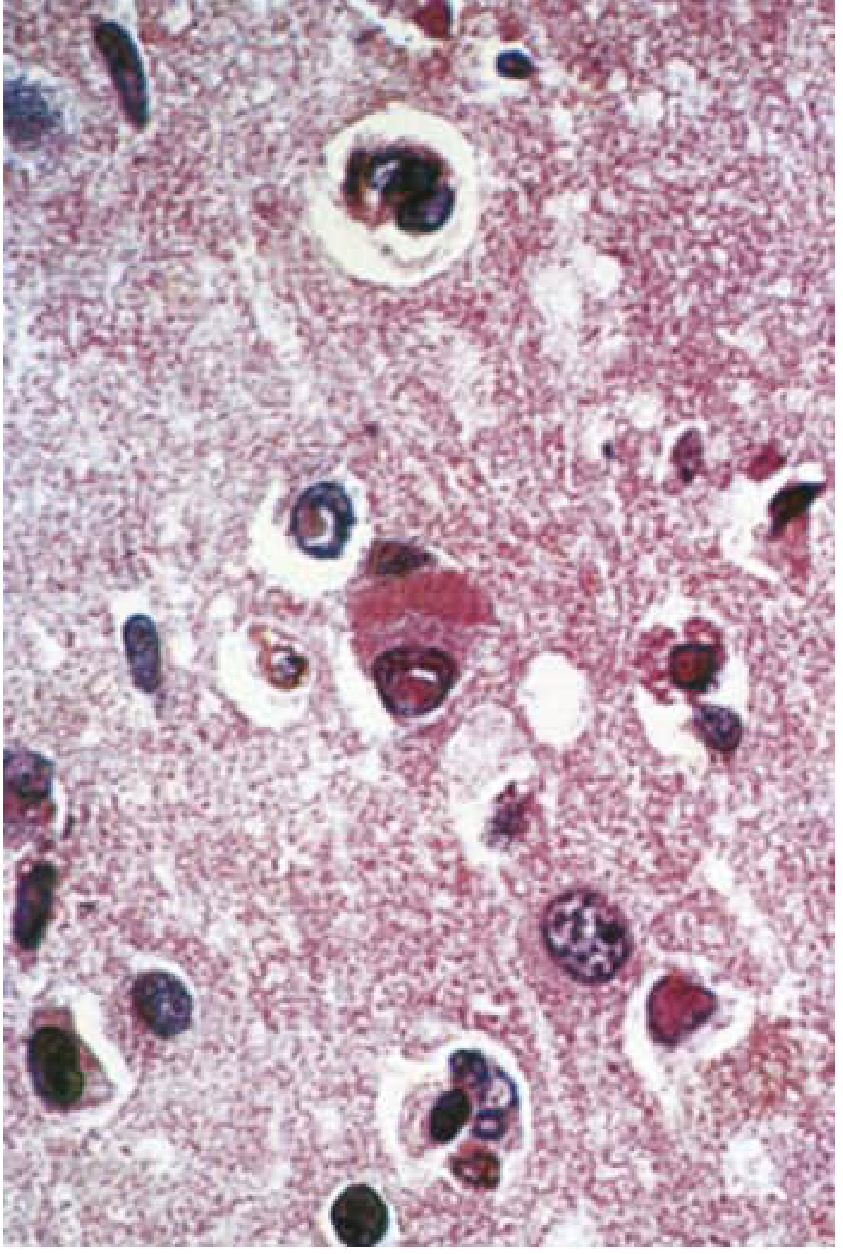
Histopathology
Lesions involve the cerebral cortex and white matter of both hemispheres and the brainstem. The cerebellum is usually spared.
Key findings:
- Eosinophilic intranuclear and intracytoplasmic inclusion bodies (Cowdry Type A) in neurons and glial cells — the histopathological hallmark
- Destruction of nerve cells, neuronophagia
- Perivascular cuffing by lymphocytes and mononuclear cells
- White matter: degeneration of myelinated fibers (both myelin and axons) + fibrous gliosis → "sclerosing encephalitis"
- Electron microscopy: measles nucleocapsids in inclusion-bearing cells
Differential Diagnosis
(Adams & Victor)
| Condition | Distinguishing Features |
|---|---|
| Lipid storage diseases (Tay-Sachs, etc.) | Enzyme assays, cherry-red spot; no measles antibodies |
| Prion disease (CJD) | Older age, no measles antibodies, 14-3-3 protein in CSF |
| Schilder-type demyelinating disease | MRI pattern, no measles antibodies |
| Subacute measles encephalitis (immunosuppressed) | Short interval 1–6 months post measles; no antibody rise; lacks inflammation on histology |
Treatment
No definitive curative therapy exists.
| Regimen | Details |
|---|---|
| Isoprinosine (Inosiplex) | 100 mg/kg/day orally (max 3 g/day) in 3 divided doses × 6 months; first-line oral agent |
| Intraventricular interferon-α | Via Ommaya reservoir: starting 100,000 U/m² BSA/day → escalating to 10⁶ U/m²/day over 5 days, then 10⁶ U/m² twice weekly × 6 months |
| Combination (IFN-α + Isoprinosine) | ~30–35% of patients show improvement or stabilization |
| IV ribavirin + intrathecal IFN-α | Some reported benefit |
| Levetiracetam | Symptomatic improvement in myoclonus and encephalopathy reported |
| Subcutaneous IFN-α | Up to 5 million units/day — to treat peripheral reservoirs (lymphoid, glandular tissue) |
Laboratory endpoint of treatment: Eradication of detectable measles antigen from CSF.
Risks of treatment: Meningitis, interferon-induced encephalopathy, upper and lower motor neuron toxicity from IFN-α.
Amantadine and inosine pranobex have been tried; effects have not been corroborated in controlled trials. — Adams & Victor
Prevention
Measles vaccination is the only proven prevention.
- MMR (measles-mumps-rubella) or MMRV vaccine
- First dose: 12–15 months of age
- Second dose: 4–6 years of age
SSPE has practically disappeared in countries with high MMR coverage. Vaccine hesitancy is expected to drive a resurgence.
Recent Literature (2023–2024)
Recent systematic reviews highlight specific clinical features of SSPE:
- Vision loss in SSPE [Garg et al., 2023 — PMID 37160278]: Chorioretinitis and optic atrophy are significant causes of visual morbidity.
- Hyperkinetic and hypokinetic movement disorders in SSPE [Garg et al., 2024 — PMID 38765932]: Myoclonus, dystonia, chorea, and parkinsonism all described.
- Movement disorders in SSPE [Garg D et al., 2024 — PMID 38748762]: A broad spectrum of hyperkinetic and hypokinetic movements are recognized, broader than classically taught.
Sources:
- Adams and Victor's Principles of Neurology, 12th Edition, p. 774–775
- Bradley and Daroff's Neurology in Clinical Practice, pp. 1678–1679
- Harrison's Principles of Internal Medicine 22E (2025), p. 1161
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.